
Abstract
The technique of robotic kidney transplantation (RKT) under regional hypothermia is being described. It may be performed in all patients requiring kidney transplantation with some relative contraindications. Unlike open transplantation, RKT is a transperitoneal procedure. Patient lies supine with low lithotomy and 15° to 20° reverse Trendelenburg position. Port placement is like standard radical prostatectomy with a multiport device placed at the umbilicus. The graft after harvest needs special care on the bench to ligate all vascular communications and placed in a gauze jacket for easy handling. After transplant bed preparation, the graft is introduced in peritoneal cavity through the umbilical opening and placed over the bladder flap bed with ice slush for hypothermia. End-to-side vascular anastomoses of renal vein and artery are done with the graft lying in pelvic hollow and renal vessels facing laterally to external iliac vessels. After vascular anastomoses, the graft is rotated laterally to iliac fossa to be fixed with preformed peritoneal flap. A stented ureterovesicostomy to the recipient is done using extravesical technique. The external opening for introducing the graft and the robotic port openings is closed after leaving a drain. Postoperative (PO) care and PO immunosuppression are like the open counterpart, except the treatment of drain, which is removed on second PO day. Obese recipients and multiple graft vessels may be handled comfortably during RKT with described techniques. It is important to follow certain checkpoints to avoid bleeding. With graft and patient survival of 95.2% and 94.5%, respectively, RKT outcomes are noninferior to open technique in the published data. The RKT has less incidence of PO pain, wound infection, and symptomatic lymphoceles.
Featured Video
https://stream.cadmore.media/player/be571cc4-5379-4a7f-a581-eb11861cabe3

Indications
Kidney transplant is indicated in all patients with stage IV chronic kidney disease requiring renal replacement therapy. A kidney transplantation may be performed with either a traditional open, or a robot-assisted laparoscopic approach. Robot-Assisted Kidney Transplantation (RAKT) may replace open technique in all patients, except those who may not accommodate ports and positioning due to small size or compromised peritoneal cavity, or tolerate Trendelenburg position and pneumoperitoneum required for RAKT (poor cardiopulmonary reserve). Certain relative exclusion criteria are: ○ Patients with major transabdominal surgery or sepsis in the past ○ Patients with significant atherosclerotic disease in iliac vessels (evaluated with Doppler preop) ○ Children <15 years
Obesity or high body mass index is not a contraindication. Such patients, having been denied open transplant, have been successfully transplanted robotically. 1
Preoperative Preparation
Preoperative (PO) evaluation and preparation are similar to those for routine open kidney transplantation (OKT). All prospective recipients undergo evaluation of iliac vessels to exclude significant atherosclerotic disease. Graft positioning is usually planned in right iliac fossa. The use of left fossa may be indicated in patients with significant atherosclerotic disease in right iliac vessels, or a previously consumed right iliac fossa with a failed graft (second transplant), or other surgeries. Patient is prepared with adequate dialysis and appropriate immunosuppression as per the protocol of the center performing kidney transplantation.
Surgical Steps
Surgical technique for RAKT has been published previously, 2 although some changes may be needed with different robots and availability of instruments.
1. Patient positioning and port placement
The patient, after anesthesia and line placement, is placed in low lithotomy position with 15° to 20° Trendelenburg tilt, as for radical prostatectomy. The arms are placed by the side. Shoulder and chest are adequately padded and secured to prevent any slippage due to positioning.
We place a GelPOINT® device (Applied Medical) with a 4 to 5 cm vertical periumbilical incision. The incision and rectus sheath are opened in whole length to allow introduction of four fingers. Peritoneum is opened in line of incision and the device is secured. The device houses the lens port as well as an assistant port. It provides dual purpose of enabling the placement of ice slush with modified Toomy syringes for regional hypothermia, as described later, and putting the graft kidney into the peritoneal cavity. Two robotic ports, for right and left arms, are placed 4 cm from the lateral edge of the GelPOINT device at the level of umbilicus. Fourth arm port is placed in the iliac fossa 8 cm away from the left port for placement of the graft in the right iliac fossa, and vice versa. A 12 mm assistant port is placed in the contralateral flank. Robot is docked between the legs. Patient may be placed in supine position too if so desired, with oblique robot docking. The later position may be preferable in patients with limited hip mobility.
