
Abstract
Introduction and Hypothesis:
Robotic sacropexy (RSC) emerged in the last years as a valid alternative to the laparoscopic technique. However, the robotic approach is still limited by platform availability and concerns about cost-effectiveness. Recently, new robotic platforms joined the market, lowering the costs and offering the possibility to expand the robotic approach. The aim of our study was to demonstrate the technical feasibility and safety of the procedure with this new platform along with the description of our surgical setting.
Materials and Methods:
We reported data on the first five consecutive patients who underwent RSC at Onze Lieve Vrouw Hospital (Aalst, Belgium), performed with the novel HUGO™ Robot-Assisted Surgery (RAS) System. The platform consists of four fully independent carts, an open console, and a system tower equipped for both laparoscopic and robotic surgery. We collected patients' characteristics, intraoperative data, intraoperative complications, and clashes of instruments.
Results:
All procedures were completed according to the same surgical setting and technique. No need for conversion to open/laparoscopic surgery and/or for additional port placement was required. No intraoperative complications, instrument clashes, or system failure that compromised the surgery's completion were recorded. Median interquartile range docking, operative, and console time were 8 (6–9), 130 (115–165), and 80 (80–115) minutes, respectively.
Conclusion:
This series represents the first worldwide report of a robot-assisted sacropexy executed with the novel HUGO RAS System. Awaiting future investigation, this preliminary experience provides relevant data in terms of operative room settings and perioperative outcomes that might be helpful for future adopters of this platform.
Introduction
Pelvic floor dysfunctions are common urogynecological disorders, and affect up to 53% of women 50 years of age or older. 1,2 Among these disorders, pelvic organ prolapse (POP) affects more than 30% of women in Europe and United States causing discomfort and urinary incontinence, thus influencing the quality of life. 3,4 For these reasons, ∼11%–19% of all women in western countries undergo a surgical POP correction. 5 Moreover, the incidence—and associated morbidity—of POPs is likely to increase with the aging population and as such, there is a growing interest toward a durable, high-quality, and cost-effective POP treatment. For many women, surgical management of pelvic floor diseases represents the only option when conservative treatment is either impossible, undesirable, or ineffective. Although the vaginal approach is the most common surgical correction for all POPs, sacropexy can be considered the gold standard for apical prolapse. 6
Prior randomized controlled trials demonstrated the superiority of laparoscopic techniques as compared with open surgery in terms of morbidity, blood loss, cosmetic results, and length of stay. 7 –9 In this context, robot-assisted sacropexy (RSC) was originally introduced in 2004 and rapidly emerged as a valid alternative to traditional laparoscopy. 10 –12 Indeed, the robotic approach is associated with improved dexterity, precision, easier suturing of the mesh, closer visualization, and objective cure rates that range from 97% to 100%. 13 On the contrary, laparoscopic sacropexy requires demanding surgical skills to perform dissection of the vesicovaginal and rectovaginal spaces, suggesting that robotics could affect procedural learning curves and surgeons might need fewer cases to reach proficiency. 14 Despite these considerations, laparoscopy still represents the most common approach for sacropexy. Recently, several robotic platforms are emerging as contenders for the leadership in robotic surgery, bringing innovative and/or cheaper solutions into the market. 15
The continuous technical refinements and the overall reduction of procedural costs might therefore increase the access to robotic surgery. In this context, the HUGO™ Robot-Assisted Surgery (RAS) System (Medtronic©) recently received the Conformité Européenne mark approval for gynecological and urological procedures in adults. The aim of our study was to describe the first worldwide series of sacropexy performed with this novel robotic platform.
Materials and Methods
Patients' characteristics and management
We collected data of the first five consecutive patients who underwent robotic sacropexy (RSC) at Onze Lieve Vrouw (OLV) Hospital (Aalst, Belgium) between February 21st and April 5th, 2022 (Institutional Review Board Approval No. 2021071). All procedures were performed by three experienced robotic surgeons (R.D.G., G.D.N., and A.M.). Preoperative assessment included personal medical history, physical examination, and urodynamic evaluation. Prolapse was classified in accordance with the pelvic organ prolapse quantification (POP-Q) system released by the International Continence Society (ICS). 16 Patients' characteristics, as well as intra- and postoperative characteristics were collected. Specifically, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, POP-Q stage, previous hysterectomy, docking time, operative time, clashing of the instruments, technical errors or system failures, estimated blood loss, intra- and postoperative complications, length of stay, and catheter removal were recorded.
