
Abstract
Introduction:
Previous studies of pediatric urolithiasis have suggested possible associations between the relative proportions of calcium oxalate dihydrate (COD) and calcium oxalate monohydrate (COM) stones with age, gender, and ethnicity. This study aimed to investigate the composition and distribution of calcium oxalate (CaOx) stones according to these clinical factors and the metabolic correlates of the different subtypes in pediatric stone formers (PSFs).
Patients and Methods:
We retrospectively reviewed the database of all first-time stone formers between 2014 and 2019. Infrared spectrometry was used to determine stone composition. Stones were categorized by their highest relative component and reported as a percentage of occurrences in the cohort as a whole and by patient gender, age (divided into three age groups: 1–5, 6–12, and 13–18 years), and ethnicity. Clinical and metabolic correlates were analyzed.
Results:
Of 2479 consecutive stones submitted to our chemical stone laboratory, 220 first-time PSFs were identified. COD stones were the predominant subtype in the youngest group, and COM stones in the oldest group (odds ratio 0.39, 95% confidence interval: 0.18–0.86, p = 0.036). In the intermediate-age group (6–12 years), COM stones were more prevalent in Arab boys, and COD stones in girls of either ethnicity. COD stones were associated with hypercalciuria (p < 0.0001), and COM stones with hyperoxaluria (p = 0.0024). Hypercalciuria and hypocitraturia were the most prevalent abnormalities at ages 1 to 5 and 13 to 18 years, respectively.
Conclusions:
Analysis of CaOx stone subtypes and their metabolic correlates in stone formers has significant clinical relevance, specifically in children. In the present study, COD stones and hypercalciuria were more common in younger children, and COM stones and hypocitraturia in adolescents. These findings suggest unique complex interactions driving stone formations in children that may guide a more practical, limited, and cost-effective approach to metabolic evaluations, choice of treatment, and preventive measures, particularly in first-time CaOx PSFs.
Introduction
The worldwide prevalence and incidence of pediatric urolithiasis have steadily increased in recent decades. 1,2 Compared with adults, pediatric stone formers (PSFs) have more recurrences, higher radiation exposure risks and intervention rates, and require longer follow-up. 1 –3 Complete metabolic work-up, including stone composition, is particularly important in children guiding the management and patient-specific preventive strategies to reduce long-term sequelae. 2,4,5
Up to 80% of urinary stones are composed of calcium oxalate (CaOx), 2,6,7 either monohydrate (calcium oxalate monohydrate [COM]) or dihydrate (calcium oxalate dihydrate [COD]) or their combination. In adults, COM stones are the most prevalent and associated with older age and hyperoxaluria. COD are associated with younger age, hypercalciuria, higher urinary pH and CaOx supersaturation, and higher recurrence and intervention rates. 6 –9 Children, however, have a different urinary stone-forming environment. They have higher urinary pH and calcium and oxalate excretion (when adjusted for creatinine or body weight), augmenting CaOx saturation and stone formation. 4 Thus, the COM and COD stones distribution in children may be distinct from adults.
Stone formation etiology involves factors such as age, gender, diet, and genetics. 2,4 Although the pediatric stone composition distribution and underlying metabolic abnormalities have been described, 10 –14 the clinical and metabolic correlates of COM and COD specifically could only be inferred from studies that included heterogeneous age groups without an emphasis on children. 6,7 The findings suggested an equal or higher distribution of COD than COM in younger patients, and a predominance of COM in older patients. The only few studies that specifically evaluated the pediatric COM and COD stones distribution were conducted in developing countries in the Maghreb region and lacked metabolic correlates. 15,16
Israel's population comprises various ethnic groups, mainly Jewish and Arab. Race and ethnicity were also found to affect the stone prevalence and distribution. Nephrolithiasis was more common in non-Hispanic whites, 4 and in China, CaOx stone distribution differed between the Muslim Uyghur minority and Han male children. 17 Earlier pediatric studies in Israel also suggested ethnic differences in stone distribution, but they were carried out in small cohorts using obsolete chemical-based stone analyses. 18
This study sought to investigate the pediatric CaOx stones composition and distribution and the associated clinical and underlining metabolic abnormalities in Israeli PSFs by age, gender, and ethnicity. We further examined the general stone distribution and their clinical and metabolic correlates.
Materials and Methods
The records of all first-time PSFs aged 1 to 18 years who underwent stone analysis at our tertiary medical center in Israel between March 2014 and December 2019 were retrospectively reviewed.
