
Abstract
Introduction and Objective:
Robot-assisted partial nephrectomy (RAPN) has traditionally been performed as an inpatient procedure; however, recent studies have suggested the feasibility of same-day discharge (SDD) after RAPN. We aimed to evaluate the safety and cost-effectiveness of SDD for RAPN.
Methods:
A retrospective analysis was conducted on patients undergoing RAPN between January 2015 and July 2021. Comparison before and after the implementation of an SDD protocol was assessed through differences in postanesthesia care unit (PACU) time, length of stay, 30-day readmission rate, 30-day return to emergency department (ED) rates, unplanned office visits (OVs), and need for secondary procedures. A cost-efficacy model was generated to estimate the difference in expenditure between SDD and inpatient RAPN.
Results:
In total, 192 patients underwent RAPN with 74 being SDD and 118 being admitted postoperatively. After SDD protocol implementation, the percentage of patients discharged from the PACU increased from 0% to 76%. The safety profile of SDD was similar to the inpatient group, with no differences in readmission rates (1.4% vs 5.1%, p = 0.18) or return to ED (5.4% vs 9.3%, p = 0.33). Compared with inpatient RAPN, SDD was associated with increased time in PACU (375 vs 251 minutes, p < 0.001), resulting in an additional expenditure of $1,622 per patient. SDD patients were more likely to return for one or more unplanned OVs (17.6% vs 6.8%, p = 0.02). Overall, the total cost of SDD was significantly lower than inpatient RAPN ($5,222 per patient vs $8,425, p < 0.001).
Conclusion:
Despite a shorter postoperative monitoring period, SDD appears safe, with equivalent readmission rates, return to ED, and secondary procedures. SDD for RAPN saves ∼$3,000 per patient. In implementing an SDD protocol, clinicians should be cognizant of increased demands on PACU infrastructure and be willing to provide additional support in the office setting.
Introduction
In modern practice, partial nephrectomy has become the preferred management strategy for small renal masses in patients with sufficient life expectancy to warrant definitive intervention. 1 More recently, the advent and rapid adoption of robot-assisted partial nephrectomy (RAPN) have benefited patients because of demonstrated benefits in postoperative complication rate and length of stay vs traditional open surgery. 2,3 In addition to the benefits of robotic minimally invasive surgery, the development of enhanced recovery after surgery programs has demonstrated improvements in perioperative outcomes in other urologic cancer surgeries. 4 –8
These developments together have resulted in a clinical environment conducive to same-day surgery for certain urologic procedures. Several groups have recently reported on the safety and feasibility of same-day radical nephrectomy, 9 adrenalectomy, 10 radical prostatectomy, 11 or holmium enucleation of the prostate. 12 In addition to these safety and feasibility studies, recent studies on same-day discharge (SDD) in other traditionally inpatient procedures have demonstrated significant cost savings. 13,14 To date, the small number of studies examining ambulatory RAPN have contained small sample sizes and no examination of cost-effectiveness. 15,16
Our study aimed to evaluate the safety and cost-effectiveness of ambulatory RAPN in a large cohort undergoing RAPN for definitive management of small renal masses. We hypothesize the ambulatory approach to RAPN would have equivalent postoperative safety outcomes and would result in significant cost savings compared with traditional inpatient admission.
Materials and Methods
After institutional review board approval at Maimonides Medical Center, we performed a retrospective analysis of all patients at our institution aged >18 years who underwent an RAPN (Current Procedural Terminology: 50543), for management of a localized renal mass, between January 2015 and July 2021. An initial sample size of 210 patients was gathered using these parameters. Subjects were excluded if the partial nephrectomy was conducted for nononcologic reasons, if the patient underwent additional procedures, or if the renal procedure was miscoded as an RAPN (n = 18). This left a total of 192 subjects in the final analysis (Figure 1).