Surgical results were described according to the International Urogynecological Association (IUGA) and the ICS joint terminology for pelvic floor disorders. 17 A 0–10 visual analog pain scale (VAS) was used to assess pain 24 hours after surgery. Finally, a physical urogynecological examination was performed in all patients on the day of discharge using the POP-Q system.
Study endpoints
The main goals of the study were to demonstrate the technical feasibility and safety of robot-assisted sacropexy with the HUGO RAS System, along with the description of the surgical setup in terms of trocar placement, carts disposition, and docking angles (DAs). Moreover, we reported patients' characteristics and their intra- and postoperative outcomes.
The HUGO RAS System
The new HUGO RAS System consists of one system tower, an open console, and four independent arm carts, offering the choice of three or four-arm configuration depending on the procedure and surgeon's preferences. Each arm cart has six hinges with seven degrees of freedom, increasing the range of motion and the length of the arms. These features combined with the possibility to set the tilt angle (TA) of each arm lead to an easy trocar placement, and a low risk of external, as well as internal collisions. The patient cart positioning, trocar placement, and docking procedure are facilitated by the official setup guide, which provides these settings for each type of surgery. That said, the versatility of the system allows to change the official configuration according to surgeons' preferences. Finally, the compact configuration of patient carts allows easy transportability and storage.
The system is equipped with a Karl Storz™ endoscope and a Valleylab™ FT10 Electrosurgical generator, allowing both robot-assisted and traditional laparoscopic procedures. The three-dimensional (3D) high-definition laparoscopic camera, available with a 0° or 30° lens, is enclosed in a dedicated robotic adaptor and placed in an 11-mm port, while the other robotic instruments are placed in 8-mm trocars. The camera can be flipped by the bedside assistant or the scrub nurse manually by rotating the robotic adaptor or digitally pushing a button inserted directly on the camera. The camera can also be digitally flipped directly from the console by the surgeon. The Tower is also connected with Digital System 1 (DS1), a smart computer with built-in anonymization and protection capabilities, which provides automated analytics after surgery and enables easy but secure access to surgical videos on Touch Surgery™ App.
The open console is provided with a 32-inch-wide liquid–crystal display with an EIZO™ 3D screen and 3D glasses with a head-tracking system. Each console is equipped with a HUGO task simulator, allowing surgeons to learn and practice instrument moving, camera control, electrosurgery application, needle driving, and suturing. The console is provided with “pistol-like” hand controllers with an in-built clutch to activate or lock the robotic instruments. The surgeon can also customize several settings according to his preferences, such as rotation multiplier, motion scaling, and screen vision settings through the small interactive display placed on the right of the console. Finally, the pedals control camera, clutch, fourth arm, monopolar and bipolar energies, including a specific pedal for the Ligasure™ technology instruments. The instruments currently available include monopolar curved shears, bipolar fenestrated grasper, bipolar Maryland forceps, large and extra-large needle drivers, Cadiere and Secure Cadiere forceps, double fenestrated grasper, and toothed grasper.
Patient positioning, trocar placement, and docking procedure
Patients were positioned in a dorsal lithotomy position with the legs supported by Allen stirrups and the arms tucked beside the body. One 11-mm endoscope port was placed above the umbilicus ∼16 cm from the pubic bone. The other three 8-mm robotic ports were placed under vision at least 8 cm far from each other. According to the Medtronic setup guide, the right and left-hand trocars were positioned along a transversal line 5 cm below the optic port, whereas the fourth arm trocar was positioned on the same transversal line of the optic port. Finally, one 12-mm Airseal trocar for the assistant was positioned in the right hemiabdomen. The patients were set in a 20° Trendelenburg position (Fig. 1).
