
Abstract
Purpose:
Water vapor thermal therapy (WVTT, i.e., Rezum®) and prostatic urethral lift (PUL, i.e., Urolift®) are minimally invasive surgical therapy (MIST) options for benign prostatic hyperplasia (BPH). Few studies have directly compared the two procedures. We examined the clinical characteristics and postoperative outcomes of patients undergoing WVTT and PUL at our high-volume urban academic center.
Methods:
We reviewed our institutional MIST database to identify patients with prostate sizes ≥30 and ≤80 cc who underwent WVTT or PUL for treatment of BPH between January 2017 and September 2021. Pre- and postoperative outcomes, including retreatment rates, American Urological Association symptom score (AUA-SS), maximum flow (Qmax), postvoid residual (PVR), medication usage, trial of void success rates, catheterization requirements, and postoperative complications within 90 days were extracted and compared between procedures.
Results:
Three hundred seven patients received WVTT and 110 patients received PUL with average follow-up times of 11.3 and 12.8 months, respectively. WVTT patients showed significant improvements in AUA-SS, Qmax, and PVR, whereas PUL patients showed improvements in only AUA-SS and Qmax. Both WVTT and PUL patients with longitudinal follow-up demonstrated improvements in AUA-SS, Qmax, and PVR. Postoperatively, alpha-blocker utilization was significantly decreased following both WVTT and PUL (WVTT: 73.9%–46.6%, PUL: 76.4%–38.2%, both p < 0.001). Compared to patients receiving PUL, WVTT patients more frequently reported postoperative dysuria (22.8% vs 8.3%, p = 0.001) and nonclot-related retention (18.9% vs 7.3%, p = 0.005); PUL patients more frequently experienced postoperative clot retention (7.3% vs 2.6%, p = 0.027). There were no differences in rates of postoperative bladder spasm, trial of void success, urinary tract infections, or emergency department visits. Postoperative erectile dysfunction and retrograde ejaculation were rare and occurred at similar rates.
Conclusion:
In the real-world setting, WVTT and PUL have similar medium-term efficacy in improving symptoms and decreasing medication utilization for patients with BPH. Differences in postoperative complication profiles should inform patient counseling.
Introduction
Symptomatic benign prostatic hyperplasia (BPH) occurs when the overgrowth of prostatic tissue compresses the prostatic urethra and constricts the urethral opening. Consequent lower urinary tract symptoms (LUTS) can negatively impact patients' quality of life. 1 Untreated BPH may lead to serious complications such as urinary tract infections (UTIs), acute urinary retention, and renal failure. 2 Patients with BPH-induced LUTS who fail life-style modifications and medical therapies are often managed surgically.
Transurethral resection of the prostate (TURP) has been considered the gold standard for definitive surgical intervention. 3 However, the efficacy of TURP in improving urinary flow is accompanied by risks of undesirable adverse effects, including sexual dysfunction and incontinence. 4 Numerous ambulatory minimally invasive surgical therapies (MISTs) have emerged in recent years to improve LUTS while minimizing postoperative side effects of TURP, 5 of which the most prominent include transurethral water vapor thermal therapy (WVTT, i.e., Rezum®) and prostatic urethral lift (PUL, i.e., UroLift®).
WVTT is performed transurethrally via the delivery of radiofrequency-generated water vapor into the prostate tissue, thermally inducing cellular necrosis and ablation. 6 The subsequent decrease in prostatic volume can provide improvement of LUTS. The thermal effects are targeted only to specific treatment zones, thereby preserving the surrounding tissue. In contrast, PUL mechanically opens the prostatic fossa with implanted permanent, nonabsorbable sutures to create a continuous anterior channel through the prostatic urethra while preserving neurovascular bundles in the area. 7
Prospective clinical trials have demonstrated PUL and WVTT's efficacy in improving LUTS, while minimizing postoperative adverse effects. 8 –10 Real-world studies further confirmed the effectiveness of WVTT and PUL in more heterogenous patient populations with less stringent follow-up schedules. 11 –15 Together, these studies have prompted contemporary American Urological Association (AUA) guidelines to recommend either WVTT or PUL as surgical treatment options for men with BPH and prostate volumes <80 cc. 2,16 There is a paucity of literature directly comparing WVTT to PUL, and existing studies are limited in sample size. 17,18 Here, we present the largest study to date that directly compares the clinical characteristics and postoperative outcomes for WVTT and PUL for the management of symptomatic BPH.
