
Abstract
Background:
It has been demonstrated that ultrasound (US)-guided renal collecting system access during percutaneous nephrolithotomy (PCNL) is efficient and secure. The puncture success rate fell to 82%, and the total complication rate rose to 15% in kidneys with nondilated collecting systems. Contrast-enhanced ultrasonography (CEUS) has been used in PCNL techniques to address this issue.
Methods:
We did this meta-analysis following the preferred reporting criteria for systematic reviews and meta-analysis to combine the data of published studies to compare the CEUS-guided PCNL and the standard US-guided PCNL (PRISMA). For relevant literature, we searched PubMed, Embase, Web of Science, CKNI, and the Cochrane Library. The final inclusion date for this meta-analysis was May 1, 2022, and three randomized controlled trials (RCTs) were finally included. RevMan V5.4.1 was used in this work. Standard mean difference (SMD) with a 95% confidence interval (CI) was utilized as the major estimate in the synthesis of continuous data, while odds ratio (OR) with a 95% CI was synthesized as the main estimate in the synthesis of discontinuous data.
Results:
We found that compared with traditional US-guided PCNL, CEUS-guided PCNL could offer more benefits in terms of single-needle success rate (OR: 3.02, 95% CI: 1.62 to 5.61, p = 0.0005), shorter puncture time (SMD: −1.33, 95% CI: −2.06 to −0.60, p = 0.0004), shorter hospital stays (SMD: −0.37, 95% CI: −0.60 to −0.13, p = 0.002), and a better stone clearance rate (OR: 2.32, 95% CI: 1.15 to 4.68. p = 0.02). Although the PCNL complication rate after surgery was not significantly reduced by the CEUS technique (overall complication: OR = 0.70, 95% CI: 0.37 to 1.30, p = 0.25. Grade 1/2 complication: OR = 0.79, 95% CI: 0.41 to 1.53, p = 0.48; Grade 3/4 complication: OR = 0.44, 95% CI: 0.10 to 1.98, p = 0.28), it could reduce hemoglobin dropping compared with conventional US-guided PCNL (SMD: −0.82, 95% CI: −1.06 to −0.58, p < 0.001).
Conclusion:
The CEUS-guided PCNL technique is superior to the US-guided PCNL, according to almost all synthesized data. Additional randomized studies are still required.
Introduction
One of the gold standards for treating patients with large (>2 cm) or difficult upper urinary tract stones is percutaneous nephrolithotomy (PCNL). 1 The most crucial and challenging stage of the PCNL is to create accurate tracts for the renal collecting system. 1 Kidney, ureter, and bladder radiograph (KUB) fluoroscopy is typically used to guide the establishment of the PCNL tracts. However, there is a risk of KUB radiation exposure, and the surgeon may make a mistake based on the two-dimensional planar image. 2
The efficacy and safety of ultrasound (US)-guided renal collecting access systems in PCNL have been satisfactorily demonstrated. 3 Real-time needle entrance channel monitoring and the ability to prevent renal vascular injury thanks to color Doppler flow imaging are the key benefits of US-guided renal puncture. 4,5 However, access to the renal collecting system without hydronephrosis is a significant technologic difficulty for US-guided PCNL. According to previously published research, a US-guided renal puncture can effectively access 96.6% to 100% of kidneys with dilated renal collecting systems brought on by hydronephrosis with little problems. The success rate of puncture fell to 82% in kidneys with nondilated collecting systems, while the overall complication rate rose to 15%. 6
Due to the use of a contrast agent, contrast-enhanced ultrasonography (CEUS) has superior imaging capabilities to standard US. 7 The use of CEUS technology in PCNL may be promising, given its benefits in avoiding radiation and minimizing problems. Recent randomized controlled trials (RCTs) indicated that CEUS-guided PCNL was significantly more effective and safer than conventional US-guided PCNL. 8 However, higher level evidence-based medical literature is currently lacking to justify CEUS's replacement of US as the principal US guidance technique for establishing PCNL tracts. This study aims to compare the CEUS-guided PCNL and the traditional US-guided PCNL by combining the data from existing studies.