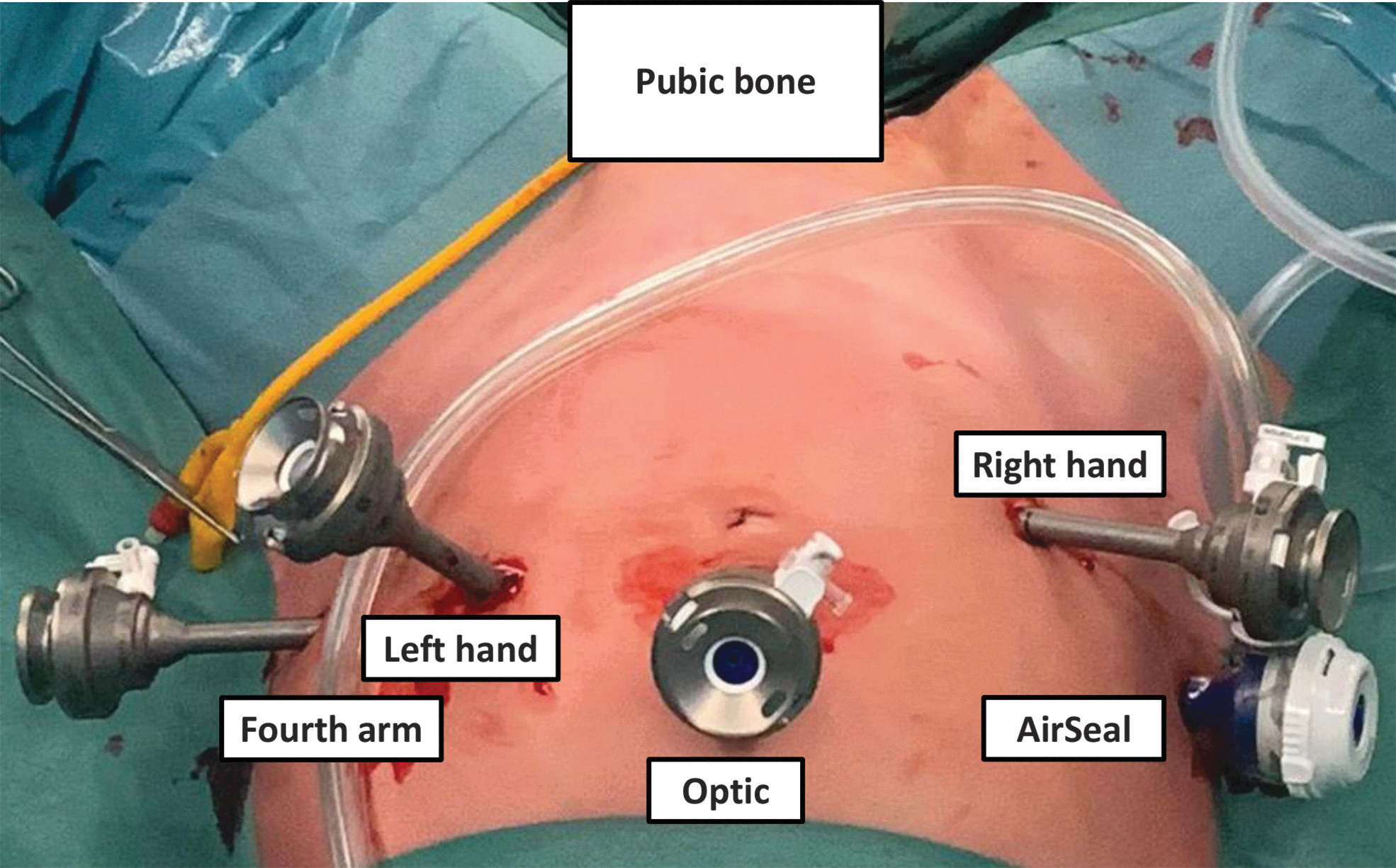
Trocars placement for robot-assisted sacropexy. The optic trocar is an 11-mm trocar, whereas all other robotic trocars are 8 mm. Assistant trocar is 12 mm. 5 Color images are available online.
To optimize the space in the operative room, two arm carts were positioned on the left side of the operative bed, one between the patient's legs and one on the right side of the operative table. While the bedside assistant worked on the right side between the bed and the system tower, the scrub nurse worked on the left side of the patient, with an easy access to the left robotic arms and enough space to manipulate the vaginal spatula. Finally, two additional screens were installed to allow the nurse and bedside assistant to have a complete vision from every angle (Fig. 2).

The setting of the operative room for robot-assisted sacropexy using the new HUGO Robot-Assisted Surgery system. Color images are available online.
