
Abstract
Introduction and Objective:
Prior literature had demonstrated increased stone burden and higher rates of staged surgery in individuals of lower socioeconomic status (SES). Low SES individuals are more likely to experience delays in definitive stone surgery after initial presentation to the emergency department (ED) for kidney stones. This study aims to investigate the relationship between delays in definitive kidney stone surgery and the subsequent need for percutaneous nephrolithotomy (PNL) and/or staged surgical procedures using a statewide data set.
Methods:
This retrospective cohort study gathered longitudinal data from 2009 to 2018 using the California Department of Health Care Access and Information data set. Patient demographic characteristics, comorbidities, diagnosis/procedure codes, and distance were analyzed. Complex stone surgery was defined as initial PNL and/or undergoing more than one procedure within 365 days of initial intervention.
Results:
A total of 1,816,093 billing encounters from 947,798 patients were screened, resulting in 44,835 patients with ED visits for kidney stones followed by a urologic stone procedure. Multivariable analysis revealed that relative to patients who underwent surgery within 1 month of initial ED visit for stone disease, patients were at increased odds of undergoing complex surgery if waiting ≥6 months (odds ratio [OR] 1.18, p = 0.022), ≥1 year (OR 1.29, p < 0.001), and ≥3 years (OR 1.43, p < 0.001).
Conclusions:
Delays in definitive stone surgery after initial ED encounter for stone disease were associated with increased likelihood of undergoing a complex stone treatment.
Introduction
An estimated 11
Although the exact pathophysiology of kidney stone formation is still unknown, it is understood that stones grow larger over time. 5 Larger stones require more invasive surgical approaches and have higher likelihood of needing staged procedures for stone clearance. 6 Brubaker and colleagues found that underinsured patients and those of Black or Hispanic race and ethnicity experienced delays in time to definitive stone surgery relative to patients with private insurance and patients who are White. 7 These findings implicate delays in definitive treatment as a potential component influencing the relationship between social factors associated with low SES and increased frequency of staged and/or invasive procedures for stone disease.
The objective of this study was to investigate the relationship between delays in definitive surgery for kidney stones and the subsequent need for complex surgical procedures using a statewide data set. The hypothesis is that the likelihood of complex surgical treatment (as defined by percutaneous nephrolithotomy [PNL] surgery and/or staged surgery) for stone disease increases with increasing time from initial emergency department (ED) presentation for kidney stones to subsequent definitive intervention.
Methods
Data source
Longitudinal data from 2009 to 2019 were gathered using the Department of Health Care Access and Information (HCAI), formerly the Office of Statewide Health Planning and Development (California). The data sets included billing data from ambulatory surgical encounters, ED visits, and inpatient encounters. This study was approved by the California Protection of Human Subjects Committee (Project No. 2020-232) and local institutional review board at the University of California (San Francisco). Standardized data elements available for use across all queried data sets included patient characteristics, diagnosis codes, procedure codes, and other key location-specific parameters of the patient and the health care facility.
Inclusion criteria
All adult patients (18 years or older) with an ED visit with a principal diagnosis of urolithiasis (see Appendix A1 for diagnosis codes) were included in the study population. Patients with a documented surgical intervention or intervention within 7 days of ED visit were excluded as a window to exclude emergency procedures. Any patients with a documented history of urothelial carcinoma, cystinuria, or hyperoxaluria (Appendix A1) were excluded to prevent the inclusion of cancer-related urologic procedures and genetic causes of kidney stones.
Outcome
The outcome of this study was receipt of complex stone surgery following an ED visit. Complex stone surgery was defined as initial PNL (see Appendix A1 for procedure codes) and/or undergoing more than one procedure within 365 days of initial intervention (excluding emergent procedures within 7 days). Patients undergoing only stent placement or nephrostomy tube placement as isolated initial procedures were not considered to have undergone a definitive stone procedure. Initial definitive stone procedure was defined as initial PNL, ureteroscopy (URS), and/or extracorporeal shockwave lithotripsy (SWL). All subsequent stone interventions (PNL, URS, SWL, stenting, and/or nephrostomy tube placement) were counted as staged procedures downstream of the initial definitive intervention.