Materials and Methods
According to the standard reporting items for systematic reviews and meta-analyses, this review and analysis were conducted (PRISMA). 9 Five major databases—PubMed, Embase, Web of Science, CKNI, and Cochrane Library—were searched to find prospective candidate studies. The search terms were CEUS and PCNL. Each candidate article's reference was reviewed to locate any candidate-published research. Date of most recent search: May 1, 2022.
This systematic review and meta-analysis used the PICO principles as inclusion and exclusion criteria. 10
Population: Kidney stone patients with nondilated collecting system treated with PCNL.
Intervention: CEUS guiding system should be applied.
Comparison: CEUS guiding system compared with conventional US guiding system.
Outcomes: Outcomes concerned about efficacy and safety should be reported.
Study design: This systematic review and meta-analysis should include only RCTs.
The detailed baseline parameters should be reported for pooling to assess baseline differences in the meta-analysis, according to the detailed results. It is important to report primary efficacy outcomes such as single-needle puncture success rate, puncture time, operation time, and hospital stay. It was decided to use the stone clearance rate as a secondary efficacy outcome. The complication and hemoglobin falling data were needed for pooling for safety evaluation. Only studies published in English (or English abstract offered) and as a journal article were included in this work.
The data extraction and literature review were carried out independently by two authors. The included RCTs were subjected to quality control using Cochrane methods. The data pooling and analysis were conducted by using RevMan 5.4.1. The threshold for statistical significance was a two-tailed p < 0.05. Standard mean difference (SMD) with a 95% confidence interval (CI) was utilized as the major estimate in the synthesis of continuous data, while odds ratio (OR) with a 95% CI was calculated and synthesized as the main estimate in the synthesis of discontinuous data. Both the Q test and I 2 index were used to assess heterogeneity. A random-effect model for pooling was used when significant heterogeneity was found and p < 0.05 in the Q test and I 2 was greater than 50%.
Sensitive and subgroup analyses were carried out to provide further details on identifying the source of heterogeneity. The primary findings were displayed using forest plots. The Egger test, the Begg test, and the funnel plots were used to measure publication bias.