Materials and Methods
After obtaining IRB approval, we queried our institutional MIST database for patients who were treated with WVTT or PUL from January 2017 to September 2021. Patients with preoperative prostate sizes between 30 and 80 cc and postoperative follow-up >30 days were included.
Patient demographics, BPH surgical history, and prostate cancer history were extracted from patient records. Clinical metrics of disease, including pre- and postoperative prostate size, AUA symptom score (AUA-SS), maximal urinary flow rate (Qmax), postvoid residual (PVR), sexual health inventory for men score (SHIM), serum prostate specific antigen (PSA) level, and BPH medication usage were extracted. BPH medications were classified as alpha-blockers, 5-alpha-reductase inhibitors (5AR-I), phosphodiesterase-5 inhibitors (PDE5-I), or antispasmodics. Postoperative outcomes included surgical and medical retreatment rates, unresolved catheterization dependence within 90 postoperative days, fever, hematuria, dysuria, bladder spasms, retention, clot retention, hematospermia, erectile dysfunction, suspected UTI, emergency department (ED) visits, and/or hospital readmissions.
For patients with multiple data points on preoperative clinical metrics and medication utilization, the data closest to the date of surgery were used. For patients with multiple data points on postoperative clinical metrics and medication utilization, the data closest to last follow-up date were used. Median postoperative day of follow-up for each postoperative clinical metric was reported. Patients with longitudinal follow-up were defined as those with pre- and postoperative urologic parameter measurements (AUA-SS, Qmax, PVR). Primary analyses were performed on the entire study cohort. Subgroup analyses were performed based on two prostate size subcategories: 30 to <50 cc and 50 to ≤80 cc.
Statistical analyses were performed using GraphPad Prism 9.3.1. For continuous data, Mann-Whitney U and Wilcoxon signed-rank (paired data) were used for group comparison. Chi-squared analysis or Fisher's exact test (for data with <5 records) was used to analyze group differences in categorical data. Kaplan–Meier estimates were used to calculate 1-year retreatment rates due to variable follow-up. Univariate logistic regressions were performed to assess for independent predictors (age, body mass index [BMI], baseline prostate size, AUA-SS, Qmax, PVR, and number of injections/implants) of postoperative complications. Multivariate logistic regressions were performed using variables with p-values ≤0.2 from univariate logistic regressions. For all statistical tests, p-values ≤0.05 were used to denote statistical significance.
Results
Five hundred fifteen underwent WVTT and 191 patients underwent PUL. Of these, 307 WVTT and 110 PUL patients met inclusion criteria. Patient exclusions are detailed in Figure 1. Baseline patient characteristics are summarized in Table 1. Patient treated with PUL were older and had greater baseline PVR (PUL: 158 ± 184 mL, WVTT: 86 ± 127 mL, p < 0.001). Patients who underwent WVTT had greater preoperative prostate volume. There were no differences in BMI, baseline PSA, AUA-SS, Qmax, or SHIM score between groups. The proportions of patients who had indwelling catheters or relied on clean intermittent catheterization at baseline were similar between groups, as were the proportion of patients with prior BPH surgery. The average follow-up duration between the groups were similar (WVTT: 11.3 ± 7.8 months, PUL: 12.8 ± 12.0 months, p = 0.260).