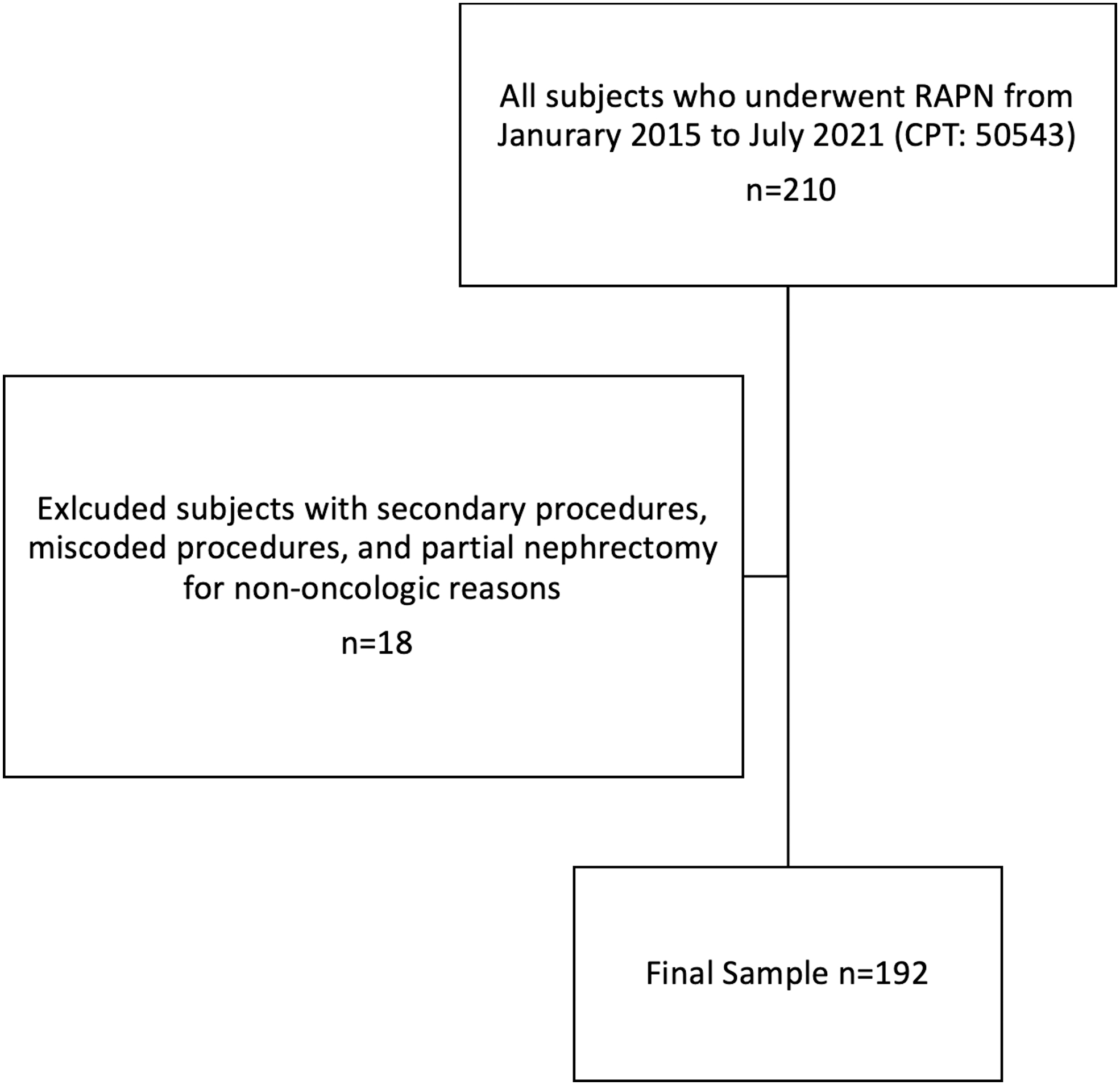
Sample selection figure. CPT = current procedural terminology; RAPN = robot-assisted partial nephrectomy.
Implementation of an SDD protocol started in June 2018. Within this voluntary protocol, all patients received preoperative counseling in an office setting regarding the expectation of SDD. Although a standardized script was not utilized in this study, all aspects within informed consent for participation in SDD were discussed by the five attending physicians involved with this study. Particular attention was paid to the patient understanding postoperative symptoms and avenues for seeking care, including an office visit (OV), calling the answering service to reach a physician, or going to the emergency department (ED). After a thorough discussion and addressing all concerns, any patient not comfortable with SDD was admitted and kept overnight. Patients were split into two groups for examination: those admitted to the hospital overnight, and those discharged home without admission (SDD).