Results
After the literature screening and quality control, the original data extracted from three RCTs were included in this systematic review and meta-analysis. 8,11,12 Figure 1 displays the detailed flowchart. All RCTs offered efficacy and safety outcomes; there were 286 patients (144 for CEUS-guided PCNL and 142 for US-guided PCNL) included in the quantitative analysis. Table 1 provides detailed information about the included studies. The quality and risk-of-bias assessment results for included RCTs were conducted with Cochrane tools (Supplementary Fig. S1). The main possible bias was performance bias (blinding participants and personnel, which was impossible for RCTs conducted in surgery).
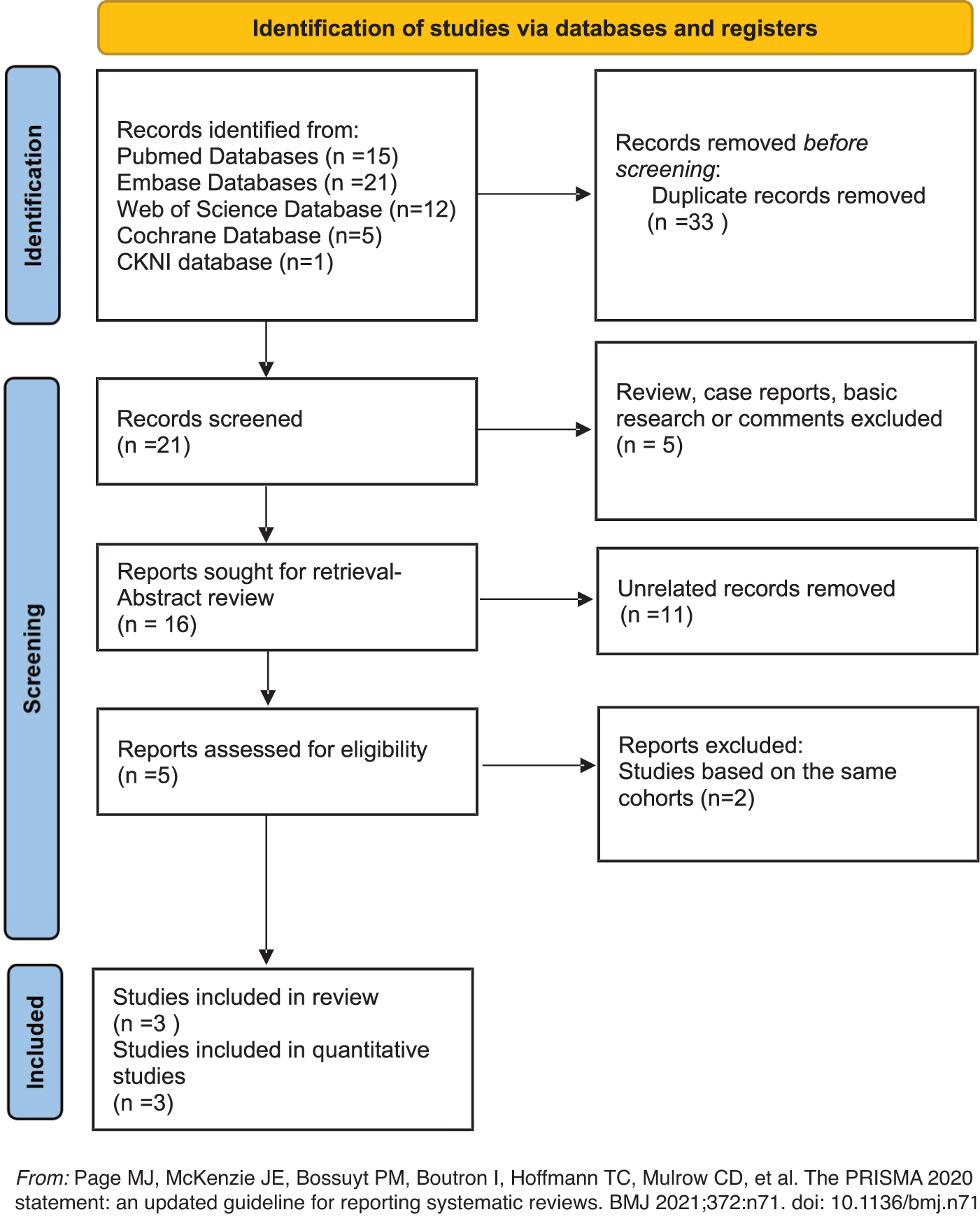
The study selection flowchart based on PRISMA principles. Color images are available online.
The Basic Information of Included Studies
BMI = body mass index; CEUS = contrast-enhanced ultrasonography; IQR = interquartile range; PCNL = percutaneous nephrolithotomy; SD = standard deviation; US = ultrasound.
Three studies (comprising 286 participants) offered relative information and were included in the comparison. In the overall synthesis, we found that baseline characteristics of patients' age, stone size, and body mass index (BMI) in the CEUS-guided PCNL group were similar to that in the control group (Supplementary Fig. S2). Pooled outcomes were reasonable when there was no significant difference in pooled baseline data between the two groups.
According to this meta-analysis, the CEUS-guided technique might offer better efficacy in PCNL for kidney stone disease than US-guided PCNL. In the success rate of a single-needle puncture comparison between CEUS-guided and US-guided groups, CEUS-guided PCNL could offer a better success rate than US-guided PCNL (OR: 3.02, 95% CI: 1.62 to 5.61, p = 0.0005; Fig. 2A) without detectable heterogeneity (I 2 = 0%, P heterogeneity = 0.94; Fig. 2A). In the puncture time comparison, SMDs were calculated and pooled since Guo X's study's time data were with different units (minutes and seconds offered in the other two studies). CEUS-guided PCNL also offered a shorter puncture time than US-guided PCNL (SMD: −1.33, 95% CI: −2.06 to −0.60, p = 0.0004; Fig. 2B), significant heterogeneity was detected (P heterogeneity = 0.0004, I 2 = 86%; Fig. 2B).

Forest plots of efficacy comparisons between CEUS-guided PCNL and US-guided PCNL.