Predictors
The primary predictor of interest was time from ED visit to initial surgical intervention. Other important covariates included age, gender, race and ethnicity, insurance at the time of ED visit, distance to intervening hospitals, and Charlson Comorbidity Index (CCI). Payer information available at the time of ED visit was categorized as: private insurance, Medicaid (Medi-Cal), Medicare, self-insured, and other. Race and ethnicity were used as a single covariate by stratifying White/Caucasian and Black/African American races by ethnicity to generate four categories: White Non-Hispanic, White Hispanic, Black Non-Hispanic, and Black Hispanic. Distance to intervening hospitals was derived using patient zip code and hospital zip code at all surgical encounters. CCI was calculated based on diagnosis codes at the time of ED visit (Appendix A1).
Prior decompression was identified as any ureteral stent or nephrostomy tube placement (Appendix A1) between ED presentation and definitive surgery. Social deprivation index (SDI) was used to account for social factors including factors associated with demographics of the patient zip code with a higher score corresponding to higher levels of area disadvantage. 8 Time categories were selected based on practical monthly/yearly calendar divisions while taking into account patient quartile distribution: 1 month (approximate first quartile), 3 months (approximate second quartile), 6 months (third quartile), 12 months (approximate third quartile), 3 years (fourth quartile), and 5 years (fourth quartile) for risk stratification.
Statistical analysis
The statistical analysis focused on the assessment of the magnitude of the association of time from the ED visit to initial surgical intervention with stone surgery complexity. Initial analyses included comparison of predictor variables between subjects with complex stone surgery and those with noncomplex stones. Chi-square tests were used to compare categorical variables between the surgery group, and Student's t-tests were used to compare continuous variables.
The association between time from ED visit to initial surgical intervention and stone surgery complexity was analyzed using a multivariate logistic regression model. The model included time as the primary predictor variable in addition to the following covariates: insurance, race and ethnicity, distance to the hospital, age and CCI, prior decompression, and SDI based on their known clinical significance. Gender was not included in the multivariate model given that it was found to be nonsignificant on univariate analysis. Marginal predicted probabilities using fitted logistic models were plotted against time to ED visit to understand the magnitude of association between time and stone surgery complexity. The magnitude of association between insurance, distance, and CCI controlling for time was also visualized by plotting marginal predicted probabilities vs time across covariate groups.