Sample population
All procedures were performed under general anesthesia by four fellowship-trained surgeons on the da Vinci Xi system. Each operation was standardized across all surgeons to limit differences in technique impacting results. Bilateral Quadratus Lumborum blocks were performed by the anesthesia team before incision using 0.25% bupivacaine mixed 1:1 with liposomal bupivacaine. All procedures were performed in a partial flank position through a transperitoneal approach. Hilar control was obtained in >95% of cases and renorrhaphy was performed through a sliding clip technique with absorbable sutures. Minimization of intraoperative narcotics was prioritized by the anesthesiology team, with boluses of fentanyl given only when necessary.
No subjects had drains placed requiring postoperative removal. All patients were monitored in the postanesthesia care unit (PACU) for a minimum of 3 hours. Pain control was strictly non-narcotic and included an initial dose of intravenous (IV) ketorolac, with further doses of IV ketorolac as well as oral Tylenol given on an as-needed basis. Early ambulation was encouraged by the nursing staff once patients were sufficiently awake. After an initial trial of clear liquids, patients were advanced to a regular diet. A formal evaluation by a urology provider was performed before discharge to evaluate for suitability for discharge.
A decision for SDD required all of the following criteria to be met: (1) Patient is ambulating well, tolerating a regular diet, and pain is adequately controlled. (2) Surgery was sufficiently uncomplicated per the primary surgeon's discretion at the time of case completion. (3) Both surgeon and anesthesiologist agree upon the status of the patient's comorbidities do not warrant further monitoring. (4) Patient is amenable to SDD and understands the circumstances necessary to return to care. If any of these criteria were not met, the patient would be admitted for overnight observation and subsequently discharged when deemed appropriate. All patients were discharged with a 5-day supply of oral ibuprofen 600 mg for pain control. Every patient received discharge instructions, which included recommendations to return to the ED if they develop a fever, have persistent hematuria, heavy blood loss from their surgical incisions, severe worsening abdominal pain, malaise, or lightheadedness.
Cost estimation
A cost model was created to estimate the total postoperative cost per patient for each group based on PACU time, number of hospital days of initial admission, 30-day readmission rate, number of hospital days upon readmission, 30-day return to ED rate, and number of unplanned postoperative OVs. PACU time was estimated at a rate of $13/minute based on a previously published accounting study on PACU and operating room (OR) costs. 17 Unplanned OV costs were estimated according to published Medicare reimbursement schedules for medium complexity established patient visits within urology. 18 Inpatient admission and ED costs were estimated using the American Hospital Association Annual Survey and the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample databases. 19,20 This resource provides standardized charges for patients regardless of payer (Medicare, Medicaid, Private, or Uninsured), All cost estimates can be found in Table 1.
Cost Estimates for Postoperative Outcomes
ED = emergency department; OV = office visit; PACU = postanesthesia care unit.
Statistics
Baseline patient characteristics, including age, gender, comorbidities, American Society of Anesthesiologists (ASA) status, body mass index (BMI), and tumor size, were recorded. In addition, intra- and postoperative variables were examined, including estimated blood loss (EBL), operative time, PACU time, 30-day readmission rate, 30-day return to ED rate, and unplanned OV rate. Patients were allotted one planned postoperative OV within the first 3 weeks after discharge. Any additional visits within this 3-week time frame were deemed unplanned. Inpatient and SDD groups were compared on these metrics using chi-square and Student's t-test as appropriate.
Results
For a 6-year time frame, a total of 192 patients underwent RAPN. The average age was 59.5 ± 10 years and 120 (62.5%) were men. Five RAPN (2.6%) utilized an off-clamp approach. The average tumor size within the entire cohort was 3.32 ± 1.42 cm. Baseline clinical characteristics are summarized in Table 2. A total of 74 (38.5%) patients were discharged the same day vs 118 (61.5%) who were admitted for at least 1-day postoperatively. Following the implementation of SDD 76% of patients receiving RAPN were discharged the day of their surgery.
Sample Characteristics Stratified by Same-Day Discharge vs Inpatient Robot-Assisted Partial Nephrectomy
Bold represents statistically significant difference between the two groups for that particular variable.
ASA = American Society of Anesthesiologists; BMI = body mass index; EBL = estimated blood loss; IR = interventional radiology; OR = operating room; RAPN = robot-assisted partial nephrectomy; SDD = same-day discharge.
