
Abstract
Purpose:
We report results of a prospective, multicenter single-arm study of transurethral vapor ablation (TUVA) of prostate tissue in patients with unilateral, intermediate-risk, localized prostate cancer (PCa).
Materials and Methods:
Men ≥45 years of age with biopsy-confirmed unilateral Gleason grade group 2 (GGG2) adenocarcinoma of the prostate, prostate volume of 20–80 cc, and prostate-specific antigen (PSA) ≤15 ng/mL were enrolled. Cystoscopy and transrectal ultrasound (TRUS) guidance were used to deliver ∼103°C water vapor to prostate zones for unilateral hemigland ablation, including destruction of cancers detected by multiparametric MRI (mpMRI) and confirmed by biopsy. The primary outcomes were device-related serious adverse events (SAEs). At 7 days and 6 months postprocedure, the ablation extent was assessed by mpMRI; MRI/TRUS fusion biopsies were completed at 6 months. Quality of life (QOL) was assessed with validated questionnaires.
Results:
All subjects underwent a single hemigland TUVA procedure. No SAEs occurred. Grade 2 procedure-related AEs included transient urinary retention (n = 4) and erectile (n = 1) or ejaculatory dysfunction (n = 1). At 7 days, mpMRI revealed complete ablation of 14/17 (82%) visible lesions. At 6 months, biopsies showed no Gleason pattern ≥4 or ≥GGG2 cancer on the treated side of prostates in 13/15 (87%) subjects. Ten of 15 (67%) subjects were biopsy negative. Of the 5 biopsy-negative subjects, 2 had one core each of 3 + 4 disease and 3 had one core each of 3 + 3 disease with ≤5% involvement. Median prostate volume was reduced by 40.7% and PSA by 58%. Extensive QOL assessments showed, on average, no appreciable negative effects of treatment.
Conclusions:
Initial evidence suggests that TUVA is safe in men with intermediate-risk PCa. Preliminary results demonstrate the absence of ≥GGG2 disease on the treated side in 87% of men and a favorable QOL profile.
Introduction
Prostate-specific antigen (PSA) screening for prostate cancer (PCa) contributes to diagnosis of both clinically significant and insignificant cancers. Multiparametric MRI (mpMRI) and targeted biopsy have helped to increase diagnosis of significant cancers and decrease diagnosis of insignificant ones. 1 Despite advancements in robotic surgery and radiation treatment, the definitive treatment of PCa continues to carry the risk of side effects that can diminish quality of life (QOL), such as urinary incontinence and erectile dysfunction (ED).
The need to balance oncologic control with minimizing side effects has led to a variety of ablative energy sources and approaches for focal therapy being evaluated in clinical trials. 2 –6 Vapor ablation of the prostate has been proven to treat benign prostate hyperplasia (BPH). 7 It offers distinct benefits for focal therapy compared with other thermal modalities.
Water vapor delivered to a particular zone of the prostate is largely confined to that zone by the condensed collagen fibers surrounding the prostate and the pseudocapsule, 8 resulting in the excellent safety profile of this approach in treating BPH. 7,9,10 We report primary endpoint results of the transurethral vapor ablation (TUVA) device in an early feasibility, prospective, multicenter, single-arm safety study of unilateral ablation of prostate tissue in patients with intermediate-risk localized PCa.
Materials and Methods
Study subjects, protocol, and objectives
Men with Gleason grade group 2 (GGG2) unilateral PCa were treated and followed to the primary endpoint of 6 months in a prospective, multicenter, single-arm feasibility study performed in four centers in the United States (VAPOR 1 Study;
The Appendix lists key inclusion and exclusion criteria for this trial. Inclusion criteria included men with no prior PCa treatment and biopsy-confirmed, unilateral GGG2 adenocarcinoma of the prostate. Subjects had clinical stage ≤T2b disease, a prostate volume of 20–80 cc measured by transrectal ultrasound (TRUS), PSA ≤15 ng/mL, and no evidence of metastases.
The protocol was approved by institutional review boards at participating sites and research conducted in accordance with the Declaration of Helsinki. All participants signed a written informed consent.