Quantitative analysis of stone composition was performed with the Bruker ALPHA Fourier Transform Infrared (FTIR) spectrometer (Bruker, Karlsruhe, Germany). Measurements were compared with the Bruker BLG 1&2 spectral libraries. The eight most frequent stone components were documented. Organic materials, such as proteins and triglycerides, were grouped into a single class. Stones were categorized by their major component (accounting for ≥90% of the total content in pure stones or the highest relative component in mixed stones) and reported as a percentage of occurrences in the entire cohort and by age, gender, and ethnicity.
To analyze the correlation between stone composition and age, the cohort was divided into three groups: ages 1 to 5 (preschool), 6 to 12 (prepubescence), and 13 to 18 (adolescence), accounting for the different prevalence, clinical presentations, and stone distributions according to age, previously reported. 1,4,17,19 Only each patient's first stone was included in the analysis to avoid overestimating stones more prone to recurrence.
Metabolic evaluations were performed using 24-hour urine collections or, for non-toilet-trained PSFs, at least two spot urine samples. The mineral-to-creatinine ratio was compared with age-appropriate reference values, 20 as recommended by guidelines. 5
For statistical analysis, means and standard deviations or median and interquartile range were used for continuous variables, and proportions for categorical variables. Continuous variables were compared by the Wilcoxon test and t-test, and categorical variables by chi-square and Fisher's exact tests. Two-sided p-values <0.05 were considered significant. Data were generated with SAS, version 9.4 (SAS Institute, Inc., Cary, NC, USA).
The study was approved by the institutional review board (Protocol No. 770-19) and conducted in accordance with the principles of the Declaration of Helsinki. Owing to the retrospective design, a waiver for consent was granted.
Results
Of the 2479 stones submitted to our chemical laboratory during the study period, 254 were derived from children. After eliminating recurrent stones, the final cohort included 220 first-time PSFs.