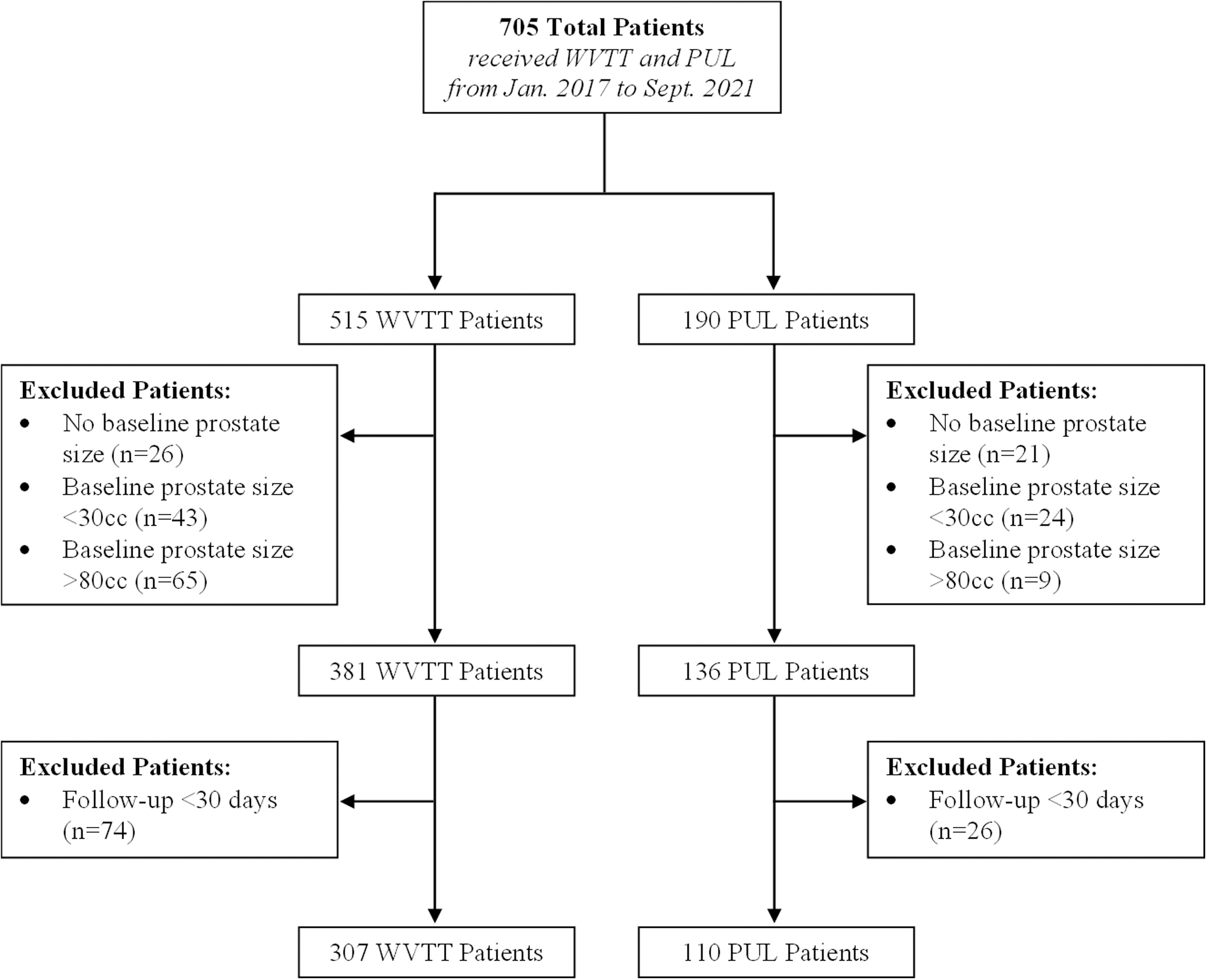
Study inclusion and exclusion flowchart for patients who received WVTT and PUL. PUL, prostatic urethral lift; WVTT, water vapor thermal therapy.
Baseline Characteristics, Surgery Details, and Benign Prostatic Hyperplasia Surgical History for Patients Treated Water Vapor Thermal Therapy or Prostatic Urethral Lift Between January 2017 and September 2021
BMI = body mass index; BPH = benign prostatic hyperplasia; PSA = prostate- specific antigen; PUL = prostatic urethral lift; SD = standard deviation; WVTT = water vapor thermal therapy.