Of the 74 patients in the SDD cohort, 46 (62.1%) were men with a mean age of 58.9 ± 9.9 years. Twenty-nine (39.2%) patients were assigned an ASA score of 3, whereas the remaining 45 (60.8%) were assigned an ASA score of 2. Mean tumor size was 3.31 ± 1.28 cm. In terms of T stage, 50 (67.6%) of the patients were T1a, whereas the remaining 24 (32.4%) were T1b. There were no differences between the SDD and inpatient groups in terms of tumor size or T stage. Mean total operative time for the cohort was 172 ± 39 minutes. Mean intraoperative blood loss was 117 ± 177 mL. There were no intraoperative or postoperative blood transfusions.
Three patients returned to the ED within 30 days but were not admitted to the inpatient service. One patient experienced prolonged postoperative retention and came into the ED on postoperative day (POD) 7 with a clogged Foley. One patient returned with vague abdominal pain and subjective fever and was discharged home after an ED work-up. The final patient was treated in the ED for an asymptomatic hypertensive crisis identified on her scheduled follow-up visit. A single patient was readmitted on POD 13 with fevers and hypoxia and was found to have pneumonia secondary to coronavirus disease-19 [COVID-19] SARS-CoV-2 infection. She was treated conservatively and discharged home 5 days later. Thirteen (17.6%) patients required a postoperative OV, a large portion (53.8%) for a trial of void or recurrent urinary retention.
Univariate analysis
On univariate analysis (Table 2), SDD patients were more likely to have a shorter operative time (172 vs 194 minutes, p = 0.002), be the first case of the day (70.3% vs 50.0%, p = 0.006), have a longer PACU time (375 vs 251 minutes, p < 0.001), and require 1 or more unplanned OVs (17.6% vs 6.8%). There were no significant differences between the two groups with respect to age, BMI, ASA score, tumor size or stage, ischemia time, EBL, 30-day readmission, or 30-day return to ED. In a subgroup analysis of just those cases after the implementation of the SDD protocol, patients who were the first case of the day were more likely to be discharged home the same day vs those who were the second case or later (83.9% vs 62.9%, p = 0.019).
Cost comparison
In our postoperative cost model, SDD after RAPN was significantly cheaper than inpatient RAPN ($5,222 vs $8,425, p < 0.001) (Figure 2). Most of this cost difference was driven by the upfront cost savings associated with no initial inpatient hospital days in the SDD group ($0 vs $4,673). Some of these cost savings were offset by differences in PACU cost ($4,880 vs $3,258, p < 0.001). Importantly, the cost savings from the lack of initial admission was not offset by significant differences in return to ED or readmission costs.
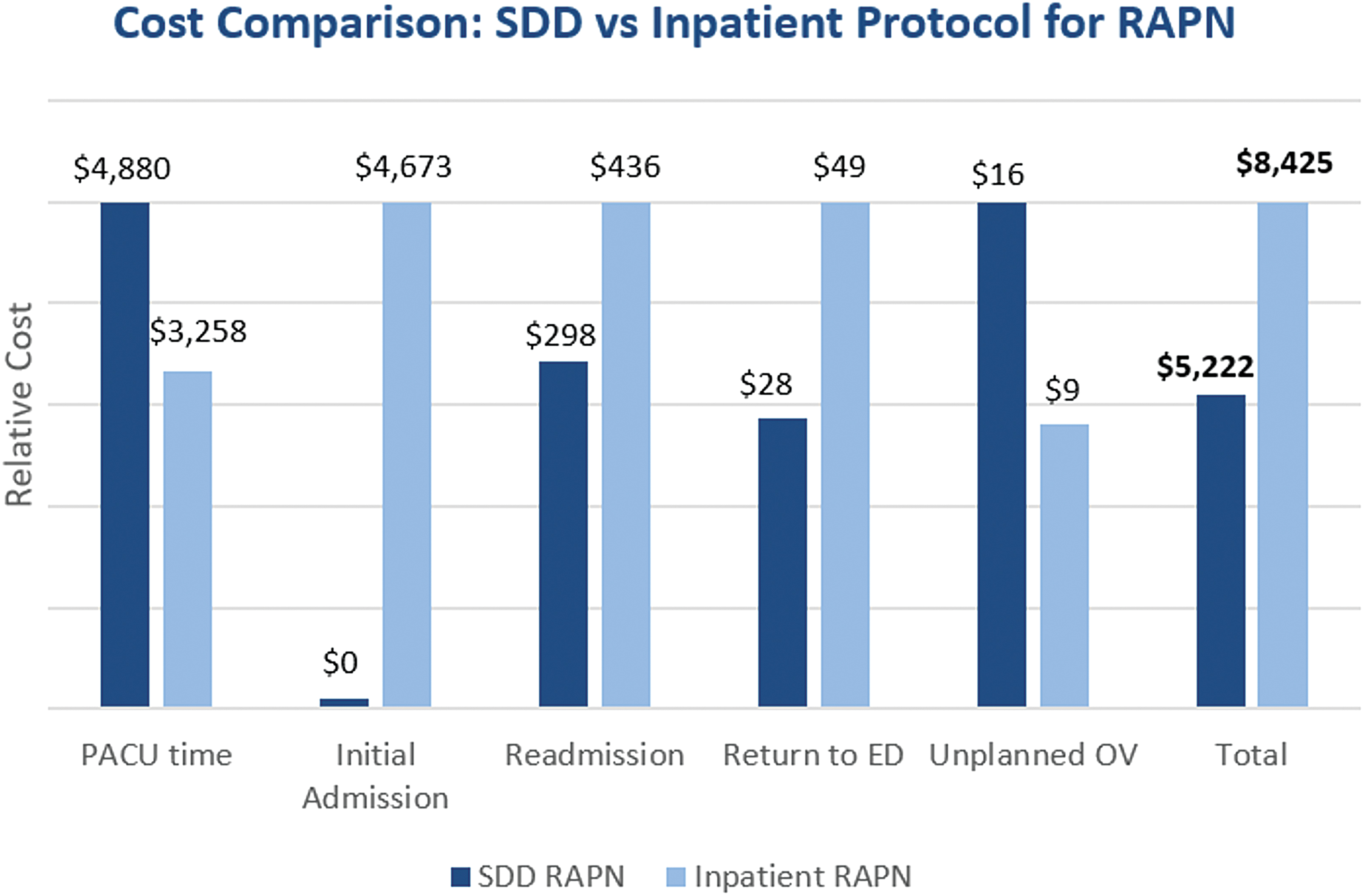
Cost comparison between SDD and inpatient protocol for RAPN. ED = emergency department; OV = office visit; PACU = postanesthesia care unit; SDD = same-day discharge. Color images are available online.
Discussion
To our knowledge, this is the first study to combine a report on the safety of SDD and an estimate of postoperative cost in patients undergoing an RAPN. There are several points of discussion.