The clinical characteristics of the cohort are presented in Table 1. Most children (74%) were symptomatic at diagnosis, with differences by gender and age. Female gender was associated with higher rates of urinary tract infection (UTI) (p < 0.0001) and fever (p = 0.046). Patients aged 1 to 12 years had higher than older children urinary retention rate, diagnosed clinically by a “globus” identification on physical examination or a bladder scan (p = 0.027), whereas colic pain was more prevalent at ages 13 to 18 (p = 0.04). UTI was significantly more prevalent in the 1- to 5-year group than in the rest of the cohort (p = 0.017).
Clinical Characteristics and Presenting Features
Non-Jewish and non-Arab ethnic origin.
For example: ureteropelvic stenosis, ureterovesical stenosis, horseshoe kidney, ectopic ureter, and ureteral stricture.
BMI = body mass index; IQR = interquartile range; SD = standard deviation; UTI = urinary tract infection.
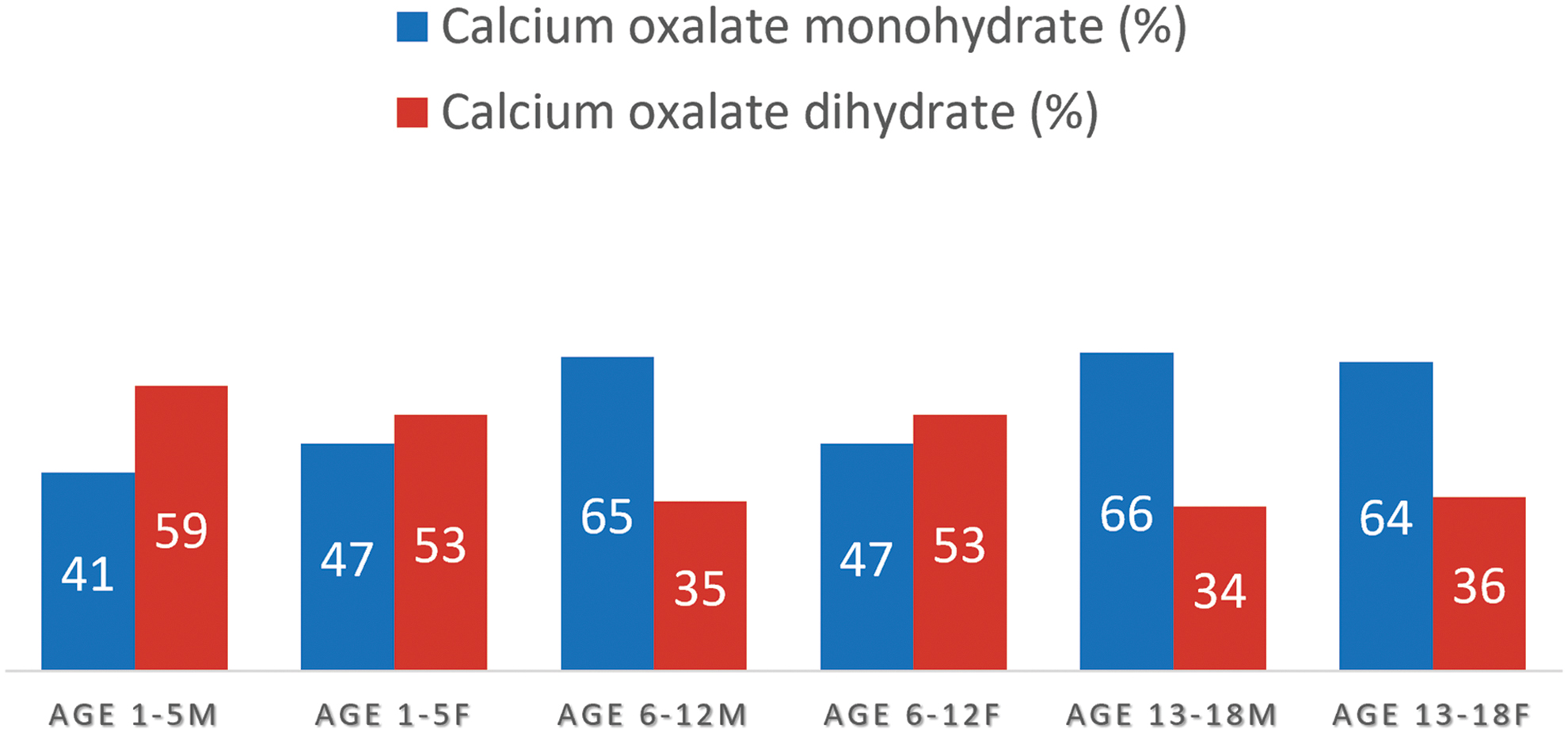
The distribution of the major stone components and metabolic abnormalities are presented in Table 2. COM was the most prevalent stone composition (40% of total stones), with differences in prevalence relative to COD by age. COM was significantly more prevalent in the two older groups (6–12 and 13–18 years) compared with the youngest group (p = 0.023), in which COD stones were more prevalent (Fig. 1). In the intermediate-age group (6–12 years), the distribution of COM and COD differed by gender and ethnicity. COD stones predominated in both Jewish and Arab females. However, in Jewish males, the distribution of COD and COM stones was equal, whereas in Arab males, the relative proportion of COM stones was higher, affecting the general proportion of COM stones in this group. In the 13- to 18-year-old patients, COM was the predominant stone component regardless of gender or ethnicity (Figs. 2 and 3).

Relative ratio of COM and COD stones by age groups. COD = calcium oxalate dihydrate; COM = calcium oxalate monohydrate. Color images are available online.
Relative ratio of COM and COD stones by age and gender. Color images are available online.