2. Bed preparation
The instruments are centered around the external iliac vessels. With the bipolar device in nondominant and hot shears in other hand, the peritoneum is incised anterior to the external iliac vessels on the right side, and the external iliac artery and vein are dissected off the surrounding lymphatics. It may not be necessary to divide or excise lymphatics unless those are bulky and likely to interfere during anastomosis. Vessels are mobilized, from the level of iliac bifurcation to inguinal ligament, to obtain enough length for placing clamps across for anastomosis. Some of internal iliac vein tributaries may need clipping and division, or ligation in continuity, to allow safe placement of bulldog clamps on either side.
Peritoneal incision over the iliac vessels is extended from center of incision going laterally as a “T” incision (Fig. 1), and two triangular flaps are raised, proximally lifting the cecum, and distally until the inguinal ligament. This creates two triangular flaps for retroperitonealization of the graft in iliac fossa following the vascular anastomosis.
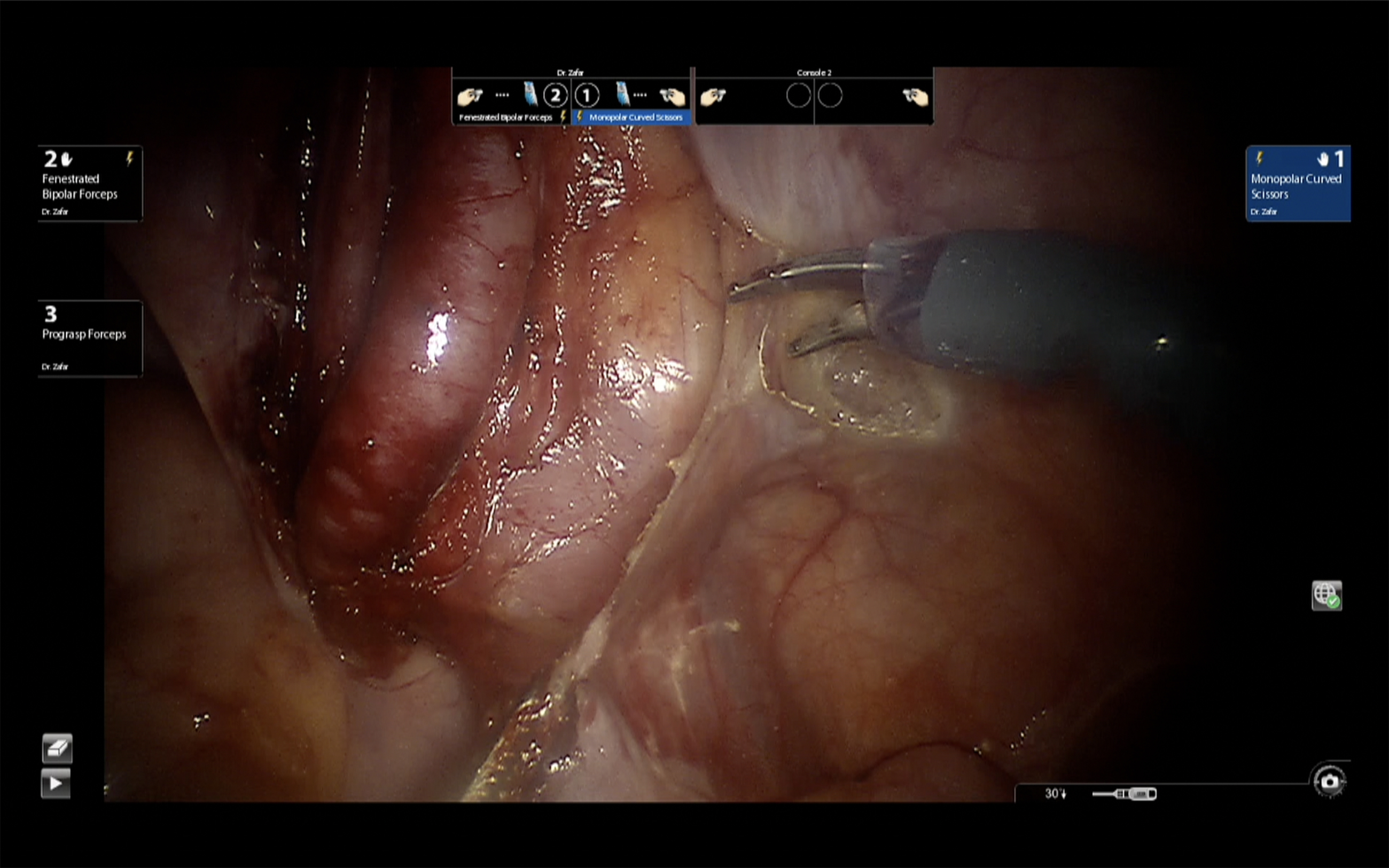
Bed preparation with isolation of external iliac vessels and peritoneal incision.
With Foley's catheter in place, the bladder is dropped until the pubic symphysis. Bladder is filled with 150 mL saline and further dissected on the side of transplantation to clear space for vesicostomy. A window is created behind the vas/round ligament on the side of proposed transplant to