The successful implementation of an SDD protocol begins with the patient and their preoperative counseling. Previous literature in SDD after radical prostatectomy showed that two-thirds of patients did not feel ready to be discharged the same day, which highlights the importance of patient preference when planning for SDD. 21 Within our study, all patients engaged in thorough discussions about what the SDD protocol entailed to provide expectations for both the patient and their support system. Patients not comfortable with SDD, or based on the surgeon's clinical judgment, were admitted for overnight observation.
Although a minority of patients within our cohort elected against SDD preoperatively, formulating a standardized checklist to counsel the patient may improve efficacy of SDD. Topics of discussion would include all aspects of informed consent (risk, benefits, alternatives, and complications), breakdown of surgical procedure, postoperative expectations regarding need for early mobility and pain control, and criteria that must be met to allow for SDD. 22 Engaging in these conversations systematically have shown to be effective in reducing postoperative complications and opioid use within certain surgical procedures. 23,24
In conjunction with verbal communication, patients can be given brochure material and videos to supplement the preoperative OVs to reduce fear and anxiety related to their procedure. 25 In addition, case timing can factor into the feasibility of SDD, which is evidenced by the admission rate falling from 24% to 16% in the subset of patients performed as the first case of the day. This is helpful when creating OR schedules as patients who have already opted out of SDD can be scheduled later in the day to provide ample time for SDD patients to meet discharge criteria.
Safety of SDD when compared with inpatient hospitalization is an important factor to assess. Within our results, SDD did not negatively affect patient safety as readmission rates and return to ED rates were no different when compared with inpatient RAPN. A single patient was readmitted within 30 days because of SARS-CoV-2-related illness, ironically emphasizing the importance of minimizing patient exposure to the health care system. In addition, a consequence of SDD was an increase in unplanned OV after discharge; however, we feel this to be a fair trade-off as longer hospital stays lead to a slower return to baseline, increased risk of infection, and harm from medical error. 26
Physicians may choose to implement a scheduled OV POD 2 to mitigate these unplanned visits and help patients address any concerns after their procedure. National data from National Surgical Quality Improvement Program (NSQIP) regarding SDD after nephrectomy provide similar findings. 27 Our study results complement these data as the NSQIP database only records 30-day outcomes as well as limited granularity of the patient's clinical course and oncologic characteristics. Nonetheless, the combined results provide growing evidence supporting the safety of SDD.