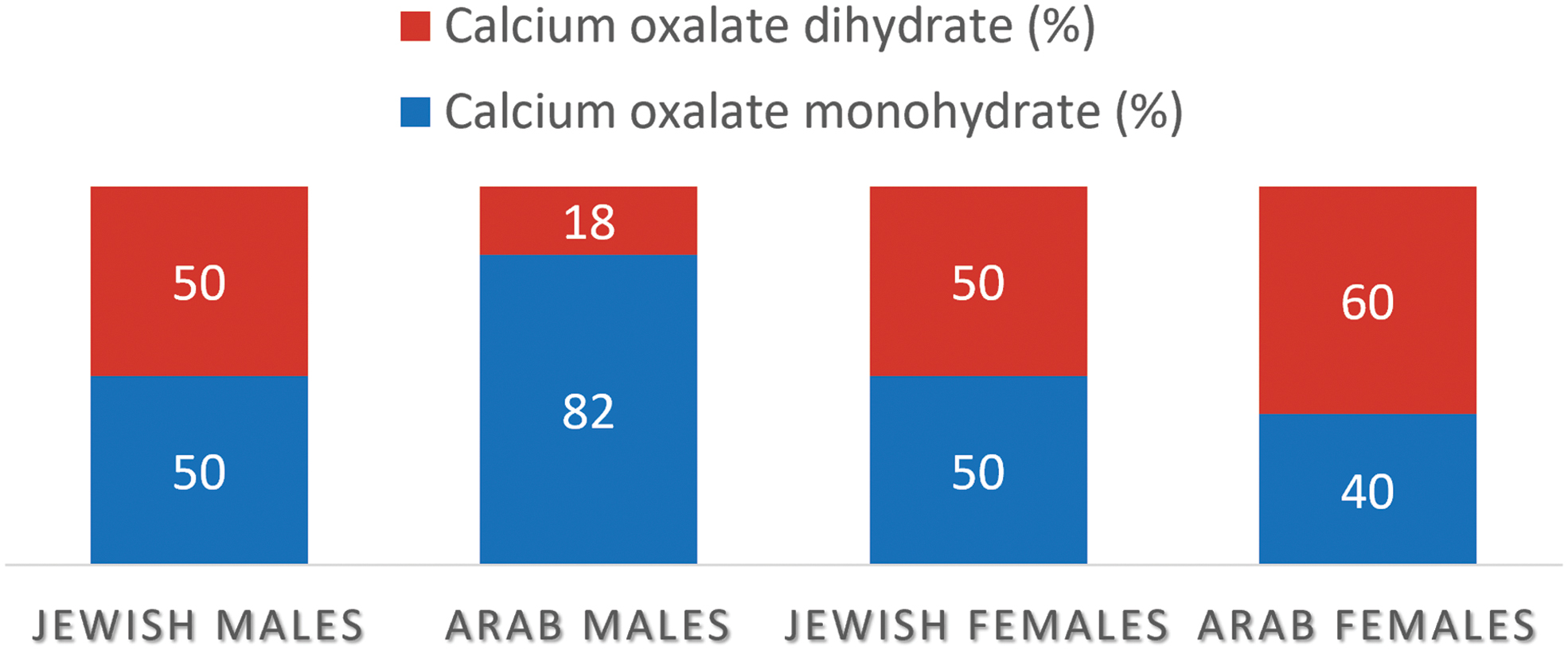
Relative ratio of COM and COD stones in the 6- to 12-year age group: ethnic correlates. Color images are available online.
The Major Stone Components and Rates of Metabolic Abnormalities
The proportion relative to all CaOx stones.
The percentage sum is >100% because some patients had more than one metabolic abnormality.
Normal reference urinary values in 24 hours urine collection: 20 calcium: <0.1 mmol/kg/24 h (<4 mg/kg/24 h); citrate: male >1.9 mmol/1.73 m2/24 h; female >1.6 mmol/1.73 m2/24 h (male >365 mg/1.73 m2/24 h; female >310 mg/1.73 m2/24 h); oxalate: <0.5 mmol/1.73 m2/24 h (<045 mg/1.73 m2/24 h); uric acid: <4.85 mmol/1.73 m2/24 h (<815 mg/1.73 m2/24 h); cystine: <250 mmol/1.73 m2/24 h (<60 mg/1.73 m2/24 h).
CaOx = calcium oxalate; COD = calcium oxalate dihydrate; COM = calcium oxalate monohydrate.
Metabolic results were available for 94 children (43%), among whom 63 had COM or COD stones (67%). Hypercalciuria was significantly more prevalent in patients with COD than COM stones (63% vs 10%, respectively; p < 0.0001), and hyperoxaluria was more prevalent in patients with COM stones (39% vs 6%, respectively; p = 0.002) (Table 3). On analysis by age, the rate of hyperoxaluria decreased from 21% to 6% between ages 1 to 5 and 13 to 18 years (p = 0.08), whereas the rate of hypocitraturia increased from 15% to 44%, respectively (p = 0.02). Overall, metabolic abnormalities were more prevalent in males (p = 0.027) and Arab children (90% vs 68%, p < 0.05).
Metabolic Abnormality Rates by the Major Calcium Oxalate Stone Component
Bold values are statistical significance.
Values are n (%) unless otherwise indicated.
On multivariate analysis, age was the only independent predictor of COM/COD stone distribution. COD stones were associated with younger ages (1–5 years) and COM, with intermediate and older ages (6–18 years) (odds ratio [OR] 0.39, 95% confidence interval [CI] 0.18–0.86, p = 0.036).
Infection stones (struvite or carbon apatite) were identified in 28 children (13%). They were more prevalent at ages 1 to 5 than at 6 to 18 (p = 0.009). Struvite stones were more common in females (p = 0.03). The most commonly associated uropathogens were Escherichia coli (n = 16, 57%) and Proteus (n = 10, 36%).