allow passage of ureteric pedicle. A small oblique incision is made in prospective ureteric line on this side of ureteric reimplantation. Submucosal plane is developed using sharp shears. We prefer to create a small detrusor muscular tunnel too proximally. A loop is placed through this tunnel to allow passage of ureter underneath. Bladder mucosa in distal part of detrusor myotomy incision is incised, and a stay suture is left in the distal end of the mucosal incision.
The graft bed preparation is complete now.
3. Graft preparation and hypothermia
In the adjoining room, the graft is harvested from the donor. Preparation of graft kidney after harvest is very important for robotic renal transplantation. All communications are suture tied and cut while defatting the graft. The graft is enclosed in small amount of ice slush and covered with gauze. The gauze has a small opening for the hilar structures (Fig. 2). The vessels are directed through this hole and the gauze jacket is draped, and suture fixed laterally, identifying lateral border. A long silk end of suture is left at the upper pole for identification. The ureter coming out of the lower end flags the lower end of the graft. This jacket holds back the perihilar fat while the vessels are visible clearly. More importantly, the jacket allows the grasp with robotic instruments and moving the graft around in the peritoneal cavity for orientation.
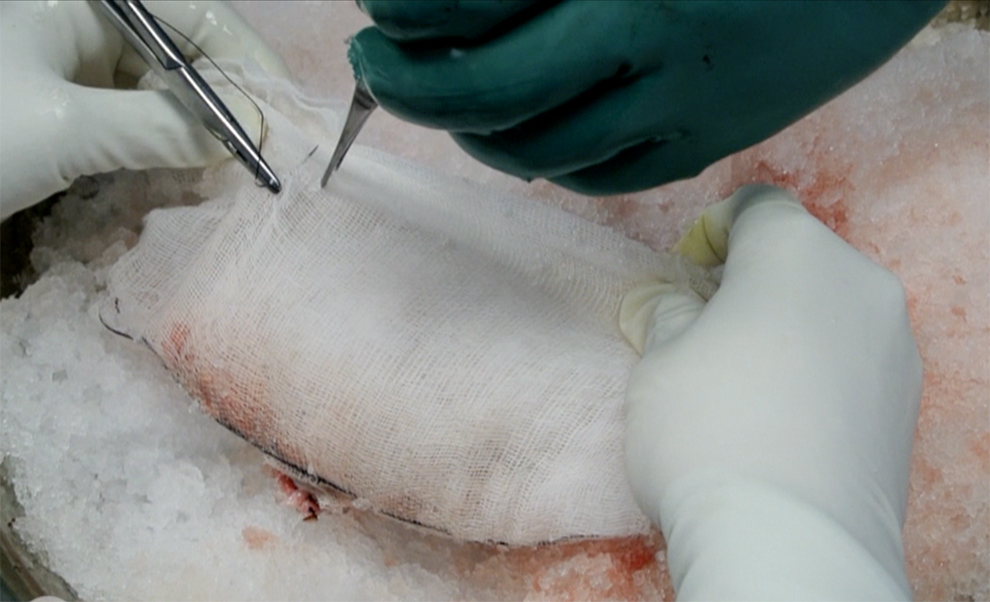
Graft jacket preparation with vessels coming out through a hole.