Considering that HUGO has independent arm carts, a step-by-step docking procedure is mandatory. The endoscope arm cart coming between the legs is docked first. To minimize docking time, the right side and the left side carts were docked simultaneously by the bedside assistant and the scrubbed nurse, respectively. Considering the lithotomy position, docking of the right and left-hand arm carts may lead to collisions with the patient or with the operative bed. These collisions can be solved by adjusting the TAs, modifying the Trendelenburg angle, or increasing the angle between the lower legs and the abdomen.
The modularity and versatility of the system allow different TA and DA and different arm cart placement to optimize access to the surgical field. In our setting, DA and TA were as follows: endoscope DA 180°, TA −45°; surgeon left-hand DA 140°, TA −30°; surgeon right-hand DA 220°, TA −30°; fourth arm DA 105°, TA +30° (Fig. 3).

Arm cart disposition in the operative room during robot-assisted sacropexy using the new HUGO RAS system. Color images are available online.
Surgical technique
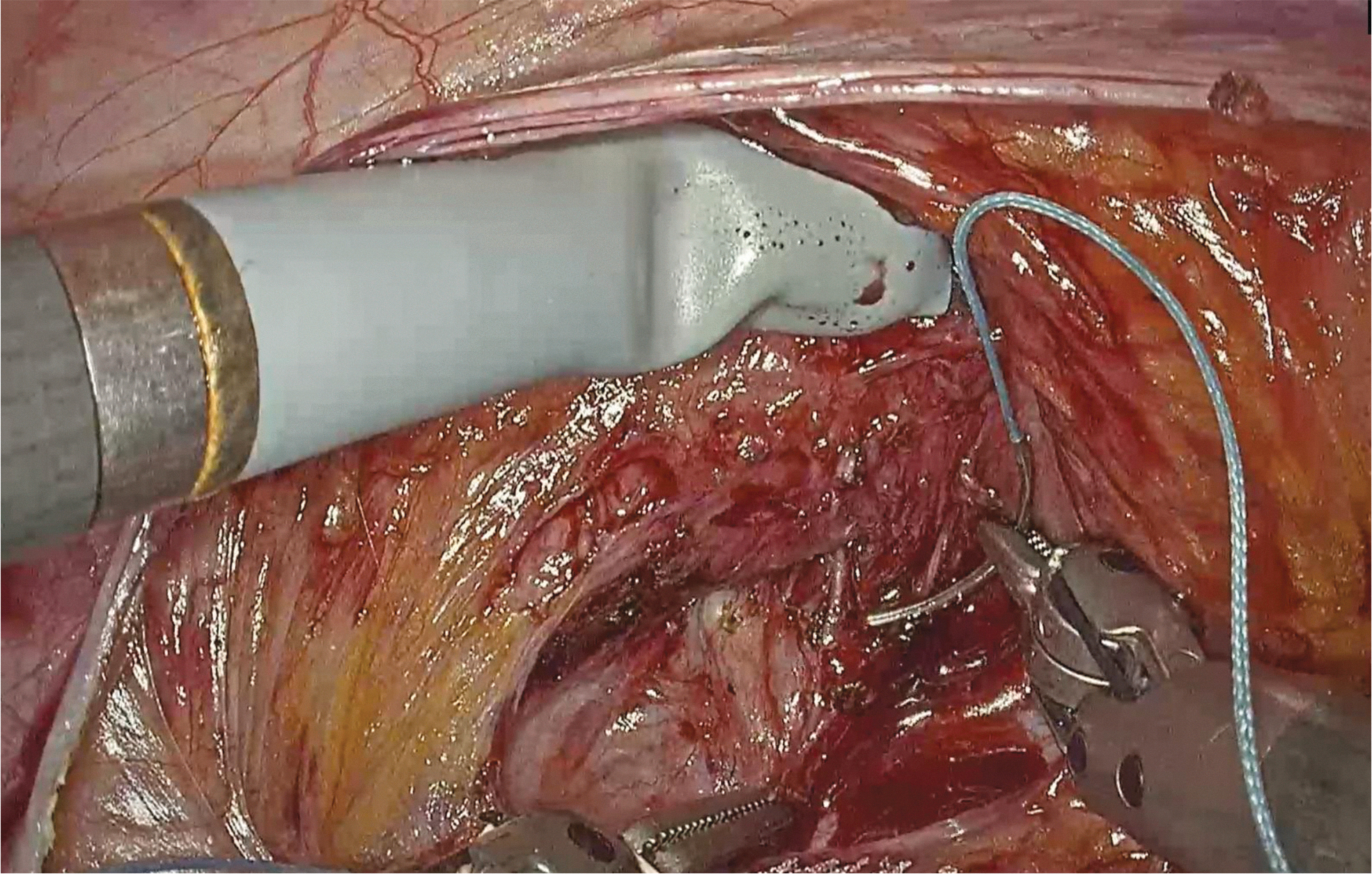
Monopolar curved shears, bipolar fenestrated grasper, and large needle driver were used in a three-instrument configuration with a zero-degree camera. A vaginal valve was used by the nurse to assist during the anterior and posterior dissection of the vaginal walls. Two “Y” preshaped knitted polypropylene monofilament Sacromesh Soft Prolaps (Cousin Biotech, Wervicq-Sud, France) meshes were used. All procedures were performed according to the following steps: urethral catheter insertion, trocar placement, right pararectal peritoneum opening, placement of a stay suture for upward retraction of the uterus (if present), dissection of the sacral promontory, dissection of the parietal peritoneum, creation of the tunnel, opening the Douglas space (Fig. 4) and dissection of the posterior vaginal wall (Fig. 5), fixation of the posterior mesh to the levator fascia/muscle and posterior vaginal wall with a nonabsorbable 0 Ethibond Excel (Ethicon Somerville, NJ, USA), insertion of the vaginal valve and dissection of the anterior vaginal wall, anchoring the anterior mesh on the anterior vaginal wall (Fig. 6), passing the meshes under the parietal peritoneum, fixation of the proximal parts of both meshes to the sacral promontory with a single nonabsorbable 2-0 Ethibond suture, and retroperitonealization of the meshes with a 3-0 V-Loc running suture (Covidien, Mansfield, MA, USA). 18

Creation of the subperitoneal tunnel. Color images are available online.

Dissection of the posterior vaginal wall. Color images are available online.
Fixation of the anterior mesh on the anterior vaginal wall. Color images are available online.