Discussion
This study sought to evaluate the distribution of CaOx stones subtypes and their association with metabolic parameters in a cohort of 220 PSFs. Most had symptoms at presentation. The main symptom was age-dependent, with renal colic presenting in older children, as previously reported, 12,19 and urinary retention in younger children. Earlier studies might explain the latter. They suggested that acute genitourinary pain in young children can trigger a unique increase in sympathetic nerve activation, with reduced pelvic floor relaxation and acute urinary retention. 21
The clinical relevance of differences in the mineral composition of CaOx stone subtypes is often underestimated. In adults, Bamberger et al. 9 identified distinct characteristics associated with each subtype: younger age and higher hypercalciuria rates with COD, hyperoxaluria and hypocitraturia with COM, similar to our pediatric cohort results.
The relative distribution of COD and COM in our cohort is in line with reports from industrialized countries, 1,6,11,13,14 whereas COM was the predominant stone in developing countries. 15,16 Our previous study in Israel 7 showed that COM stones were predominant in patients aged >20 years, and the two subtypes were equally distributed in younger patients. In France, Daudon et al. 6 similarly found COD to be the predominant component in the first two decades in both genders and COM in older patients. To the best of our knowledge, this is the first study to show that the youngest age groups (1–5 and 6–12 years) are mainly responsible for the generally higher COD ratio in patients aged <20 years. Age 1 to 5 years was a significant independent predictor for COD stones formation (OR 0.39, 95% CI 0.18–0.86, p = 0.036), whereas adolescents had the same distribution as adults.
Regarding gender and ethnicity, COD was the predominant component in all patients aged 1 to 5 years. However, in patients aged 6 to 12 years, Arab males had a higher prevalence of COM stones, whereas Arab girls and Jewish patients did not. At ages 13 to 18, COM was the predominant component in both genders and ethnicities, similar to adults. 6 –8 Girls, particularly Arab girls, had a higher prevalence of COD stones, in accordance with findings from Tunisia 16 and France. 6
Although Arabs constitute ∼20% of the Israeli population, they accounted for ∼35% of the CaOx stone formers. Furthermore, studies from Tunisia 16 and Morroco, 15 both nonindustrialized countries with Arab ethnic ancestry, reported that COM was the major stone component in all age groups, similar to our results in intermediate-age (6–12 years) Arab children. These findings may suggest that a specific predisposition genetic or dietary component unique to children of Arab ethnicity, particularly males, may promote the formation of COM over COD.
Gender and ethnic variability were also characteristic of the relative frequency of underlying metabolic abnormalities. Males (p = 0.027) and Arabs (p = 0.05) had higher rates of metabolic abnormalities than females and Jews, respectively. Indeed, a genetic predisposition for hyperoxaluria was previously reported in Israeli Arabs. 22 Although the relatively higher rates of consanguineous marriages and inherited diseases in certain Arab villages and rural areas 23 could account for some of these differences, no association between positive family history and gender, ethnicity, stone composition, or metabolic abnormalities was found in our study. This may further suggest that shared familial environmental factors, such as dietary habits, are the predominant factor predisposing to familial stone formation.
Most of our CaOx stone formers (68%) had metabolic abnormalities, as previously reported. 2,4 Similar to findings in adults, 8,9 we observed a correlation of COM and COD with hyperoxaluria and hypercalciuria, respectively. At ages 1 to 5, hypercalciuria and hyperoxaluria were the most prevalent metabolic abnormalities, as opposed to hypocitraturia and hypercalciuria, which were the most prevalent at ages 13 to 18. Additionally, the mean urinary pH (6.6 ± 0.8) was higher than the mean pH (∼6) previously associated with COD in adults, in accordance with other pediatric studies. 8
Furthermore, the hyperoxaluria rate decreased between ages 1 to 5 and 13 to 18 years (21%–6%, p = 0.08), whereas the rate of hypocitraturia increased (15%–44%, p = 0.02). Urinary citrate levels have been shown to be highest in early childhood and to decrease thereafter. 4,13,24,25 Turudic et al. 24 found that although oxalate excretion in PSFs tended to decline with age, there was a significant increase in oxalate relative to the CaOx crystallization inhibitors citrate and glycosaminoglycans due to their declining excretion. 24 Hypocitraturia has been implicated with higher COM formation in adults. 9 These may explain the rising rates of COM stones and hypocitraturia in the absence of rising hyperoxaluria rates with age, observed in the present study. However, we also found that combined hypercalciuria and hypocitraturia were primarily associated with COD, not COM, suggesting that urinary calcium excretion may be a more significant determinant of pediatric CaOx stone formation.