Fine ice slush is pushed through GelPOINT device using Toomey syringes with cut away front nozzle and placed over the temporary graft bed over the bladder flap. About 100 mL of ice slush is initially used, each syringe providing 50 mL of ice slush. More ice may be placed later during the procedure if the procedure gets prolonged. The graft is now placed inside the peritoneal cavity through the GelPOINT device, the cap is locked, and the robot is docked.
4. Venous anastomosis
The graft is oriented and placed medial to the dissected external iliac vessels in the pelvic hollow. The renal vessels coming out of the jacket face the vessels, while the lower pole, identified with ureter, goes toward the bladder. Bulldog clamp handed by the assistant through the assistant port is placed for proximal and distal control on the vein around the selected anastomotic site. External iliac vein is incised at the selected site and flushed with saline before starting the anastomosis. Renal vein is anastomosed to external iliac vein using CV-6 polytetrafluoroethylene (PTFE) suture with 9 mm needle, end to side, in a continuous manner. This PTFE suture is preferred to polypropylene suture due to its easier handling. The monofilament nonabsorbable suture does not have memory and is strong enough to be handled by the robotic instruments.
A 15 cm length of one end of this double-ended suture is used for vein. It is easier to start anastomosis at the distal end, running in the posterior wall. A knot is tied at lower end to turn sides before proceeding anteriorly (Fig. 3). The anastomosis is flushed with heparinized saline before last suture is tied. After the venous anastomosis is complete, the renal vein is clamped and the iliac vein continuity restored, taking off proximal clamp first and then releasing the distal end.

Completion of posterior layer of end-to-side venous anastomosis.
5. Arterial anastomosis
Like the vein, the selected segment of the external iliac artery is isolated using bulldog clamps. A small arteriotomy incision is made, and desired opening created using a 3.6- or 4.0-mm aortic punch inserted through the GelPOINT device. The usual punch length may fall short, and we have long aortic punch(s) fabricated for the purpose. The arterial segment is flushed, a 10 cm second end of the same CV-6 PTFE suture, used for vein, is used for arterial anastomosis. An end-to-side anastomosis is done in a fashion like venous anastomosis (Fig. 4). A large needle driver is used in dominant hand while black diamond forceps in the other hand works as a DeBakey forceps to hold and spread to identify edge correctly. After the completion of anastomosis, renal artery is clamped and the clamps are released from external iliac artery, distal end first. The anastomotic site is inspected for need for any additional sutures. Some ooze form arterial holes stop on its own in a short time.