Statistics and Ethics Committee
Frequencies and proportions were reported for categorical variables. Median (± interquartile range [IQR]) were reported for continuous variables. All statistical tests were performed using SPSS 23.0 for Windows. The present study has been approved by the Institutional Review Board of the OLV Hospital, Aalst, Belgium.
Results
Median (IQR) age and BMI were 73 (56–76) years and 25 (22–28), respectively. The median (IQR) ASA score was 2 (1–2). All patients had a III or IV POP-Q stage for anterior and/or apical compartment prolapse. Two patients had previously undergone hysterectomy before they were referred to sacropexy. All procedural steps were completed with no need for conversion to open or laparoscopic surgery, or for additional port placement. No intraoperative complications, instrument clashes, or failure of the system were recorded. Median (IQR) docking, operative, and console time were 8 (6–9), 130 (115–165), and 80 (80–115) minutes, respectively. Median (IQR) estimated blood loss was 20 (10, 35) mL. Median (IQR) VAS 24 hours after the surgery was 3 (2–3). All patients removed the catheter on the first postoperative day, while the median (IQR) length of stay was 2 (1–2) days. Urogynecological examination performed on the day of discharge revealed no anatomic surgical failure, defined as a descent of the vaginal apex more than one-third into the vaginal canal or an anterior or posterior vaginal wall descent beyond the hymen. No perioperative complications were reported.
Discussion
In this clinical investigation, we demonstrated the feasibility and safety of robot-assisted sacropexy using the novel HUGO RAS System. We described our setup for this new robotic platform that resulted in no intraoperative complications, major issues, or conflicts among the robotic arms. Moreover, as compared with the official one, the disposition of the robotic arms in our setting, along with the configuration of DA and TA, increased the working space for both the assistant on the right side of the bed and for the nurse on the left side of the bed, allowing them to easily access all robotic arms. The creation of our operative setting was made possible by a thorough examination of the new platform before deploying the robot in a real operating room. Indeed, all components of the surgical team practiced in dry and wet laboratories, testing different operative set-ups for pelvic surgeries in human cadavers with the HUGO RAS System in ORSI Academy, Ghent, Belgium. 19,20 This work enabled us to create tailored and reliable configurations for urological and gynecological procedures covering both oncological and nononcological fields.