The primary objective was to determine the safety of the TUVA procedure. Secondary objectives included evaluation of the effectiveness of TUVA in ablation of predetermined prostate tissue in the peripheral zone (PZ) and transition zone (TZ). The treatment strategy was hemiablation, including eradication of cancer identified through biopsy and mpMRI, to then support a further pivotal study of this novel technology.
Image acquisition and evaluation
All mpMRI studies of the prostate gland, including T2-weighted, diffusion-weighted, and dynamic gadolinium contrast-enhanced images obtained pretreatment, were assessed using the Prostate Imaging–Reporting and Data System (PI-RADS), v2.1, 11 by the site radiologist and a central study radiologist. Assessments confirmed the eligibility and absence of confounding structural abnormalities or aggressive malignant features such as extraprostatic extension.
MRI was repeated 7 days and 6 months after treatment to assess the ablation extent, evaluate for complications, and to plan the 6-month follow-up biopsy, distinguishing the treated vs untreated regions of the reshaped prostate following tissue absorption. At 6 months postprocedure, all patients underwent a combined 12-core systematic and MRI/TRUS fusion biopsy.
Specific sampling included cores from the treated areas as well as targeting of all lesions categorized as PI-RADS ≥3 on the untreated side and any lesions deemed by the central radiologist to be indeterminate or suspicious for cancer on the treated side. All images were reviewed using RadiAnt DICOM Viewer© software.
Thermal treatment procedure
The study procedure used an investigational device, the TUVA system (Poseidon System; Francis Medical, Inc., Maple Grove, MN), including a generator and transurethral delivery device with a cystoscopic lens, for hemigland ablation of prostate tissue containing biopsy-confirmed Gleason GG2 PCa under general anesthesia in an outpatient setting.
A transperineal needle was placed to inject saline into the space between the prostate and rectum to protect against rectal perforation or vapor leak in the unlikely event the posterior prostate capsule was unintentionally punctured. This was a precautionary measure only. The handheld delivery device deploys a temperature-resistant plastic needle transurethrally into the prostate under cystoscopic and ultrasound guidance. The needle could be advanced or retracted at 1-mm increments under real-time TRUS guidance to treat the TZ and PZ in all regions to achieve a hemiablation.
Water vapor (∼103°C) was then delivered through the needle and visualized with real-time TRUS. Interchangeable needle cartridges with different banks of emitter holes allowed customizable vapor delivery based on prostate anatomy. Water vapor was delivered in 10-second treatments, causing irreversible thermal ablation. The needle was then either repositioned along the same needle path for additional vapor cycles at adjacent sites or retracted and repositioned for treatment in another area of the prostate.
After the procedure, subjects were discharged with a urethral catheter. A video of the TUVA procedure is provided in Supplementary Material.
Assessments
The primary safety endpoints were device-related serious adverse events (SAEs) and secondary endpoints included treatment effectiveness as assessed by reduction in PSA and prostate volume, negative biopsy for Gleason pattern ≥4 on the treated side, and effect on QOL at 6 months. AEs were assessed at each clinic visit and adjudicated by an independent reviewer using Common Terminology Criteria for Adverse Events (CTCAEs), v5.0. 12 PSA levels were obtained at baseline and at 90 days and 6 months postprocedure.
Digital rectal examination, uroflowmetry, and urinalysis were performed at 6 months. The MRI was followed by a 12-core systematic TRUS, and MRI/TRUS fusion biopsy included targeting PI-RADS lesions ≥3 if present on the untreated side and any residual PI-RADS-equivalent lesions on the treated side, as determined by the site and central radiologists.
Validated questionnaires at 90 days and 6 months postprocedure were used to document the impact of treatment on lower urinary tract symptoms (lower urinary tract symptoms [LUTS] with International Prostate Symptom Score [I-PSS]), QOL (I-PSS-QOL, Expanded Prostate Cancer Index Composite-32 [EPIC-32] 13 ), and sexual function (International Index of Erectile Function [IIEF-15] and Male Sexual Health Questionnaire–Ejaculatory Dysfunction–Short Form [MSHQ-EjD-SF]).