Postoperatively, WVTT patients showed significantly improved mean AUA-SS (16.5 ± 7.4 to 11.0 ± 6.6, p < 0.001), Qmax (9.0 ± 5.4 mL to 11.0 ± 5.7 mL, p < 0.001), and PVR (86 ± 127 mL to 47 ± 71 mL, p < 0.001)
Urologic Parameters and Medication Utilization of Patients Who Were Treated with Water Vapor Thermal Therapy or Prostatic Urethral Lift at a Single Institution Between January 2017 and September 2021
AUA-SS = AUA symptom score; IQR = interquartile range; POD = post-operative day; PVR = postvoid residual; Qmax = max flow rate; SHIM = sexual health inventory for men score.
For the subset of both WVTT and PUL patients with both pre- and postoperative urologic parameter measurements, significant improvements were seen in AUA-SS, Qmax, and PVR without significant differences in the magnitude of improvements from baseline in AUA-SS, Qmax, and PVR between PUL and WVTT patients (Table 2B). Postoperatively, both WVTT and PUL patients had significant decreases in alpha-blocker utilization (Table 2C). WVTT patients also had significant increases in antispasmodic medication usage.
Table 3 summarizes the postoperative outcomes of the overall cohort for each procedure. There were no significant differences in 1-year retreatment rates or mean time to retreatment between the groups. All WVTT patients and 36.4% of PUL patients received postoperative Foley catheters. WVTT patients more frequently experienced dysuria and nonclot-related retention. PUL patients more frequently experienced clot retention. Rates of postoperative UTI, ED visits, and readmissions within 90 days were similar between the groups.
Clinical and Postoperative Outcomes of Patients Who Were Treated with Water Vapor Thermal Therapy or Prostatic Urethral Lift at a Single Institution Between January 2017 and September 2021
Note: 1-year retreatment rate is calculated with Kaplan–Meier estimates with p-value is derived from Log-Rank Test.
ED = emergency department; UTI = urinary tract infection.
Several risk factors for postoperative issues were identified. For WVTT patients, increased baseline Qmax (odds ratio [OR]: 1.155, 95% confidence interval [CI]: 1.056–1.302) was associated postoperative bladder spasms. Increased baseline AUA-SS (OR: 1.119, 95% CI: 1.024–1.239) and decreased baseline Qmax (OR: 0.8151, 95% CI: 0.6740–0.9485) were associated with development of postoperative retention. Finally, decreased age (OR: 0.9636, 95% CI: 0.9298–0.9975) was associated with being BPH medication-free after WVTT. For PUL patients, decreased BMI (OR: 0.8581, 95% CI: 0.7286–0.9863) and baseline AUA-SS (OR: 0.8910, 95% CI: 0.8065–0.9741) were associated with postoperative hematuria. Decreased baseline AUA-SS (OR: 0.8717, 95% CI: 0.7694–0.9706) was associated with development of postoperative bladder spasms.
Subgroup analyses of WVTT and PUL patients based on prostate size (30–50 cc, 50–80 cc) were performed (Table 4). There were 193 WVTT and 82 PUL men with medium-sized prostates 30–50 cc. For this subgroup, WVTT patients showed significant improvements in AUA-SS (WVTT: 16.1 ± 7.9 to 11.3 mL ±6.8, p < 0.001), Qmax (9.7 ± 6.0 mL to 11.1 ± 5.7 mL, p = 0.011), and PVR (78 ± 119 mL to 41 ± 62 mL, p = 0.009). In contrast, PUL patients had significant improvements in AUA-SS (18.1 ± 7.0 to 12.8 ± 6.9, p = 0.002) and Qmax (7.7 ± 4.9 mL to 10.2 ± 6.2 mL, p = 0.025) with no significant changes in PVR (140 ± 183 mL to 90 ± 121 mL, p = 0.094).
