
Abstract
Purpose:
Ureteral stenting following uncomplicated ureteroscopy (URS) is common practice. Several studies have proven the safety of omitting routine stent placement following distal ureteral stone treatment. However, there is a paucity of data regarding the utility of stent placement for proximal URS. We designed a prospective, randomized controlled trial to evaluate the role of ureteral stent placement following URS for proximal ureteral and renal stones.
Methods:
Seventy-two patients with proximal ureteral or renal stones measuring as much as 1.5 cm were prospectively randomized into stented (37) or unstented (35) groups. The surgeon was blinded to the treatment group until after stone treatment. Patients tracked postoperative pain medications and completed validated pain questionnaires on postoperative days 0, 3, 7, and 28. Stents were removed on postoperative day 7. Postoperative follow-up imaging was obtained at 4 weeks.
Results:
No statistical differences were observed between the two groups in terms of demographics or stone characteristics. The operative time was longer in the stented group (p < 0.03). Patients in the stented group had more irritative urinary symptoms (p < 0.0001) and pain (p < 0.0001), missed more days of work (p < 0.01), and used more narcotics (p < 0.0005) during the first week, but no differences were observed at 30 days. Emergency room visits and overall complication rates were similar between the two groups. Three nonstented patients required stent placement. Two stented patients required early stent removal. Urinary tract infections developed in three stented patients, but not in unstented patients. Postoperative imaging did not reveal any hydronephrosis in either group, and the total stone-free rate was 94%.
Conclusions:
For most patients undergoing uncomplicated ureteroscopic treatment for proximal ureteral and kidney stones, it may be safe to omit ureteral stents to potentially decrease urinary symptoms and pain while improving short-term quality of life. Further studies with larger patient cohorts may be warranted to confirm our results.
Introduction
The prevalence of kidney stone disease is 9% in the United States. 1 –3 Ureteroscopy (URS) for urinary stones smaller than 1.5 cm is recognized by the American Urological Association 4 and European Association of Urology 5 guidelines as an appropriate first-line treatment option. Ureteral stents following URS are placed to prevent potential renal colic and ureteral obstruction and delay ureteral stricture formation. 6 –8
Recently, an international Endourology Society (Clinical Research Office of the Endourological Society [CROES]) study on ureteral stenting following URS indicated that stents were placed in >80% of cases undergoing renal stone treatment. 9 Despite their significant usage following URS, ureteral stents can be associated with increase in pain and lower urinary tract symptoms, decrease in quality of life scores, and increase in analgesic requirement. 10 –14
In 2003, Joshi et al reported increased pain and urinary symptoms and decreased quality of life in 80% of their patients. 15 This study developed a validated quality of life tool titled the Ureteral Stent Symptoms Questionnaire 16 (USSQ). 17,18 In view of the negative effects of ureteral stents on patient satisfaction, several studies have reported that routine stent placement following uncomplicated URS, especially for distal ureteral calculi, may be safely omitted. 19 –23
However, there is a paucity of data specifically evaluating upper ureteral and kidney stone URS treatment without placement of a ureteral stent. Therefore, we sought to evaluate the role of ureteral stent placement, following URS of proximal ureteral and renal stones, in patient satisfaction, safety and efficacy, and unplanned medical visits. We conducted a prospective, surgeon-blinded, randomized controlled trial of ureteral stent placement following URS in proximal ureteral and kidney stone patients.