Pelvic pain intensity was measured at 7 days, 30 days, and 6 months post-treatment on a 10-point numerical scale. 14
Statistical methods
Descriptive statistics performed with SAS, v9.4, described baseline subject characteristics and endpoints in the study. Data are presented as mean ± standard deviation, frequency as n (%), or median and range.
Results
A total of 26 subjects were enrolled in the study. The 15 qualified subjects were 49–78 years of age. Each treated subject had a single TUVA procedure between June and November 2020 and completed all assessments through 6 months postprocedure (Fig. 1). Baseline clinical characteristics are presented in Table 1.
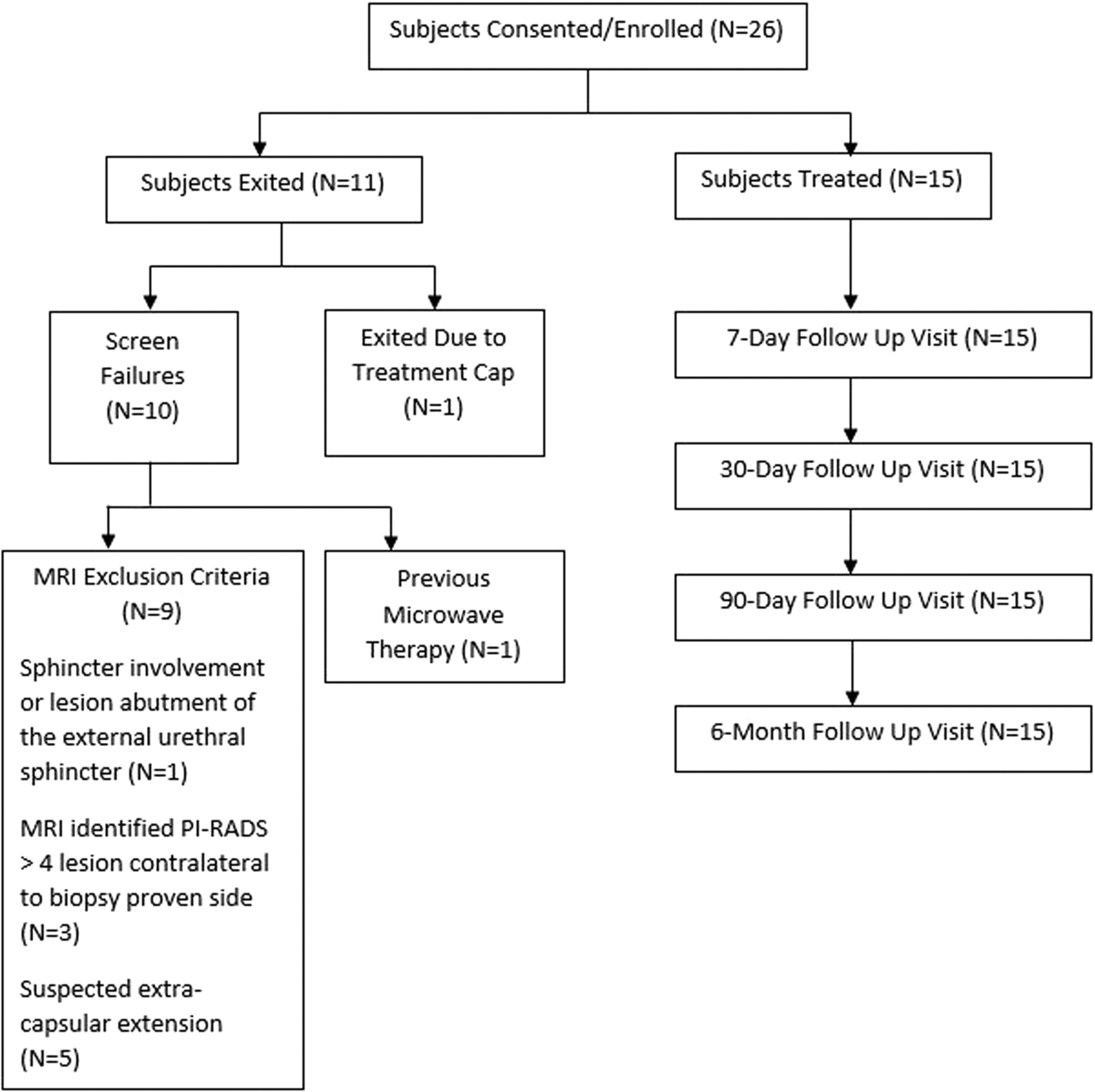
Flow diagram of subjects' disposition.