Results
A total of 1,816,093 billing encounters from 947,798 patients were screened, resulting in 44,835 patients with ED visits followed by a urologic stone procedure (Fig. 1). Univariate analyses illustrated that 14.8% (6624 patients) of the 44,835 patients included in the study population underwent complex stone surgery after ED diagnosis of urolithiasis. Significant differences in the receipt of complex stone surgery existed across all covariates except gender (Table 1). Similarly, significant differences in time to initial surgery existed across all covariates including gender (Supplementary Table S1). All patients experienced a mean interval of 269.8 (standard deviation [SD] = 430.3) days from their ED visit to their initial surgery (Q1: 22.0, median: 55.0, Q3: 293.0).
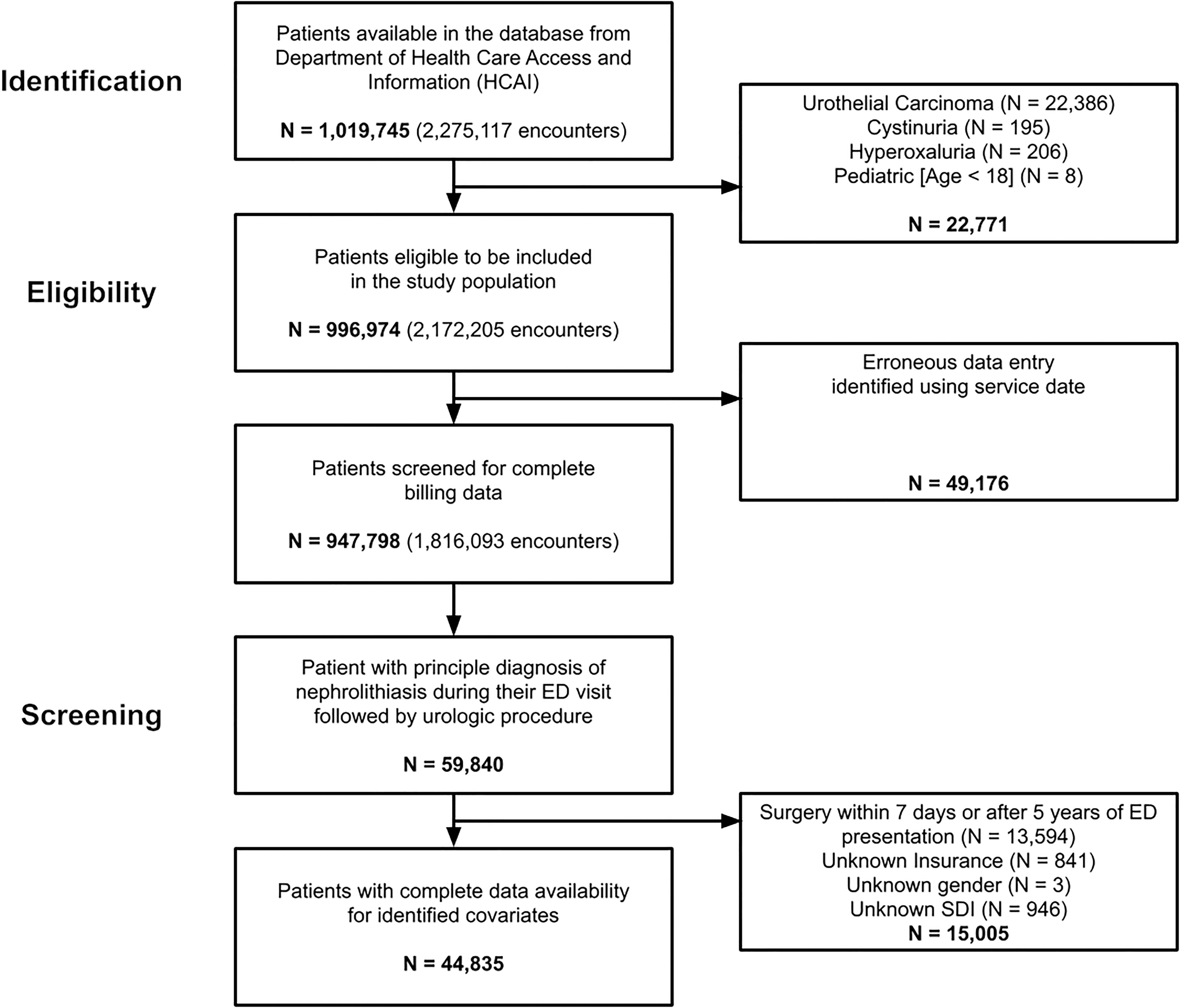
Patient selection workflow. A total of 1,019,745patients were identified as potential stone formers using the Health Care Access and Information data set. After applying the inclusion and exclusion criteria and considering potentially erroneous data collection, 44,835 patients were included in the study population.
Sample Size and Patient Characteristics
Bold values signify p values less than 0.05.
Univariate analysis of 6743 (14.8%) and 38,805 (85.2%) patients receiving complex stone surgery and noncomplex stone surgery, respectively, revealed significant differences based on age, race and ethnicity, insurance status, the time of ED visit, distance between residence and surgical location, and Charlson Comorbidity Index. Gender was found to be nonsignificant.
ED = emergency department; SDI = social deprivation index.
Six thousand six hundred seventy-four (14.9%) patients were outside of the interquartile range (1.5 × IQR) for time in days between ED visit and definitive surgery date, suggesting a skewing of our data set toward individuals identified as waiting >699 days from their ED presentation to their definitive surgery. After their initial stone intervention, patients in the complex stone surgery group underwent a mean of 1.22 (SD = 0.88) procedures after their initial intervention with an average time difference of 83.59 (SD = 87.91) days (Supplementary Figs. S1 and S2).
Odds of undergoing complex stone surgery following ED visit was significantly higher after intervals >6 months between ED visit and definitive intervention. Odds of complex stone surgery with a delay of 6 to 12 months, 1 to 3 years, and 3 to 5 years were 1.18, 1.29, and 1.43 higher, respectively (p < 0.01). Insurance status at the time of ED visit was also predictive of complex stone surgery with Medicaid (odds ratio [OR] 1.52, 95% confidence interval [CI] 1.41–1.64) and Medicare (OR 1.25, 95% CI 1.14–1.38) showing significantly higher odds relative to private insurance (p < 0.001).