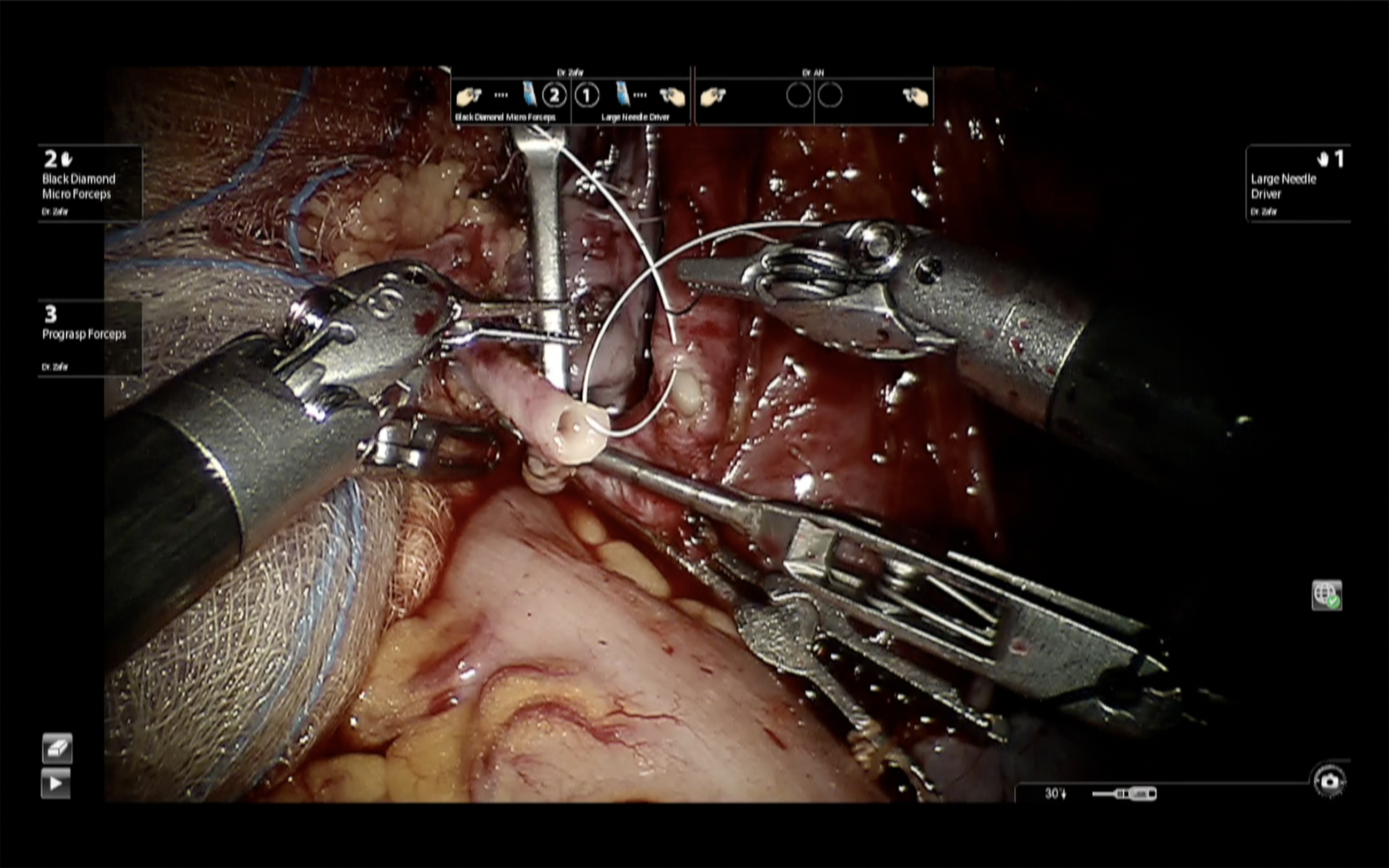
Starting end-to-side arterial anastomosis.
6. Revascularization and graft fixation
The intra-abdominal pressure is dropped to 8 from 10 mmHg. The gauze is cut and removed from over the graft. Some perforators on the surface of kidney may need to be treated with bipolar energy. The graft is inspected for color and turgor. Once the integrity of the anastomosis is confirmed, the graft is flipped laterally by 180° and the two previously prepared peritoneal flaps are brought over the kidney and fixed using clips to fix kidney in the iliac fossa (Fig. 5). This ensures that vessels may not get kinked with torsion or movement of the graft. It also allows safe percutaneous access to kidney for ultrasound-guided biopsy postoperatively, not an uncommon event following kidney transplantation.