In terms of postoperative outcomes, SDD patients spent >2 hours longer in the PACU. The additional time spent in PACU, at least in part, represents the additional time needed to allow patients to meet all necessary milestones for discharge. A common problem in the PACU was the extended duration trial of void, a problem that has more recently been mitigated by a fill and pull method. Another approach can be to discharge patients with a Foley to avoid TOV in the PACU. In this instance, patients can be provided information about how to pull their Foley at home, minimizing the need for an OV.
Similar outcomes in SDD after partial nephrectomy were recently published by Benamran et al., providing more evidence that SDD after partial nephrectomy can be a safe means of postoperative care. 28 Surgeon experience, hospital resources, and, more recently, COVID-19 all factor into its feasibility and importance. Therefore, SDD for RAPN continues to be refined at our institution. Adjustment of the protocol based on our study and future studies will allow for more standardized criteria for SDD.
We found a significant cost advantage to SDD after PN as compared with patients staying overnight. Analysis revealed SDD after RAPN resulted in a cost savings of >$3,000 per patient. The largest and most obvious factor driving these savings is the lack of cost associated with postoperative admission. This was somewhat offset by the cost associated with increased PACU time, a factor worth considering by any hospital system considering a transition to an SDD pathway. Although there were significantly more unplanned OVs after an SDD approach, the magnitude of the impact on postoperative cost paled in comparison with admission, readmission, and PACU time factors.
Although cost considerations will always be secondary to patient safety concerns, they should not be neglected in the current atmosphere of ever-increasing health care expenditures. Prior studies in traditionally inpatient procedures have demonstrated that SDD can provide cost savings; however, the degree of cost savings is largely procedure, region, and health system dependent. 29,30 Estimates of cost-effectiveness using charges from a single hospital can often prove virtually meaningless to providers practicing in another state or care environment. It is for this reason that we chose to use various publicly available cost estimates, despite the potential loss in accuracy of estimation.
Whenever an SDD approach is attempted for a traditionally inpatient procedure, caution must be taken to ensure that any upfront cost savings are not negated by increased readmission and ED visit costs. Costs associated with readmission have garnered substantial attention in the United States as a key area for achieving potential cost savings. 31 According to recent studies, up to $45 billion per year is wasted on unnecessary hospital readmissions, and readmission costs are higher than initial admission costs for more than two-thirds of common diagnoses. 32 Our study provides the first evidence that not only is SDD for partial nephrectomy a safe approach with significant upfront cost savings, but these savings are not offset by increased readmission costs that might be particularly concerning in the current climate.
Our study is not without limitations. First, the retrospective nature of the study design introduces inherent biases, including selection bias. The cohort of our study was stratified as SDD or inpatient for a time period of 6 years within which an SDD protocol was implemented. This approach was undertaken to ensure an adequate sample size in the control/inpatient group to allow for meaningful analyses. Follow-up studies exclusively comparing patients after the introduction of SDD will be needed to confirm the safety and cost savings demonstrated in this study. These studies should also provide patient characteristics not available in our study, which include nephrometry scores, to provide an improved clinical picture of the cohort.
As mentioned earlier, we recognize that publicly available cost estimates (whereas location and specialty-specific where possible) are inherently less accurate than institution-level cost data. However, we see this as a benefit since the standardized approach can be more applicable across institutions. What is important is not the exact amount of difference, but that there was a difference at all, and that the difference measured in the thousands of dollars per patient. Despite these limitations, we were able to demonstrate the safety of SDD after RAPN in a relatively large relatively unselected patient cohort. We were also able to provide the first estimates of postoperative cost savings achieved by following an SDD protocol after RAPN.
Conclusion
SDD after RAPN is a safe and reasonable approach for most patients and results in significant cost savings vs a traditional inpatient approach. Providers and institutions considering implementing an SDD approach should be cognizant of increased demands on office and PACU infrastructure.
Footnotes
Authors' Contributions
Conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing by A.W. Methodology, formal analysis, and writing—review and editing by D.J. Methodology and writing—original draft by E.K.-M. and E.K. Conceptualization, methodology, and supervision by M.L., E.T., D.S., and A.S.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.