Living more than 10 miles from the hospital was associated with a 12% increase in odds (p < 0.001). Each one-point increase in CCI was associated with a 10% average increase in odds of undergoing complex surgery (p < 0.001). Prior decompression was associated with 12% increased odds of complex surgery (p = 0.019). Higher SDI was also associated with increased odds at 1.25 and 1.26, respectively, for SDI of 51 to 75 and 76 to 100 (p < 0.001). There was no significant difference in odds of undergoing complex surgery by race and ethnicity or age (Table 2).
Odds Ratios for Undergoing Complex Stone Procedure
Bold values signify p values less than 0.05.
Multivariate logistic model with time and all significant univariate covariate as predictors revealed increasing odds of complex stone surgery with increasing time delay, significant differences among insurance groups, distance from residence and surgical location, and Charlson Comorbidity Index.
CI = confidence interval; OR = odds ratio.
Predicted probabilities of receipt of complex stone surgery, based on multivariate logistic regression, showed increasing trends with greater delay between ED visit and first definitive surgical intervention (Fig. 2). Using time as a continuous variable revealed 0.03% increase in odds of undergoing complex surgery for every 1 day delay in surgery (OR 1.00028, 95% CI 1.00023–1.00034, p < 0.001) (Fig. 3 and Supplementary Fig. S3A). Predicted probabilities were also observed to be increased for Medicare and Medicare in reference to the private insurance group (Supplementary Fig. S3B). Distance illustrated increased predicted probabilities for patients living more than 10 miles from the hospital; however, a significant overlap in the 95% CI was observed across time (Supplementary Fig. S3C). Increasing probabilities were observed across time for each stratum (0–3) of CCI (Supplementary Fig. S3D).
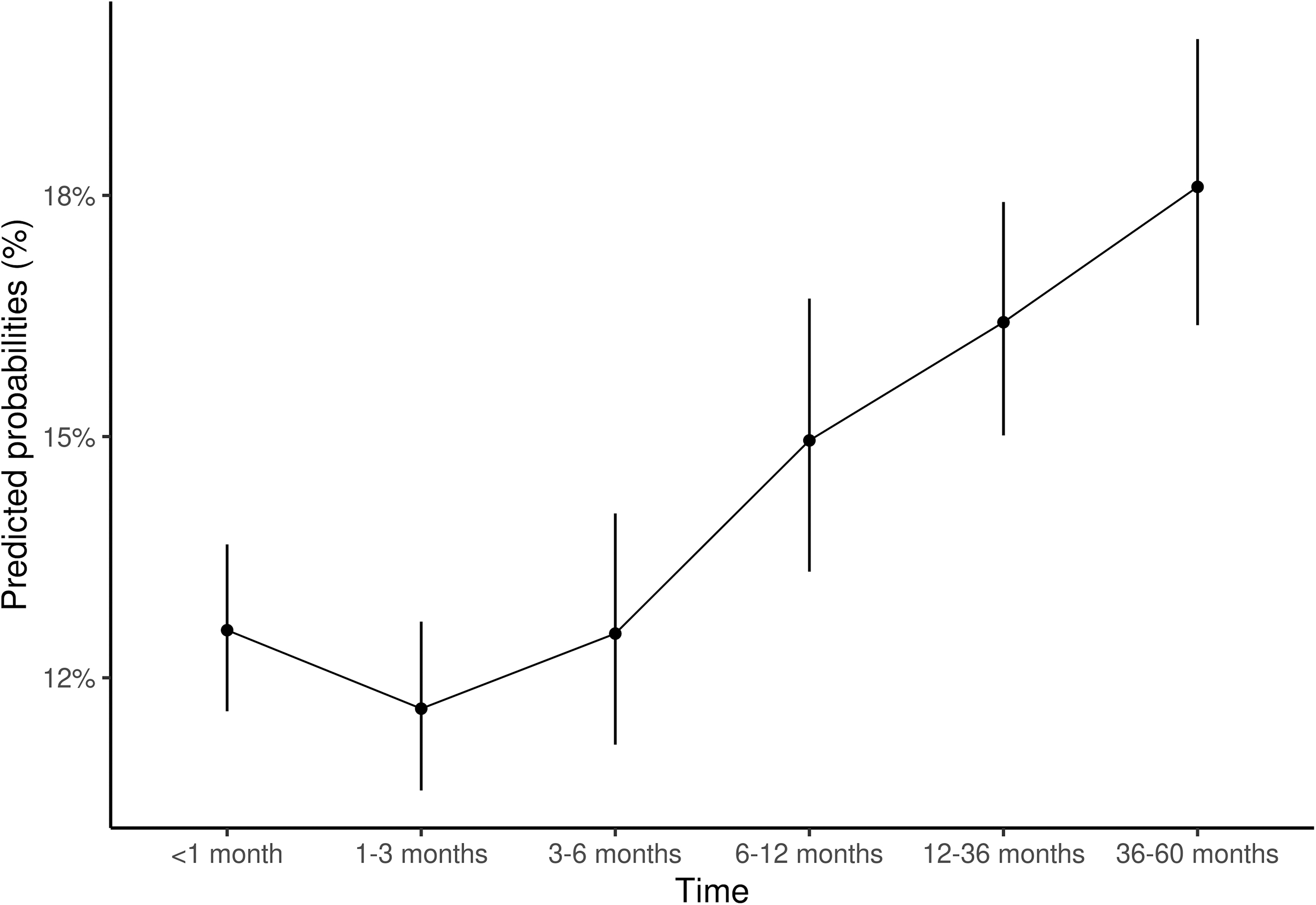
Complex stone surgery by time categories. Multivariate logistic model using clinically significant time categories as a predictor showed increasing probability of complex stone surgery as time increased, especially past the 3 to 6-month period.