Guo X's study brought about main heterogeneity. After omitting it, the same result was obtained (SMD: −1.72, 95% CI: −2.03 to −1.41, p < 0.0001, P heterogeneity = 0.46, I 2 = 0%). Although CEUS-guided PCNL may bring a shorter puncture time than US-guided PCNL, overall operation time was the same between the two groups (SMD: −0.18, 95% CI: −0.42 to 0.05, p = 0.12; Fig. 2C) without significant heterogeneity (P heterogeneity = 0.24, I 2 = 31%; Fig. 2C). In the hospital stay comparison, CEUS-guided PCNL could offer a shorter hospital stay compared with US-guided PCNL (SMD: −0.37, 95% CI: −0.60 to −0.13, p = 0.002; Fig. 2D), without significant heterogeneity (P heterogeneity = 0.26, I 2 = 26%; Fig. 2D). CEUS-guided PCNL appears to provide a better stone clearance rate, perhaps due to better puncture sites (OR: 2.32, 95% CI: 1.15 to 4.68, p = 0.02; Fig. 2E) without significant heterogeneity (P heterogeneity = 0.91, I 2 = 0%).
In the safety comparison, CEUS-guided PCNL also displayed some advantages. In the complication comparisons, there was no significant difference in the Grade 1/2 complication (OR: 0.79, 95% CI: 0.41 to 1.53, p = 0.48; Fig. 3A) without significant heterogeneity (P heterogeneity = 0.61, I 2 = 0%; Fig. 3A) and Grade 3/4 complication (OR: 0.44, 95% CI: 0.10 to 1.98, p = 0.28; Fig. 3B) without significant heterogeneity (P heterogeneity = 0.26, I 2 = 21%; Fig. 3B). In the overall complication comparison, there was no significant difference between the two groups (OR: 0.70, 95% CI: 0.37 to 1.30, p = 0.25, P heterogneity = 0.29, I 2 = 19%) either. Perhaps due to better puncture site selection, CEUS-guided PCNL appears to be able to provide less hemoglobin dropping after surgery (SMD: −0.82, 95% CI: −1.06 to −0.58, p < 0.00001; Fig. 3B) without significant heterogeneity (P heterogeneity = 0.25, I 2 = 29%).