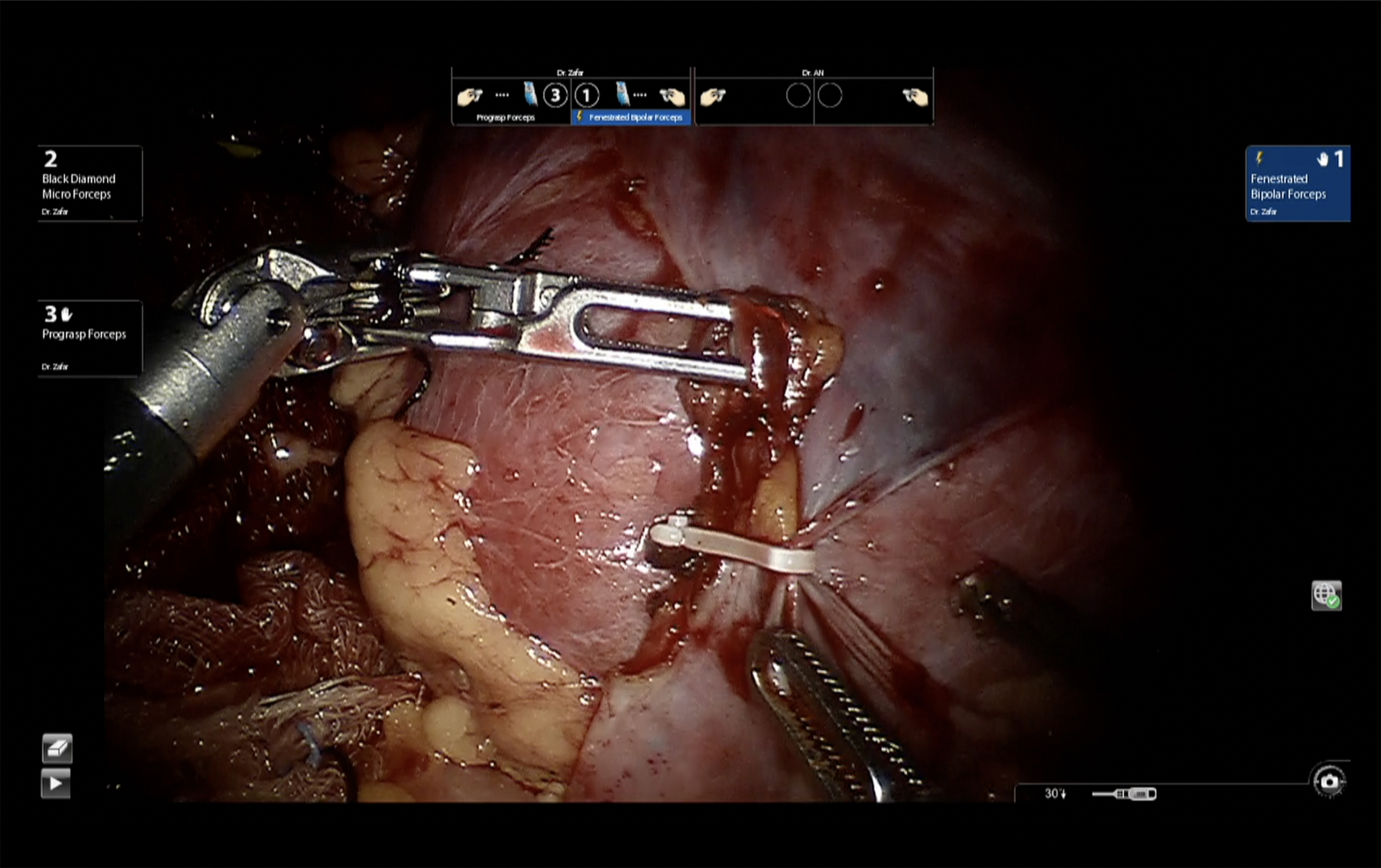
Fixation of graft in iliac fossa with peritoneal flaps.