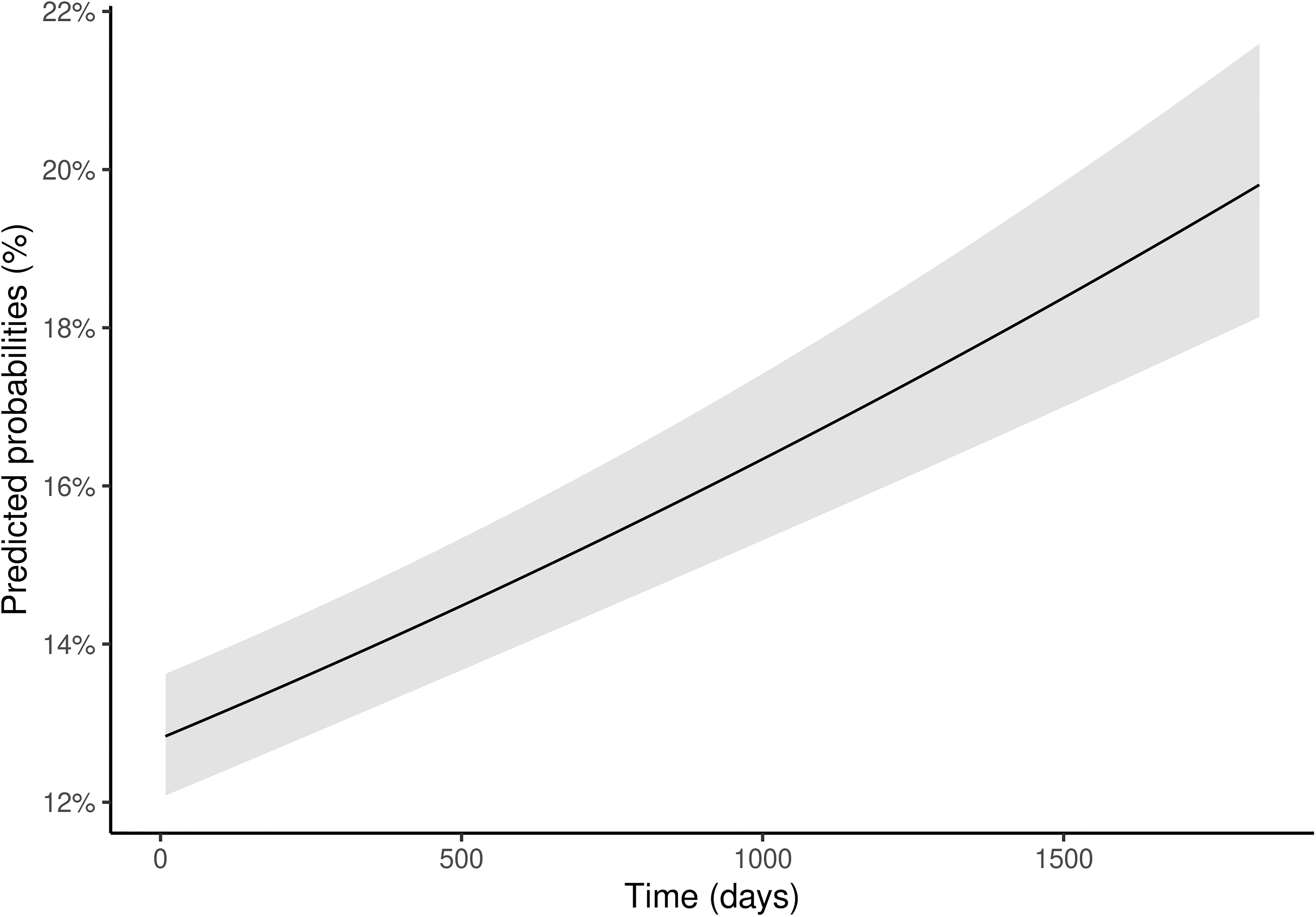
Complex stone surgery by time in days. Multivariate logistic model using time as a continuous predictor showed increasing probability of complex stone surgery as time increased.