Prostate Size Subgroup Analysis of Medication Utilization and Postoperative Outcome for Patients Treated with Water Vapor Thermal Therapy and Prostatic Urethral Lift
There were 114 WVTT and 28 PUL men with moderately large prostates 50–80 cc. For this subgroup, WVTT patients had significant improvements in AUA-SS (17.1 ± 6.7 to 10.6 ± 6.4, p < 0.001), Qmax (7.9 ± 3.9 mL/s to 10.7 ± 5.6 mL/s, p = 0.007), and PVR (100 ± 140 mL to 58 ± 83 mL, p = 0.007) whereas PUL patients showed only improvement in PVR (206 ± 182 mL to 98 ± 195 mL, p = 0.001) with no changes in AUA-SS (13.5 ± 5.1 to 9.3 ± 6.3, p = 0.074) or Qmax (7.5 ± 4.0 mL/s to 8.4 ± 7.3 mL/s, p = 0.667).
Compared to men with prostates 30–50 cc, men with prostates 50–80 cc received more WVTT injections (30–50 cc: 4.3 ± 1.6 injections, >50–80 cc: 5.8 ± 2.0 injections, p < 0.001) and PUL implants (30–50 cc: 4.5 ± 1.0 implants, >50–80 cc: 5.2 ± 1.3 implants, p = 0.010). In both subgroups, 30–50 cc and 50–80 cc, PUL and WVTT patients had significant decrease in alpha-blocker usage and only WVTT patients had significant increase in antispasmodic usage. Compared to PUL patients, WVTT patients in both subgroups more frequently reported dysuria.
Discussion
The efficacy of WVTT and PUL for men with BPH have been demonstrated in two landmark prospective, randomized clinical trials by McVary et al and Roehrborn et al, respectively. 8,9 Both studies showed that WVTT and PUL provide significant, durable improvements in urinary function with preservation of sexual function, highlighting novel minimally invasive treatment options available to men with BPH. However, direct comparisons between PUL and WVTT in context outside of controlled clinical trials are sparse.
Previous small retrospective studies by Baboudjian et al (n = 48) and Tutrone and Schiff (n = 53) demonstrated that WVTT and PUL provided similar significant improvements in BPH symptoms, while PUL patients showed faster recoveries with decreased rates and duration of postoperative catheterization. 17,18 However, the small sample sizes of these studies limited analyses on postoperative medication usage and adverse effect profiles. This is the largest retrospective study to directly compare the two procedures. Our study confirmed the findings of previous comparative studies regarding the similarities in BPH symptom improvement and the differences in overall postoperative course between PUL and WVTT. Our study further elucidates the comparative efficacy, medication utilization, and detailed postoperative complication profiles of WVTT and PUL.
The landmark prospective studies of WVTT and PUL used inclusion criteria based on prostate size (between 30 and 80 cc) and baseline clinical metrics of disease (Qmax <12 mL/s, PVR <250 mL, AUA-SS >13). In contrast, our study included patients with similar prostate sizes without exclusion criteria based on baseline Qmax, AUA-SS, or PVR. 8,9 At 1-year follow-up, patients in the WVTT and PUL clinical trials showed greater improvements in Qmax and AUA-SS than patients who received these MIST procedures in our study. The reasons for the decreased effect seen in our study compared to the prospective trials are likely multifactorial. The lower baseline AUA-SS and greater Qmax for patients in this study likely translated to decrease magnitude of postoperative improvements in AUA-SS and Qmax.
Although previous real-world studies have consistently confirmed the significant improvements in BPH symptoms after WVTT and PUL, the magnitude of improvement in AUA-SS, Qmax, and PVR varied greatly among the studies. 19 Compared to prior studies of PUL, our study observed less improvement in AUA-SS (29% vs 39%–52% from baseline) and similar Qmax (28% vs 15%–55% from baseline). 7,14,20 Likewise, compared to prior studies of WVTT, our study also showed less improvements in AUA-SS (33.3% vs 45%–68% decrease from baseline) and similar Qmax (22% vs 18%–65%). 12,21,22
For the subgroup with prostate sizes 30–50 cc, PUL and WVTT patients demonstrated similar, significant improvements in AUA-SS and Qmax, and significant reductions in alpha-blocker usage, suggesting similar effectiveness in LUTS management between WVTT and PUL. For the subgroup with prostate size >50 cc, WVTT patients had significant improvements in all clinical metrics of disease, whereas PUL patients only showed improved PVR. Our results suggest that WVTT may be more effective than PUL in patients with moderately large prostate sizes.