Materials and Methods
After receiving institutional review board approval (C.2017.070), we conducted a prospective, randomized controlled study between May 2017 and April 2020 (
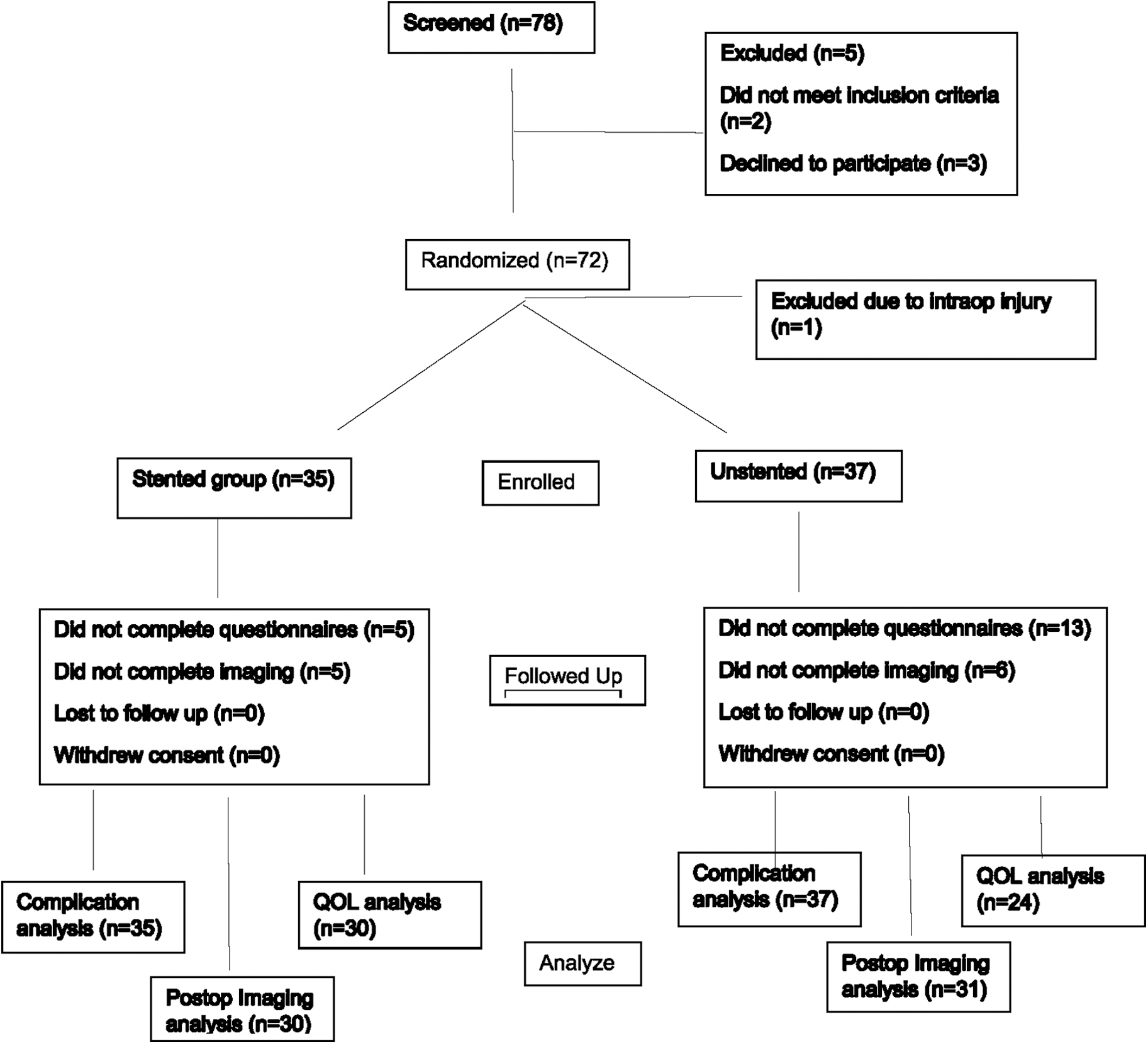
Study flow diagram for URS randomization of ureteral stent placement or omission. URS = ureteroscopy.
Group sizes were determined based on the clinically relevant USSQ score effect size of 5 U, with a conservative SD of 7 U, in which the power analysis for our noninferiority study equated to 35 subjects per group with power set at 80% and alpha at 0.05. All patients had at least one stone within the proximal ureter or kidney, and after appropriate counseling of the criteria for stone surveillance vs surgery, patients elected to proceed with URS for definitive treatment. For our study, eligible proximal ureteral stones were those located above the superior border of the sacroiliac joint.
All eligible patients were stratified according to patient age, gender, and stone location and randomized using a random number generator. The surgical team was blinded to randomization of the treatment group until the stones were treated, at which time, the treatment group was revealed, and a ureteral stent was either placed or omitted. No additional stone treatment was performed after the treatment group was revealed.
Our inclusion criteria included adults with unilateral proximal ureteral and/or renal stones measuring as much as a cumulative total of 1.5 cm. Preoperative imaging consisted of CT scans or plain film (kidney, ureter, and bladder radiograph [KUB]). Our exclusion criteria included cumulative stone size >1.5 cm, solitary kidney, pregnancy, evidence of active infection, or presence of distal or mid-ureteral stones.
Patients who were pre-stented or with nephrostomy tubes were excluded. The only intraoperative exclusions were ureteral perforation (visualized periureteral fat and/or ureteral extravasation of contrast medium on retrograde pyelogram) or the absence of a proximal or renal stone during URS. Of note, renal extravasation of contrast medium, such as for pyelovenous backflow, was not an exclusion criterion.