Discussion
This study found that individuals who had surgical delay from their ED presentation to their initial surgical intervention had cumulatively increasing odds of undergoing complex stone procedure. More specifically, each 1 day increase in delay between ED visit and definitive surgical intervention showed a 0.03% increase in odds of complex surgery (p < 0.001). Relative to patients who underwent surgery within 1 month, there was a significantly increased odds of undergoing complex surgery for patients waiting ≥6 months (OR 1.18, p = 0.022), and a consistently increasing odds for patients waiting ≥1 year (OR 1.29, p < 0.001) and ≥3 years (OR 1.43, p < 0.001). This study also found higher odds of complex stone surgery among patients with Medi-Cal (OR 1.52), Medicare (OR 1.25), or self-pay (OR 1.23) relative to patients with private insurance (p < 0.001).
Comorbidities captured via CCI were associated with a modest increase in one's odds of complex stone surgery (OR 1.10, p < 0.001), as was living a distance >10 miles from the center where surgery was performed (OR 1.12, p < 0.001). Complexity of the stone presentation measured using receipt of prior decompression procedure with stent placement of nephrostomy tube placement showed increased odds of eventual complex definitive treatment (OR 1.12, p < 0.019). These findings are not consistent with prior research demonstrating improved stone-free rates with a stent placed before URS for obstructing stones; however, our analysis also takes into account temporizing nephrostomy tube placement as well. 9 Social factors summarized using SDI had increasing odds with SDI >50 with odds of up to 1.26 (p < 0.001). Here, PNL is considered a “complex stone procedure” because it is a more invasive surgical treatment compared with SWL and URS, resulting in higher incidence of complications such as bleeding, infection, and renal failure. 10 –12
Increasing the odds of having to undergo initial PNL and/or multiple PNL, URS, or SWL procedures may be due to delaying surgical intervention places patients at an increased risk of developing surgical complications. These findings are consistent with prior research demonstrating that earlier SWL intervention is associated with reduced odds of requiring additional SWL procedures. 13 –15 Patients facing delays in care due to COVID-19 have been noted to have higher rates of leukocytosis, elevated creatinine, hydronephrosis, and need for emergency procedures. 16,17 Patients who experience longer wait times to surgery are more likely to have repeated emergency room visits, repeated CT imaging, and upper urinary tract decompression before definitive treatment. 7 However, these prior studies have followed patients over time intervals of a few days to a few months. This study is unique in that it follows patients over much longer time intervals of care delays before definitive surgical intervention (up to 5 years), demonstrating increasing odds for PNL and/or multiple stone surgeries as this interval increases.
Relative to patients with private insurance, patients with Medi-Cal, Medicare, or self-pay were found to have significantly increased odds of undergoing a complex kidney stone surgery (p < 0.001). Even after adjusting for other SES-related factors such as race, gender, income, and education level, private insurance has been associated with lower odds of developing stones compared with having state-assisted insurance. 18,19 Underinsured patients (patients with Medicaid and Medicare) with urolithiasis also have greater odds of a staged surgery for stone clearance. 20 This study also demonstrated that comorbidities captured via the CCI are associated with a modest increase in one's odds of complex stone surgery (OR 1.09, p < 0.001).