Baseline Clinical Characteristics of Treated Subjects (n = 15)
Positive targeted core count as one core even if multiple cores from target are positive.
I-PSS at enrollment, score range 0–35.
Erectile function at baseline determined by IIEF-5.
EjD at baseline determined with MSHQ-EjD-SF; maximum score is 15, indicating no EjD.
ED = erectile dysfunction; GGG2 = Gleason grade group 2; I-PSS = International Prostate Symptom Score; IIEF-15 = International Index of Erectile Function; MSHQ-EjD-SF = Male Sexual Health Questionnaire–Ejaculatory Dysfunction–Short Form; PSA = prostate-specific antigen; SD = standard deviation; TRUS = transrectal ultrasound.
All subjects had a history of LUTS at baseline, with urinary frequency and nocturia being reported most often by 10 (66.7%) and 11 (73.3%) subjects, respectively. Based on IIEF-EF scores, 8 of 9 subjects who reported mild or no ED at baseline were sexually active at 6 months postprocedure. Five subjects (33.3%) reported EjD at baseline.
All TUVA procedures were completed as planned. No device- or procedure-related SAEs or unanticipated adverse device events were reported. A total of 20 CTCAEs of grade 1 or 2 were reported among 8 subjects. The 14 procedure-related events were grade 1 (mild) in 8 and grade 2 (moderate) in 6 subjects. Of the 6 patients with grade 2 AEs, 4 had urinary retention and one each reported ED and EjD (Table 2). One patient with urinary retention had prolonged catheterization for >30 days with resolution at 44 days without sequelae. Four of the 14 procedure-related events were ongoing at 6 months.
Procedure-Related Adverse Events in Treated Subjects (n = 15)
All other events resolved without sequelae. Ten CTCAEs were adjudicated as procedure related; some subjects had more than one type of event.
Ongoing at the 6-month follow-up.
Resolved within 3 days; at the 90-day visit, brief intermittent penile pain lasting 1–2 seconds was reported as a sequela.
CTCAEs = Common Terminology Criteria for Adverse Events.
At baseline, a total of 17 MRI-visible lesions with PI-RADS scores of ≥3 were identified on the treated side among 14 subjects. One subject with a positive biopsy had no MRI-visible lesions, while one subject had 2 and another had 3 MRI-visible lesions on the treated side. The MRI evaluations at 7 days after treatment revealed 100% radiographic ablation of 14 of 17 (82.4%) MRI-visible lesions (Table 3).
MRI Assessment of Ablation of MRI-Visible Lesions at Seven Days Post-Treatment
SD = standard deviation.
Of the 17 MRI-visible lesions, 15 (88.2%) were in the PZ and 2 in the TZ. The efficiency of ablation relative to the location within the prostate zones and regions is shown in Table 4. Baseline and post-TUVA MRI findings from 4 of the treated subjects provide visual evidence of hemigland ablation of MRI-visible lesions, as shown in Figure 2.

T2-weighted MRI from four subjects showing the pretreatment locations and radiologist-determined size of hypointense targeted MRI-visible lesions (upper panel) and contrast-enhanced images at 7 days post-TUVA (lower panel). In the lower panel, areas of hypointensity were deemed to represent ablated tissue. TUVA = transurethral vapor ablation. Color images are available online.
MRI-Visible Lesion Ablation by Location at Seven Days Post-Treatment
In some cases, MRI-visible lesions were located in more than one prostate region. Five of 17 were in more than one region and one lesion was in all three regions (N = 23).
PZ = peripheral zone; TZ = transition zone.