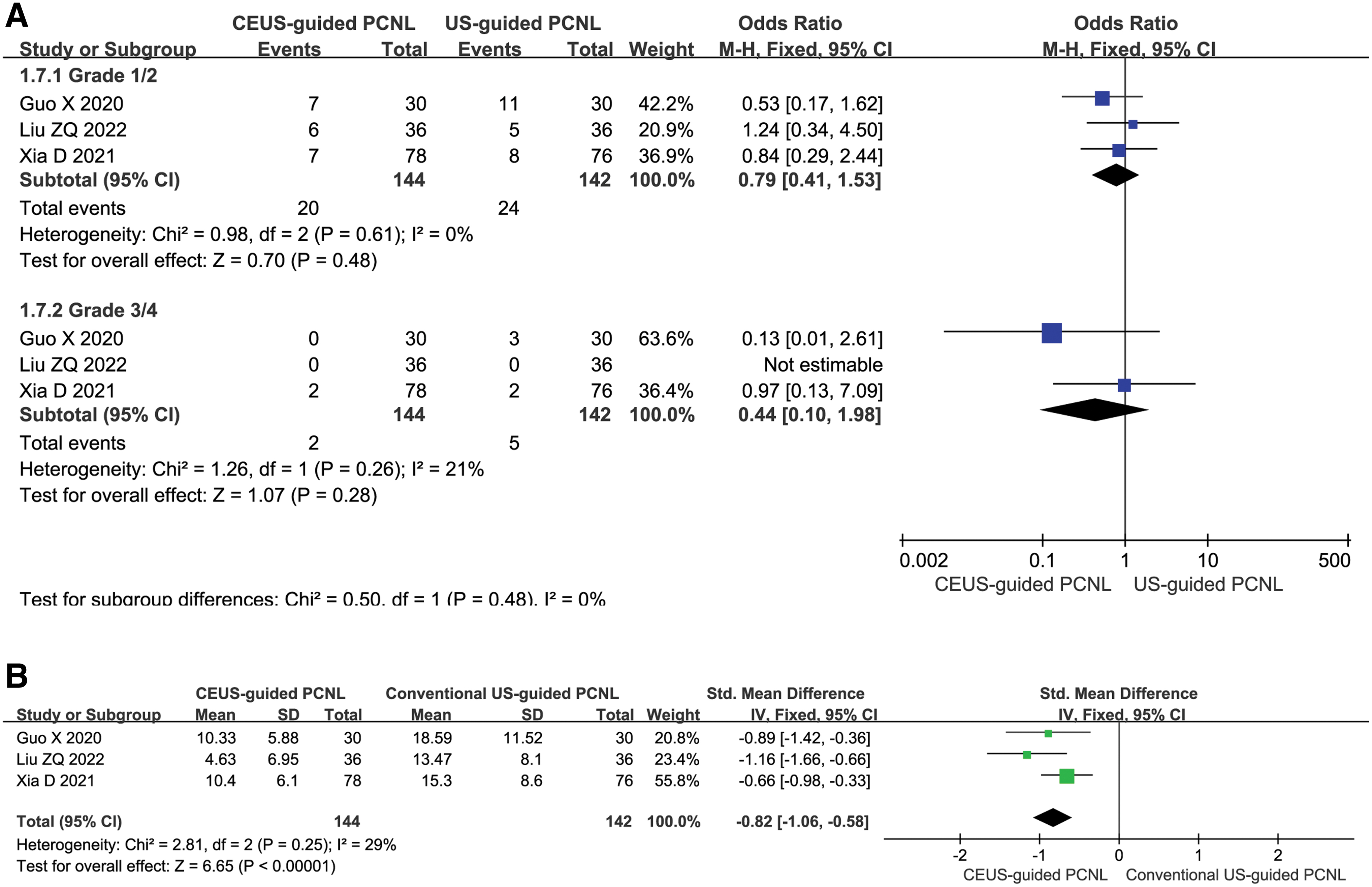
Forest plots of safety comparisons between CEUS-guided PCNL and US-guided PCNL.
Since there were only three RCTs included in this meta-analysis, linear regression-based publication bias detection methods such as the Begg and Egger tests may be inaccurate. 13 In this work, funnel plots of two main outcomes (success rate of a single-needle puncture, overall complication rate) were produced for visual estimation of publication bias (Fig. 4). Although there were only three studies in the funnel plots, they could still demonstrate the potential symmetry. We also further performed a subgroup analysis to offer more information (Table 2). According to the subgroup analysis, different subgroups did not bring about differences in pooled results. However, since there were only three studies in this meta-analysis, subgroup analysis results might be weakened.
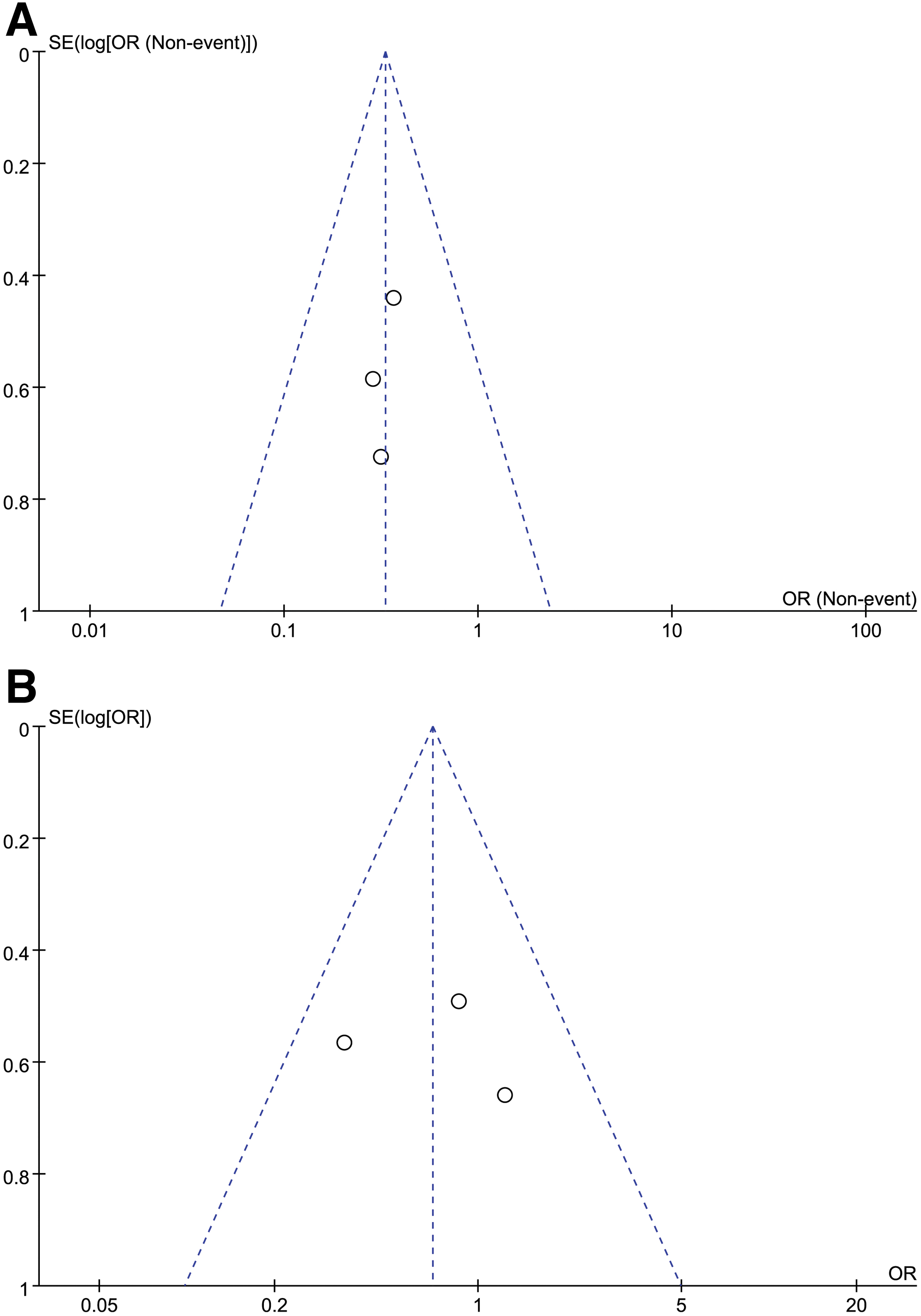
Funnel plots of two main outcomes.
Subgroup Analyses of Comparison
CI = confidence interval; OR = odds ratio.
Discussion
Because of the preceding findings, many urologists think that patients with nondilated renal collecting system PCNL who have kidney stones may benefit from using the CEUS technology. Cui and colleagues developed the CEUS approach for percutaneous nephrostomy (PCN) and concluded that CEUS may enhance the PCN procedure. 13 Due to its benefits, such as no radiation and ongoing monitoring of the needle insertion position, US-guided PCNL has become more and more popular. However, US-guided PCNL has proven a more problematic issue in urology patients without hydronephrosis. Since poor US image quality in patients without hydronephrosis, it is challenging to needle-target the nondilated target calix. According to previously published comparative studies, kidneys with dilated collecting systems had a success rate of US-guided PCN of about 96% to 100%. However, kidneys without dilated collecting systems had a success rate of only about 80%. 14