Our findings may promote a more practical clinical approach to metabolic evaluations, treatment decision-making, and preventive measures in PSFs. Metabolic evaluations are cumbersome, expensive, and time-consuming. Chan et al. 26 suggested that in first-time PSFs, a limited evaluation consisting of 24-hour urinary volume, calcium, oxalate, and citrate was sufficient to detect almost all clinically significant metabolic abnormalities when the stone composition was available without the need to change the prescribed therapeutic regimen for missed abnormalities. This strategy also reduced costs by nearly 60%. 26 Given the results of the present study, a less extensive evaluation might be adopted to identify suspected hypercalciuria and hyperoxaluria or hypocitraturia in children with COD and COM stones, respectively.
Moreover, in cases of COD stones and borderline metabolic abnormalities, clinicians might consider a lower threshold for initiating thiazide diuretics when deciding on the feasibility of medical treatment beyond the general dietary recommendations.
Our findings may also impact the surgical treatment choice. Extracorporeal shockwave lithotripsy (SWL) is recommended as first-line treatment for pediatric renal stones measuring <20 mm. 5,27 It has been found to yield better results in children than adults. Although a shorter skin-to-stone distance and easier ureteral stone fragments passage might explain the difference from adults, the stone composition is a more critical factor in predicting SWL success rates. 5 COD is more fragile than COM due to its more heterogeneous exterior morphology and less dense internal architecture, which make it more responsive to lithotripsy. 9 This factor warrants consideration when weighing treatment choices, particularly for the youngest (age 1–5 years) children.
Alfandary et al. 28 reported an association between elevated body mass index (BMI) and stone formation rates in Israeli Jewish adolescents in their population-based study. This finding, which only identified two worldwide trends of increasing pediatric obesity 29 and stone prevalence, 1 without established causality, was not supported by the present study that also included younger and Arab children. The overall 22% obesity rate in our cohort was lower than the ≥35% reported in Israeli children, 29 similar to previous pediatric studies. 1,4,12 The higher mean urinary pH in PSFs may encourage less BMI-dependent stone formation, as opposed to the inverse relationship between BMI, stone formation, and urinary pH in adults. 1,4
This study was limited by the retrospective design and missing data in some patients (BMI, symptoms, family history, imaging, genetic and metabolic urinary, and serum evaluations) due to nonuniform documentation in the medical files. However, the patient characteristics rates concorded with other studies in nonendemic and developed countries. 1,2,4,12,19 Furthermore, considering most of our metabolic evaluations were ordered by either nephrologists or urologists, our metabolic evaluation rates, overall (43%) and in the 1- to 5-year group (52%), were similar to other studies in developed countries, such as those of Chan et al., 26 which only one-third of their patients submitted adequate 24-hour urine specimens, and Ellison et al. 30 (12%; four- to sevenfold higher when ordered by a urologist or nephrologist and in younger children). Nevertheless, we recognize the possible bias inherent in using spot urine mineral-to-creatinine ratio adjusted to age and weight.
Finally, our chemical laboratory serves as the stone analysis center for the largest health management organization in Israel, providing health care to more than half of the population. Thus, we believe that our data are representative of the local population.
Conclusions
This study showed that CaOx stone subtypes in first-time PSFs vary by age, gender, and ethnicity. COD was more prevalent in younger ages and females. As in adults, it was associated with hypercalciuria, and COM with hyperoxaluria. Hypercalciuria and hypocitraturia were the predominant metabolic abnormalities in younger and older children, respectively. Our findings suggest that the complex metabolic interactions that drive stone formation differ between children and adults. Thus, a more limited less expensive approach to metabolic evaluation may be feasible to guide the treatment choice and preventive measures in PSFs.
Footnotes
Authors' Contributions
P.L.: Conceptualization, methodology, data curation, validation, formal analysis, investigation, visualization, writing—original draft, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work. H.H.: Data curation, investigation, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work. R.B.: Data curation, investigation, formal analysis, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work. R.T.: Data curation, resources, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work. D.B.-M. and R.M.: Data curation, visualization, supervision, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work. D.L.: Conceptualization, methodology, data curation, supervision, visualization, writing—original draft, writing—review and editing, approved the final version and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.