7. Ureterovesicostomy
The ureter is brought out beneath the vas and the previously made detrusor tunnel. 4-0 Polydioxanone suture (PDS), continuous suture, is used for ureterovesical anastomosis. The medial layer is sutured first, followed by the lateral layer (Fig. 6). A stent is placed after completion of the first layer. Detrusor is now closed over the ureter using a 3-0 V-Loc® suture.

Ureterovesical anastomosis.
8. Drain and closure
A drain (usually a 24F) is placed in the pouch of Douglas over the graft through the right lateral assistant port site. An additional flat drain may be placed through the left-sided fourth arm port and placed anterior to the bladder. Robot is undocked and port sites and the umbilical incisions are closed after removal of the GelPOINT device.
An on-table vascular doppler study confirming the revascularization of the graft is desirable before moving the patient to transplant intensive care unit. Indocyanin Green fluorescence videography may also be used to assess ureteral and graft perfusion intraoperatively. 3
PO Care
PO care of a RAKT case is like that transplanted with open technique, except managing the drain. Immunosuppression is as per institutional protocol, similar to open counterpart. Hematocrit and renal functions are monitored as per the protocol. Drain fluid is sent for fluid creatinine measurement on PO day 1. If normal, the drain is removed on day 2 irrespective of the drain output volume. Unlike open transplant, the drain fluid is absorbed in robotic approach with free access to peritoneal cavity with little risk of lymphocele. Percutaneous graft biopsy may be obtained easily, if needed during the PO course. 4 Foley's catheter is removed on PO day 4, and patient may be discharged the next day.
Troubleshooting
Obese patient: Obese recipient, often a problem during open transplant, is a relative indication for robotic renal transplantation. Robotic approach has been successfully used in morbidly obese patient denied open transplantation surgery. 1
Previous surgeries: Mesh hernioplasty and appendectomy are common procedures causing bladder and right iliac fossa adhesions requiring adhesiolysis. Such adhesiolysis may be needed before or after the port placements. Initial umbilical open approach enables the surgeon to assess and monitor intrabdominal conditions before proceeding for surgery. Extensive adhesions following previous major abdominal procedures or sepsis may be dealt with open transplant surgery or robotically using extraperitoneal approach.
Check points: It is advocated to observe strict sequence of clamp release with four check points to avoid vascular complications
After venous anastomosis is complete, a bulldog is placed on renal vein and the proximal clamp over external iliac vein is released followed by the distal clamp
After completion of arterial anastomosis, a bulldog is placed on renal artery too, and the distal clamp over external iliac artery is released first. Retrograde filling of the artery allows easy identification of need for any additional suture before release of the proximal clamp and revascularization of the graft.
Clamps from the renal vein is then removed followed by release of renal artery. Turgidity and color of the graft is observed at this time, as well as bleeding from surface perforators. A brisk diuresis too ensures optimal revascularization.
The flipping of the graft to iliac fossa may kink the vessels. Observation of the color and turgidity of the graft, including observation of the pulsations of the renal artery, after the graft is flipped is ensured before and after fixing of the graft in its final position.
The use of left iliac fossa: Any compromise of the right iliac fossa, by significant adhesions, previous renal transplant, or compromised iliac vessels may prompt the use of left iliac fossa for the graft placement.