According to Degirmenci's study, the success rates of conventional US-guided PCN primary punctures for dilated and nondilated collecting systems, respectively, were 96.4% and 82.7%. Multivariate regression analysis identified the nondilated collecting system as the primary factor influencing postpuncture problems. 15
According to the results above, increasing the visibility of the nondilated system may increase puncture success rates and decrease complications in the PCNL. Intravenous diuretics are frequently used to widen the renal collecting system by encouraging the patient to produce more urine quickly. 16 Retrograde injection of physiologic saline into the calix through a ureteral catheter to dilate the renal collecting system has also been reported. 17 Although utilizing physiologic saline for retrograde expansion of the renal calix is nearly identical to employing CEUS, substantially more physiologic saline needs to be injected into the renal pelvis to have the desired effect. The risk of fever and infection may be increased by the persistently high pressure of the renal collecting system, which can cause lymphatic reflux in the renal pelvis and the systemic absorption of germs or endotoxins. As a result, using contrast agents has emerged as the best option.
To improve US pictures, sulfur hexafluoride microbubbles, a stable microbubble formulation comprising sulfur hexafluoride gas, were developed. 18 Only a minimal amount of fluid must enter the renal calix when utilizing sulfur hexafluoride microbubbles as a contrast agent for CEUS to acquire precise US pictures without significantly raising intrarenal pressure.