Our primary goal was to evaluate patient outcomes of urinary and pain symptoms, effects on quality of life, and medication usage. Our secondary goal was to evaluate unplanned medical visits and short-term complications.
Surgical technique
Patients underwent general anesthesia, had negative urine cultures, and received guideline-based antibiotics. A 6.9F distal tip semirigid ureteroscope (Olympus, Center Valley, PA) was used for ureteral stone cases with direct access to the ureter without balloon dilation of the ureteral orifice. A flexible (Karl Storz, Tuttlingen, Germany; Flex-X2™) or LithoVue™ ureteroscope (Boston Scientific, Marlborough, MA) was used for all kidney stones.
Ureteral access sheaths (UASs) were used at the surgeon's discretion. Small stones were removed—intact or, otherwise, fragmented with holmium:YAG laser of various settings—using endoscopic basket or dusting techniques.
After the stone was completely treated, the treatment arm was revealed to the surgical team. In the stented group, cystoscopic placement of a 6F-diameter stent with appropriate length was based on patient anatomy. Intraoperative medications were given at the discretion of the anesthesia team. Postoperative medications were standardized: hydrocodone/acetaminophen (5/325 mg), ibuprofen (600 mg), phenazopyridine (200 mg), and tolterodine (4 mg).
Patients were on alpha blockers before surgery and continued until stent removal. Patients kept track of medication use for the first 7 days postoperatively. Our study protocol was initiated before the transition away from post-URS narcotic usage. All stents were removed using a string on postoperative day (POD) 7, and all patients in both groups received one dose of levofloxacin (unless contraindicated) on POD 7 to avoid impacting urinary tract infection (UTI) data comparison between the groups.
All patients were discharged home the day of the surgery.
Outcome measures and follow-up
In both groups, we recorded operative times, use of access sheath, use of safety wire, stone size, and stone-free status. Outcomes were assessed using USSQ forms on the day of surgery and postoperative days 3, 7, and 28. Stone-free status was determined by KUB, renal ultrasound, or CT scan 4–12 weeks following surgery.
Short-term complications were determined by chart review for unplanned emergency room (ER) visits, hospital admissions, and stent placement or early removal.
Statistical analyses
Categorical data were summarized using counts with percentages and analyzed using chi-squared tests or Fisher's exact test, as appropriate. Medians and interquartile ranges were used as summary statistics for continuous variables and analyzed using Wilcoxon's test. A repeated-measures analysis of variance (ANOVA) was performed to compare USSQ metrics over the course of the hospital stay.
The post hoc analysis was adjusted using Tukey's method. Significance of results was established when p-values were <0.05. All statistical analyses were performed using JMP, v13.2 (SAS Corp).
Results
A total of 72 (two intraoperative exclusions) consecutive patients with eligible stones treated with URS were randomized to either the group with ureteral stent placement, 35 patients, or with no stent, 37 patients (Fig. 1). There were no significant differences between the groups in terms of patient demographics or stone characteristics (Table 1). Mean patient age was 50 ± 13 (stented) and 52 ± 13 (nonstented) years (p = 0.566).
Patient and Stone Characteristics for Ureteroscopy of Proximal Ureteral and Kidney Stones
Thirty-seven percent (stented) and 48% (nonstented) patients were female (p = 0.324). The mean stone size (longest diameter) was 7.9 ± 3.6 mm in the stented group and 7.7 ± 2.8 mm in the nonstented group (p = 0.917), with a range of 4 mm–1.3 cm. Stone location was similar between the two groups with 60% of kidney stones (p = 0.99).
Access to stones in all cases within both groups was achieved (100%), and UASs were used in 20% (stented) and 8.5% (nonstented) patients (p = 0.141). Direct visual inspection of the ureteral mucosa following UAS removal was performed and none of the patients with UASs were excluded for ureteral perforations. A semirigid ureteroscope was used for proximal ureteral stones and flexible ureteroscope for all renal stones.
Intraoperative exclusion (2 cases) included one case with ureteral perforation during semirigid URS and one with no proximal or renal stone on URS. Operative time (calculated from introduction of the endoscope to the final removal of the cystoscope ± stent placement) was significantly longer for the stented group, 55 minutes (interquartile range [IQR] 43, 74), compared with the nonstented group, 52 minutes (IQR 40, 57) (Wilcoxon p = 0.04), but not clinically significant.