Evidence of extraprostatic vapor was identified in 11 of 15 (73.3%) subjects at the 7-day MRI. The location of vapor escape was predominantly at the cranial base of the prostate near the junction of the prostate with the seminal vesicles and bladder. On MRI analysis, no detectable effect on adjacent organs was noted in 8 of these 11 subjects.
One subject demonstrated vapor effects on the seminal vesicle on the ipsilateral side, one showed focal bladder wall edema, and one had an effect on both the seminal vesicle and bladder edema. Subsequent imaging at 6 months demonstrated resolved bladder edema in both subjects and resolution of the effect on the seminal vesicle in one subject. There was no visible effect of vapor on the rectum, nor any clinical sequelae of extraprostatic vapor in any subject.
At 6 months, biopsies showed no Gleason pattern ≥4 or ≥GGG2 cancer on the treated side of the prostates in 13 of 15 (87%) subjects. Ten of 15 (67%) subjects were biopsy negative on the treated side. Of the 5 biopsy-positive subjects, 2 had one core each of 3 + 4 disease, and 3 subjects had one core each of 3 + 3 disease with ≤5% involvement (Table 5).
Effectiveness of the Prostate Cancer Transurethral Vapor Ablation Procedure
<5% core involvement.
Biopsy-confirmed GGG2 cancer in 2 of 15 subjects was associated with incomplete ablation of the MRI-visible lesion as seen on the 7-day MRI. Although one additional lesion appeared only partially ablated on the 7-day MRI, the 6-month MRI/TRUS fusion biopsy detected no cancer. Two of 15 subjects were positive for newly identified Gleason grade group 2 (GGG2) cancer on the contralateral untreated side. At 6 months, median reductions in PSA of 58% and prostate volume of 40.7% were observed; PSA increased in one subject.
Patient-reported QOL outcomes at 6 months after TUVA treatment relative to baseline showed no appreciable changes in mean EPIC-32 domain scores of urinary, bowel, or hormonal function (Table 6). IIEF-EF scores for the entire cohort decreased slightly at 6 months post-treatment.
Subject-Reported Outcomes at Six Months Post-Transurethral Vapor Ablation
Results presented as mean ± SD [range].
Higher score at a single point in time = better.
Lower score at a single point in time = better.
EPIC-32 = Expanded Prostate Cancer Index Composite-32; IIEF-EF = IIEF-Erectile Function; QOL = quality of life; TUVA = transurethral vapor ablation.
Among eight subjects with no or minimal ED at baseline who remained sexually active through the 6-month follow-up, two with mild ED had worsening EF scores; in one, the change was unrelated to treatment, whereas in the other, the relationship to treatment could not be determined. MSHQ-EjD function and bother scores were slightly diminished, while urinary symptoms and QOL improved; very low levels of pain were associated with the TUVA procedure (Table 6).
Discussion
Results of this initial safety and feasibility study indicate that TUVA treatment can safely provide hemigland ablation of prostate tissue containing Gleason GG2 adenocarcinomas. In particular, there were no rectal injuries, significant incontinence, or bladder injuries resulting in negative sequelae attributable to the procedure. Of note, this study achieved a similar safety profile as observed with vapor ablation and TZ only treatment for BPH 5,7 while routinely treating both the TZ and PZ of the prostate.
A need exists for PCa treatments that provide oncologic control while minimizing effects on QOL. Focal therapy attempts to strike this balance. Several focal therapies have been tested in clinical trials. 2 –6 While preliminary results are encouraging, there remain significant limitations and risks of side effects with these modalities.
Thermal modalities are challenged to attain the necessary temperature needed for tissue destruction within the prostate while not injuring surrounding tissues, including the rectum, neurovascular bundles, or the external sphincter, especially when attempting to treat cancers near the capsule. Since these modalities use thermal energy that spreads by conduction, distance provides the major temperature gradient between lethal and nonlethal thermal energy, largely ignoring anatomic borders.
TUVA offers a distinct alternative to conductive thermal energy since it spreads by convection and is generally confined by condensed collagen fibers surrounding the prostate capsule and pseudocapsule. Importantly, energy delivered within the prostate tends to stay in the prostate, limiting the potential for injury to surrounding structures. This theoretically provides the ability to treat disease abutting the capsule while maintaining a favorable safety profile, minimizing negative impacts on QOL.