Three well-performed RCTs were included and analyzed in this systematic review and meta-analysis. All three included RCTs used the same US-enhancing agent and the same contrast injection method. Despite variations in the amount of contrast agent utilized, there was no appreciable difference in the three studies' CEUS methods. After the data pooling, a total of 286 patients were included in this analysis, and no significant baseline difference was found. We chose stone diameter, BMI, and age to be pooled as synthetic baseline data as follows: BMI can largely represent the patient's body size and sebum thickness, which may affect the success rate of puncture and the time of puncture in PCNL. 19 Older people always have a higher risk of complications from any surgical procedure. 20 The larger the stone diameter, the longer the operation time, which may also affect the postoperative complications, operation time, postoperative stone clearance rate, and other outcomes. 21
In the outcome data synthesis, we found that CEUS-guided PCNL could bring more benefit in single-needle success rate (OR: 3.02, 95% CI: 1.62 to 5.61, p = 0.0005), shorter puncture time (SMD: −1.33, 95% CI: −2.06 to −0.60, p = 0.0004), shorter hospital stay (SMD: −0.37, 95% CI: −0.60 to −0.13, p = 0.002), and better stone clearance rate (OR: 2.32, 95% CI: 1.15 to 4.68, p = 0.02) than conventional US-guided PCNL. Although the CEUS technique could not bring a significantly less complication rate after surgery in PCNL (overall complication: OR = 0.70, 95% CI: 0.37 to 1.30, p = 0.25. Grade 1/2 complication: OR = 0.79, 95% CI: 0.41 to 1.53, p = 0.48, Grade 3/4 complication: OR = 0.44, 95% CI: 0.10 to 1.98, p = 0.28), it could reduce hemoglobin dropping compared with conventional US-guided PCNL (SMD: −0.82, 95% CI: −1.06 to −0.58, p < 0.00001).
Almost all the synthesized data support that the CEUS-guided PCNL technique is better than conventional US-guided PCNL. There, only one comparison showed significant heterogeneity, puncture time comparison, and this was mainly introduced by Guo X's study. After careful reading of Guo X's article, we found that the time of successful puncture from Guo X's team was much shorter than that from other two studies (Fig. 2B). This situation may be caused by the extremely skilled puncture technique of Guo X's team, resulting in shorter puncture times for both US and CEUS. This may also affect the advantages of CEUS, that is, for expert operators, CEUS is obviously less helpful than it is for beginners.
However, the existing literature still points out some other possible pitfalls of CEUS-guided PCNL. First, since the needle image in US B mode is much clearer than in CEUS mode, both B and CEUS modes should be applied during the operation. This significantly increases the complexity of the operation. Second, even though US contrast media is considered a safe drug, there are still severe complications associated with contrast media that have been reported in the previous literature, and the FDA also requires the addition of a warning to the labeling of sulfur hexafluoride microbubbles emphasizing the risk of severe cardiopulmonary reactions. 18 The associated risks should be noted in future clinical trials and the practical application of contrast agents.
This systematic review still had significant shortcomings. Only three articles with a total of 286 patients were included because we only included studies of CEUS in PCNL and randomized designs to assure the consistency of the study's content. Second, because all the included research was conducted in Asia, it is difficult to generalize to other regions. More randomized trials are still required.
Conclusion
We discovered that CEUS-guided PCNL could provide more benefits in terms of single-needle success rate, shorter puncture time, shorter hospital stays, and better stone clearance rate than conventional US-guided PCNL. Although the CEUS technique could not provide a significantly less complication rate after surgery in PCNL, it could reduce hemoglobin dropping when compared with conventional US-guided PCNL.
Footnotes
Authors' Contributions
Conception and design of the study: Y.M. and P.L. Acquisition of data: Y.M., P.L., L.X., and J.W. Data analysis and/or interpretation: Y.M. and P.L. Drafting of the article and/or critical revision: Y.M. and P.L. Approval of a final version of the article: X.J.
Ethical Approval
No ethical concerns.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Figures 1 and 2.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This article is supported by grants from the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (Grant No. ZYGD2018011), and Sichuan Provincial Department of Science and Technology (Grant No. 2022YFS0304).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.