The postoperative side-effect profile differed between WVTT and PUL. Clot retention may have occurred more frequently in PUL patients due to the absence of postoperative catheters in many of these patients. Without catheters, small blood clots are more likely to cause episodes of clot retention. PUL and WVTT patients reported similar rates of postoperative bladder spasm. However, WVTT patients received increased usage of antispasmodic after the procedure. As our study reviewed the presence of bladder spasms without noting the severity or persistence of the spasm, the increase in antispasmodic postoperatively may suggest that WVTT patients experience more severe and bothersome bladder spasms that require medication for alleviation. Patients may subsequently elect to continue the medication due to urinary flow improvements.
Postoperative complications reported in this study were largely consistent with data from previous WVTT and PUL studies. Compared to previous real-world studies, WVTT patients in this study reported similar rates of hematuria (32% vs 14%–72%), dysuria (22% vs 22%–28%), and suspected UTI (9% vs 4%–20%), but greater rates of postoperative retention (19% vs 4%–14%). 11,21,23,24 Rates of postoperative hematuria (23% vs 11%–75%), dysuria (8% vs 2%–53%), and UTI (4% vs 3%–10%) for PUL patients in this study were consistent with previously reported complication rates from real-world studies. PUL patients reported more frequent bladder spasm (13% vs 0.3%) and retention (20.2% vs 0.3%–7.5%) than the prospective studies. 9,25
The 1-year retreatment rate for WVTT in this study was 4.4%, slightly higher than the 1 year retreatment rate of 1%–3.4% reported by other retrospective real-world studies. 8,11,12,15,18,24 The increased retreatment rate reported in our study may be due to variable follow-up in our cohort. Patients with satisfactory outcomes may have less frequent urology follow-up, which would lead to underestimation of 1-year retreatment rate by Kaplan–Meier estimates due to censoring. The 1-year retreatment rate for PUL in the study was 10.2%, consistent with the 1-year retreatment rate of 5.2%–11% from prior real-world studies. 10,13,14,26
Our study has several limitations. The retrospective design introduces selection bias. Postoperative symptoms were retrospectively assessed rather than captured from standard questionnaires, which may result in underreporting of these symptoms. Patients in the study also had variable follow-up time and incomplete data, both of which further introduce bias in the study. Patients who were satisfied with their urinary stream after the procedure may be less likely to receive Uroflow measurements and AUA-SS questionnaire despite continued follow-up. Prostatic median lobe size measurements could not be reliably extracted from patient charts and their effects on treatment efficacy could not be assessed. Differences between pre- and postoperative medication utilization were reported as binary differences without consideration for complex changes in medication utilization over time during the postoperative follow-up.
The PUL cohort had significantly lower sample size compared to the WVTT cohort. Conclusions drawn from subgroup analyses were also limited by the small sample sizes, especially in the subgroup with prostates 50–80 cc. Future prospective studies comparing the efficacy of WVTT and PUL in treatment of BPH LUTS are needed to address these limitations.
Conclusion
PUL and WVTT are both effective MIST treatments for BPH. WVTT patients more often reported dysuria and nonclot-related retention, whereas PUL patients more frequently experienced clot retention. WVTT may be more effective than PUL in patients with moderately large prostate sizes from 50 to 80 cc. Further prospective investigations are needed to directly compare PUL and WVTT to confirm the findings of this study.
Footnotes
Authors' Contributions
C.P.C., E.B.G., J.S.A., and M.A.P.: project development, data collection, data analysis, and article writing/editing. K.T.R., D.S., O.O., and M.L.: project development, data collection, and data analysis. D.Q.: data collection and article writing/editing. R.V., A.R., S.M., J.M., and C.N.: data collection and article writing/editing. M.G., A.C.S., and S.A.K.: data collection, data analysis, and article writing/editing.
Author Disclosure Statement
S.A.K. is the principal investigator for Urotronic, Inc., and ProVerum Ltd.
Funding Information
The study was performed at the Icahn School of Medicine at Mount Sinai without any external funding.