The early assessments of the effectiveness of TUVA are encouraging. MRI/TRUS fusion biopsies at 6 months detected no GGG2 disease on the treated side in 86.7% of subjects. The TUVA procedure was able to treat biopsy-positive regions and MRI-visible lesions in the apex, mid, base, and anterior and posterior regions of the prostate, including lesions near the capsule.
Furthermore, it is anticipated that the currently observed excellent safety profile may be further improved by limiting application of vapor to biopsy-proven regions or MRI-visible lesions plus adequate margins, rather than hemigland ablation as was required per protocol, potentially limiting retention or ejaculatory dysfunction.
While one of the clear advantages of TUVA is that intraprostatic vapor delivery is bound by the prostate capsule and pseudocapsule, we observed evidence of vapor escape. This occurred nearly exclusively at the base, likely where seminal vesicles and ampullae of the vasa pass through the prostatic capsule.
Alternatively, it is possible that vapor could also be released outside the prostate through inadvertent capsular puncture sites during the procedure. Because vapor delivery is monitored by real-time ultrasound, it can be immediately stopped if extraprostatic vapor is suspected.
The characteristics of interstitial and surface ablation (extraprostatic vapor) are quite different. Interstitial ablation is rapid and complete because the vapor is under pressure in the gland. On the other hand, extraprostatic vapor is not confined within the prostate and is under greatly reduced pressure. This results in only surface ablation without deep tissue effects. Procedural and technical modifications in the application of this technology are anticipated to minimize extraprostatic vapor leak in the future.
Results of our study suggest limited decrement in urinary and sexual function in men undergoing TUVA, including no occurrence of serious urinary incontinence. Only two of eight subjects with normal EF at baseline who remained sexually active throughout the study period reported a significant decrease in EF. QOL questionnaires showing stable urinary and EF and minimal EjD for the majority of men suggest that the procedure may provide beneficial tissue ablation for men with intermediate-risk PCa with a relatively low risk for significant decline in QOL when performed as a hemiablation procedure, although further study is clearly required to confirm this.
While preliminary study results are encouraging, there are limitations to the data. Given the small number of patients and short-term follow-up, it is not possible to draw definitive conclusions from this initial experience. However, safety data support further study in a large-scale trial. Repeat procedures would likely be considered for patients with persistent disease and those with new lesions discovered on follow-up.
In summary, this initial report suggests that TUVA for prostate tissue containing intermediate-risk PCa appears to be a safe alternative in select men, demonstrating low levels of AEs for the population treated. The promising results support a pivotal trial to evaluate the effectiveness of this therapy in managing clinically significant PCa and further assess the risk–benefit profile of TUVA technology.
Footnotes
Acknowledgments
The authors acknowledge Michael Hoey for his invention of the technology of water vapor thermal therapy and the Francis Medical team for development and application of the TUVA procedure for treatment of PCa. The authors would like to thank Elaine K. Orenberg, PhD, for her assistance with the article.
Authors' Contributions
C.M.D. and C.A.W. were involved in conceptualization and design of the study, device design (supporting), and writing—creation of initial draft. C.M.D. was also involved in supervision—procedure proctor. B.S. was involved in analysis and interpretation of MRI data.
All authors were involved in conducting the clinical research, writing—review and revision, and final approval of the article.
Author Disclosure Statement
C.M.D. serves as a consultant to Francis Medical; R.M.L. serves as a consultant to Francis Medical and Boston Scientific; B.S. serves as a consultant to Francis Medical and Bot Image, Inc., and provides educational content to MRI Online; R.F.T. serves as a consultant to Nymox Pharmaceutical, American Gene Technologies, and Bayer; and C.H.C., M.R., S.J.M., and C.A.W. have no relevant conflicts of interests to disclose.
Funding Information
Support for the study was provided by Francis Medical, Inc., Maple Grove, MN.
Supplementary Material
Supplementary Video S1
Abbreviations Used
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.