Intact stone removal was performed in 8% stented and 11% nonstented patients (p = 0.634). The stone treatment was left to the surgeon's discretion for each case with regard to fragmentation and basket extraction or dusting techniques. During dusting, stones were fragmented to <3 mm, as per operative surgeon's estimations.
Follow-up imaging was available for 85.7% (stented) and 91.9% (nonstented) patients (p = 0.326) within the first 4–12 months. Treatment efficacy, defined as the radiographic absence of stones >2 mm, was 90% (stented) and 85.3% (nonstented) in the groups, which was not statistically significant (p = 0.227). There were no impacted stones that had eroded the ureteral mucosa in either group.
Sixty-four patients completed the USSQ assessment (Fig. 2a–c). Patients in the stented group reported significantly more dysuria, frequency, and urgency symptoms between the evening of surgery (34 vs 27; p = 0.001), POD 3 (34 vs 22; p < 0.0001), and POD 7 (31 vs 19; p < 0.0001); however, there was no significant difference by POD 28 (18 vs 18; p = 0.99).
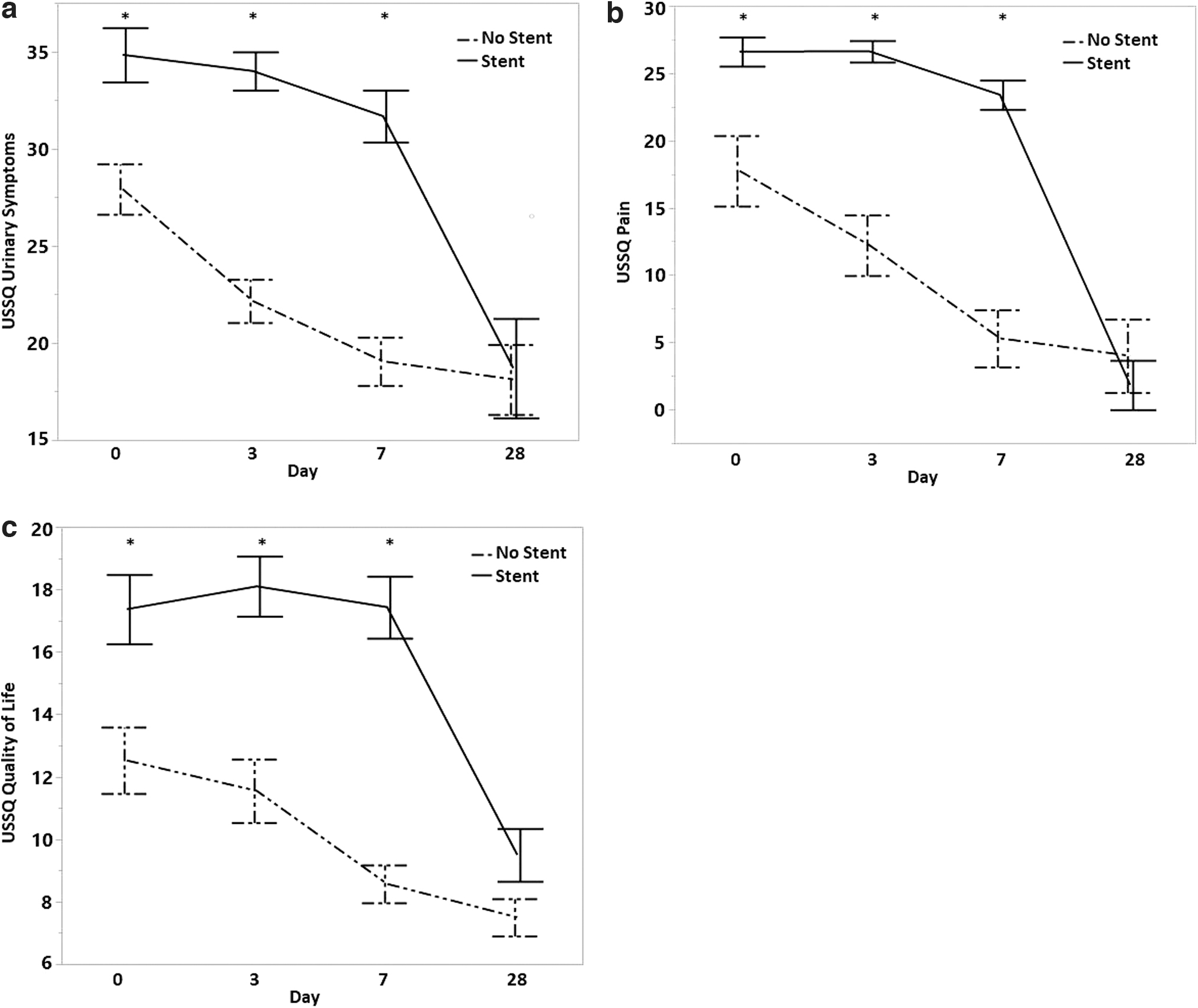
USSQ:
Overall pain scores were higher in the stented patients between the evening of surgery (28 vs 21; p = 0.007), POD 3 (26 vs 12; p < 0.0001), and POD 7 (23 vs 5; p < 0.0001), but pain scores were similar by POD 28 (1.8 vs 4; p = 0.59). Quality of life scores for stent patients were significantly higher on the evening of surgery (17 vs 12; p = 0.0068), POD 3 (18 vs 11; p < 0.0001), and POD 7 (17 vs 8; p < 0.0001), but similar by POD 28 (9.5 vs 7.5; p = 0.66). Furthermore, there was higher medication consumption by the stented patients (Fig. 3).