Vascular anomalies of the graft: Left side is often the preferred graft side for OKT. Right-sided renal graft with small renal vein may pose problems during open surgery, but is comfortably managed robotically with the graft placed medial to vessels. Multiple renal arteries, although avoided during the learning phase, would require pantaloon anastomosis on the bench before RAKT. An additional small upper polar artery may be anastomosed robotically to inferior epigastric artery. 5
Bleeding: Troublesome bleeding is rare if check points are adhered, as outlined earlier. Bleeding may still occur from one of the renal artery branches, or one of renal vein tributaries, if a good graft preparation was not adhered to. Identification of the bleeding arterial twig(s) may require placement of proximal clamp on iliac artery allowing only distal low-pressure filling of the artery. This reduced the bloody field significantly and bleeders may be identified using suction irrigation.
Failure to revascularize graft: A poor arterial anastomosis, kink, or a thrombus may cause failure of graft revascularization. Venous anastomosis is invariably robust. Immediate cold reperfusion, in situ or after extraction, may be needed before a redo anastomosis. Depending on his experience, a surgeon may decide to tackle such situation robotically. He may convert to open surgical approach anytime, extending midline incision inferiorly or through a flank routine transplant incision.
List of Instruments
Da-Vinci robotic instruments needed
420179 Hot Shears™ (Monopolar Curved Scissors)—Requires Tip Cover Accessory (PN 400180)
420172 Maryland Bipolar Forceps
420205 Fenestrated Bipolar Forceps
420033 Black Diamond Micro Forceps
420006 Large Needle Driver
420001 Potts Scissors
GelPOINT device (may be omitted if using Pfannenstiel incision)
Twelve-millimeter disposable trocars (two)
Aortic punch (long handle) 3.6 and 4 mm (may avoid if using Pott's scissor)
GORE-TEX CV-6 sutures with 9 mm needle (two)
Silk sutures 2-0 (two) for ties
4-O PDS (two) for ureterovesicostomy closure
Wound closure suture of preference to the center
Drain (24F or flat suction drain)
Standard minor set (surgical) for opening and closure
Bowel grasper (laparoscopic)/tissue grasper (for assistance)
Suction/irrigation system
Robotic bulldog clamps (six)
Hem-o-lock clip applicator
OKT set should always be handy if conversion is needed
Alternate or Modification of Technique
Like all evolving techniques, the procedure would be modified by each surgeon to his comfort. There are few modifications of the technique worth mentioning:
Using a different route to place the graft
The use of Pfannenstiel incision to place the graft and avoiding the umbilical multiport device. 6
Pros: saves the cost of GelPOINT device
Con: Need for a transverse incision in supraumbilical region, requiring closure before the vascular anastomosis after placing graft, consuming precious time. In the event of emergency, immediate hand access is an added advantage of GelPOINT device.
The use of vaginal approach to place graft in multipara females avoids umbilical or supraumbilical incision and makes procedure more cosmetic. 7
Avoiding transperitoneal cavity: Extraperitoneal approach too has been attempted for robotic transplantation and may be useful if extensive intraperitoneal adhesions are suspected. 8
Avoiding the use of ice slush/regional hypothermia:
Some surgeons find the use of ice slush messy and may like to avoid regional hypothermia, relying solely on the cold perfusion of the graft. Transplantation without using ice slush may be an option for an experienced surgeon sure of completing anastomosis within a reasonable time. If prolonged, it risks increased incidence of delayed graft function.
RAKT using single port robot have also been described. 9
Clinical Outcomes
Our medium-term outcomes following a live donor RAKT have been published recently. 10 RAKT outcomes in 126 recipients were compared with propensity-matched (1:3) contemporary 378 OKT recipients. Apart from the expected minimally invasive surgery advantages (less perioperative pain and analgesic requirement and blood loss), the robotic group was superior with absence of wound infection and symptomatic lymphoceles. Renal function recovery was overlapping in two groups, with similar discharge, 3-, and 6-month creatinine levels. Incidence of delayed graft function was comparable, as was the incidence of immunological injuries (acute rejections). There were no differences in graft (95.2% vs 96.3% at 36 months, RAKT vs OKT) and overall survival (94.5% vs 98.1% at 36 months, RAKT vs OKT) between the two groups
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.