Moreover, the surgical team had already used the new robotic platform for pelvic surgery (i.e., 10 radical and 1 simple prostatectomies) before the first sacropexy. 21 The transition from Da Vinci to HUGO robotic platform was simple and almost immediate for both the bed assistants and the surgeons. All authors attended the preliminary official technical training course, which is key to understanding how to use the system modularity and its wide versatility in terms of patient positioning, trocar placement, and arm disposition. While the set-up time differs from the Da Vinci robotic platforms, the intraoperative experience is very similar for both the surgeon and the bedside assistant allowing a very short period for adaptation to the new system.
The modularity of the system and the versatility of the independent arm carts will allow every team to design appropriate combinations of trocar placement, number of arms used, patient cart disposition, TA, and DA based on the surgeon's preferences. The possibility to adjust the operating angle without modifying the port placement underlines the importance of this new robotic platform for multiquadrant surgery. However, we did not test this possibility in the case series herein reported. Although none of our patients required laparoscopic conversion, the system tower, endoscope, electrosurgical generator, and processors are designed to support both robot-assisted surgery and traditional laparoscopy. Finally, the open console features improved surgeon ergonomics. It also allows easy communication between the surgical team components and enables a better operative room awareness for the surgeon. The open console is also interesting for training purposes as observers can stand near the surgeon and thus have the same 3D vision through the glasses.
This study showed the feasibility and safety of robot-assisted sacropexy with the new HUGO RAS System. Overall, we observed excellent intraoperative and postoperative outcomes. Surgical time, blood loss, and postoperative functional outcomes were in line with the literature and with cases performed with the DaVinci platform at our Hospital. All the patients followed the standard postoperative management, which includes early catheter removal and early discharge. We did not report any postoperative complications. Expert surgeons performed all the cases, and this has to be taken into account when interpreting those outcomes. However, all the surgeons had performed very few cases with HUGO and were therefore still on their learning curve for this new platform.
To date, the wide diffusion of robotic surgery has been limited by platforms' availability and concerns about its cost-effectiveness. In addition, the robotic approach is mainly used for oncological surgeries, while the majority of functional surgeries are still executed with an open or laparoscopic approach. In this context, it is plausible that the introduction of new, well-equipped, and cheaper platforms like HUGO RAS might allow for larger adoption of robotics not only in oncologic surgery but also in functional urogynecology.
There are two major limitations in this study that could be addressed in future research. First of all, the present feasibility study is based on a small group of patients in a high-volume robotic center. Second, we did not provide long-term functional and complications data. Awaiting future investigation about cost-effectiveness and functional outcomes on larger cohorts of patients with longer follow-ups, this preliminary experience provides relevant data that might be helpful for future adopters of this surgical platform.
Conclusion
This is the first worldwide report of a robot-assisted sacropexy performed with the HUGO RAS System. The surgical team was able to set up the system, dock the robotic arms, and perform the surgery without technical issues and in line with the surgical time described in the literature. Excellent perioperative outcomes were recorded with the use of this novel robotic system.
Footnotes
Authors' Contributions
A.M.: Conceptualization validation, formal analysis, investigation, data collection and curation, writing—original draft, and visualization; C.A.B.: investigation, validation, writing—review and editing, data collection, and visualization; L.S.: investigation, validation, writing—review and editing, and visualization; M.P.: investigation, data curation, validation, and writing—review and editing; L.N.: investigation, data collection, validation, and writing—review and editing; A.P.: investigation, data collection, and writing—review and editing; P.P., P.D.B., and R.F.: investigation and writing—review and editing; R.D.G.: investigation, review and editing, and supervision; G.DN.: conceptualization, investigation, writing—review and editing, validation, and supervision; A.M.: investigation, writing—review and editing, and supervision.
Acknowledgments
The authors would like to thank Olivier Mahieu for his invaluable research assistance. The authors would also like to thank Romain Poncelet and Marianne Vandenlindenloof for their continued support regarding technical issues.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.