Medication usage following URS of proximal ureteral and kidney stones.
The overall complication rate between the two groups was not significantly different (p = 0.9) (Table 2). Of the 11 visits to the ER in the stented group, 6 had pain, without admission or intervention; 2 required early stent removal; and 3 required hospital admission (UTI, acute kidney injury, and nausea.) There were three total UTI cases in the stent group.
Complications Following Ureteroscopy of Proximal Ureteral and Kidney Stones
Fisher's exact test used.
AKI; ER = emergency room; n/a; UTI = urinary tract infection.
In contrast, all eight ER visits for nonstented patients were related to pain. Three patients required hospitalization for stent placement. There were no UTIs in the nonstented group. Postoperative imaging did not reveal any hydronephrosis in either group.
Discussion
URS has emerged as the first-line treatment for urinary stones <1.5 cm based on national guidelines 4,5 and operative trends. 2 The CROES URS Global Study revealed that over 90% of patients in the United States receive ureteral stents following URS. 9 Despite significant usage, several studies have shown that ureteral stents can worsen pain, lower urinary tract symptoms, and decrease the overall quality of life. 10 –12,14,15
Several studies have confirmed that routine stent placement following uncomplicated URS is not necessary for distal ureteral stones. 13,20,22 URS for proximal and renal stones is thought to be associated with longer operative times and possibly increased ureteral mucosal edema, which may benefit from a ureteral stent. 24 There is a paucity of data evaluating the safety and efficacy of omitting a ureteral stent following uncomplicated URS treatment for upper urinary tract calculi.
We performed a prospective, surgeon-blinded, randomized control trial (RCT) to assess safety, patient symptoms, complications, and unplanned medical visits related to stent placement vs stent omission following uncomplicated URS treatment of proximal ureteral and/or renal stones. To our knowledge, this is the first study that has exclusively evaluated the role of a ureteral stent following URS in this patient population.
In our series, all stones (100%) were treated in both groups using standardized semirigid and flexible ureteroscope equipment. The author uses a two-wire ureteroscope dilation technique for all proximal ureteral and renal stone ureteroscopic cases, which helps to increase the ureteroscope's access to proximal and renal stones. 25 While patient demographics and stone locations and sizes were similar between groups, we noted a slightly longer operative time of 3 minutes for the stented group (p < 0.03), which is clinically insignificant.
There are mixed results on operative times between these groups in the literature. 13,21 –23 For distal ureteral stones, Ibrahim and colleagues, 13 in a study on 220 patients, found a significantly increased operative time, while Damiano and colleagues 26 found equal times in their study with 104 patients. Our stone-free rates were 90% (stented) and 85.3% (nonstented), which are consistent with a retrospective matched cohort of upper ureteral and kidney stone URS cases with 86%–94% stone-free rates. 20
UASs were used in 20% (stented) and 8% (nonstented) patients and all were for renal stone treatment, which was not statistically significant, and no exclusions were made. UAS usage and its potential effect in our study may be limited due to the small sample size.