This is consistent with the known association between hypertension, obesity, and diabetes mellitus and kidney stone disease, and is consistent with previous work showing higher odds of undergoing staged surgery for stone disease with increasing CCI. 20 –22 Interestingly, when adjusting for time, there was no statistically significant association between odds of complex stone procedure and racial/ethnic categorization. This is contrary to prior literature demonstrating Black patients, regardless of insurance status, experience delays in scheduling kidney stone surgery and have increased odds of staged surgery for stone disease. 20,23 This suggests that reducing time to surgical intervention is a feasible target for reducing racial and ethnic disparities in staged surgery for stones.
There were several limitations to this study. First, the data set used did not contain any imaging data. It also did not contain clinical data, such as primary care visits or urologic clinical visits, preventing assessment of other explanations for delays in surgery or procedural approach. Second, the assessment for staged surgery in this study does not clearly differentiate between stone persistence and recurrence; however, prior research using this data set has demonstrated that for patients undergoing multiple surgeries for kidney stones, the mean time between the first and second procedure was 60 days (median 35, SD = 74.59). 20 This suggests stone persistence rather than recurrence. Therefore, it is within reason to conclude that multiple surgeries for stones in this patient cohort are most likely due to larger and/or more complex stones.
Third, patient-level residence data were not accessible for analysis. This prohibited our ability to account for residence type (e.g., skilled nursing facility, rehabilitation facility), which could, in and of itself, pose significant barriers to seeking timely kidney stone surgery. However, our models do include the SDI as a covariate, which has previously been performed as a proxy variable for area-level deprivation. 4 Fourth, these data are derived from claims data, which may result in inaccuracies in patient information collected and analyzed, thus biasing our conclusions toward the null. Finally, the HCAI database does not include data from private surgery centers in California, preventing assessment of patients who undergo surgery for stones in private centers. Furthermore, it is important to acknowledge that varying patient factors may accelerate stone growth; therefore, it cannot be stated that delays in treatment alone are a response for increased need for complex stone.
The limitations of the available data set present an opportunity ripe for further investigation. Initially, the data recorded only includes touchpoints with the health care system following initial presentation to the ED. Prior experience having kidney stones and their symptoms may increase identification of need and urgency to advocate for more timely care. Although we identify patients when they first appear in the longitudinal data set with an encounter diagnosis for kidney stones, it is not possible to determine if patients in our cohort had experienced kidney stones before this. Furthermore, patients admitted on the weekend (i.e., Saturday and Sunday) have been found to experience delayed acute operative care compared with those presenting on a weekday (i.e., Monday to Friday). 24 Although we attempt to exclude patients who undergo emergency procedures for stones within 7 days of their initial ED visit, this “weekend effect” may nevertheless contribute to variance in patient care delays.
Finally, a more holistic assessment of the detrimental impact of stone burden and worse outcomes for those of lower SES would be beneficial. It has been shown that among patients with kidney stones, lower income, non-White race, and unemployed work status are associated with lower quality of life. 25 Although we include proxies for SES in our SDI metric, we do not have any metrics to account for quality of life, which may influence care seeking behavior, delays in treatment, and subsequent need for complex surgery. Future studies investigating the socioeconomic and quality of life consequences following care delays and subsequent complex surgery are warranted, particularly among individuals of lower SES.
It is clear that there are roadblocks to providing equitable high-quality care to patients in a timely manner. The findings of this study demonstrate that delays in the definitive surgical procedure of kidney stones are associated with an increased likelihood of undergoing a complex stone treatment. Complex surgery was also more likely among nonprivately insured patients, patients living further from the surgery facility, and patients with more comorbidities. This study is novel in that it demonstrates a potential source of disparate outcomes among low SES patients, namely delayed treatment from the time of stone disease.
Conclusions
Our findings add to the growing body of literature demonstrating the impact of suboptimal access to health care and disparate outcomes for kidney stone patients. Additional research is needed to further elucidate the factors and/or characteristics that increase the likelihood of delaying time to the surgical intervention for kidney stones.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: Study conception and design (D.B.), data curation and formal analysis (D.B., S.S., J.N.), investigation and interpretation of results (D.B., J.M., S.S., C.H., J.N., C.S.), draft article preparation (J.M., S.S., C.H.), critical review of the article (D.B., J.N., C.S., T.C., M.S.), funding acquisition (D.B., T.C., M.S.). All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
The authors declare that there are no relevant or material financial interests or conflicts of interests to disclose that relate to the research described in this article.
Funding Information
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH) (Grant No. K12DK111028).
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Abbreviations Used
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.