A 2019 Cochrane review by Ordonez and colleagues of ureteral stenting following URS management of urinary calculi determined that pain scores on the day of surgery until postoperative day 3 show little or no difference, but on day 4, stented patients show more pain; however, the authors commented that they are “very uncertain of this finding.” 27 However, the only RCT study of (distal) ureteral stone URS (measuring patient symptoms using the USSQ) by Shao et al revealed statistically significant worse overall symptoms for stented patients at 2 weeks from URS, specifically urinary frequency (p < 0.001), nocturia (p < 0.001), and pain in the kidney area at voiding (p < 0.001). 23
Our study yielded similar statistically significant scores within the stented group for pain, urinary symptoms, and decreased quality of life. In fact, the pain score differentiation between the comparative groups was largest at POD 7; median score was 23 (stented) vs 5 (nonstented) (p < 0.001). In addition, our patients' urinary symptoms and quality of life scores continued to similarly worsen for stented patients at POD 7.
This suggests that the longer the stent remains in situ, the worse the pain and urinary symptoms, compared with nonstented patients. However, by 4 weeks following URS treatment, the two groups have similar USSQ scores for pain, urinary symptoms, and overall health symptoms.
At study design, the majority of patients following URS were managed with opioid medications. 24 Our study demonstrated significant increase in pain and urinary symptoms in our stented group, which corresponded with a statistically significant increase in medication consumption.
Over the first 7 days following URS, the median cumulative number of medications consumed by the stented patients was 2.5 times higher for opioids (68 vs 25.5 MME; p = 0.003) and usage of ibuprofen, tolterodine, and phenazopyridine increased (Fig. 3). Admittedly, there is now a trend of eliminating opioid usage following URS treatment regardless of stent placement, but our study was initiated before this movement.
Our unplanned ER visit and hospital admission rates were similar between the stented (31.4% and 8.6%, respectively) and nonstented (21.6% and 8.1%, respectively) groups. Of the 11 stented patients with ER visits, 7 had pain issues; 5 cases had pain the same day following stent removal (none required reinsertion of the stent) and 2 required early stent removal. In the nonstented group, all eight patients had pain issues and three required stent placement (one distal stone and two ureteral edema cases) and admission.
In addition, we noted no UTIs with stent omission compared with 3 (8.5%) in the stented group. Unfortunately, due to our small patient numbers, it was not possible to perform a subset analysis of risk factors for unplanned visits.
There are few data regarding stent placement and unplanned visits. A meta-analysis by Pais and colleagues of 17 RCTs comparing ureteral stenting of mostly distal ureteral stones concluded that stent omission increased the odds of an unplanned visit by 60%. 28 A 2019 Cochrane review by Ordonez et al concluded that stent placement may decrease unplanned visits, but with low certainty of evidence. 27 In our study, stent omission favored (but did not reach significance) fewer unplanned visits and hospital admissions, but required three reoperations for stent placement compared with none in the stented group.
Regarding upper urinary stone URS, a review by Hollenbeck and colleagues 20 revealed a complication rate near 31% for stented patients with 72% being pain related, which is similar to our data with 64% (stented) and 100% (nonstented) of unplanned visits related to pain. Our military health system may increase patients' visits due to maximal access with minimal financial obstacles.
The current study may be limited by smaller patient numbers and operations performed by a fellowship-trained endourologist. Our single-institution military health system may not be generalizable to other health care systems. However, to our knowledge, our study is the first surgeon-blinded RCT evaluating the role of stenting following URS treatment of proximal ureteral and/or kidney stones.
Our only intraoperative patient exclusions were those with absence of eligible stones and a true ureteral perforation; otherwise, all the patients were enrolled and randomized to stent or nonstent groups. In addition, we used the validated USSQ for our patient outcome analysis. Our study results were analyzed irrespective of any previous urinary stone treatment as we did not track previous stone treatment in our data.
Conclusions
Stent omission following proximal ureteral and kidney stone URS treatment is safe and causes less patient pain, fewer urinary symptoms, and significantly less medication consumption. There were similar rates of complications and unplanned medical visits compared with the stented group; however, there may be a higher rate of reoperation.
Routine stenting following uncomplicated upper urinary tract URS may not be necessary. Larger studies are required to confirm our results.
Footnotes
Authors' Contributions
C.L.A. was involved in conceptualization, data collection, data analysis (equally), writing/original draft preparation (lead), and article editing (equally). J.K.A. was involved in statistical analysis (lead), data analysis (equally), and article editing (equally). A.M.R. was involved in conceptualization, data collection, data analysis (equally), and article editing (equally).
Disclaimer
The views expressed herein are those of the authors and do not reflect the official policy or position of the Brooke Army Medical Center, the U.S. Army Institute of Surgical Research, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army or the Department of Defense, or the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding.