
Abstract
Purpose:
To explore the safety and effectiveness of the Pure Retroperitoneal Laparoscopic Peritoneum Incision Technique (PREP-IT) in laparoscopic radical nephrectomy (LRN) and inferior vena cave (IVC) tumor thrombectomy for right renal-cell carcinoma (RCC) with level Mayo I to III venous tumor thrombus (VTT).
Patients and Methods:
From May 2015 to September 2020, 92 patients with right RCC and Mayo I to III VTT were retrospectively reviewed, including 57 patients who underwent retroperitoneal LRN and IVC thrombectomy using PREP-IT, and 35 patients who underwent open surgery. PREP-IT refers to dissecting the retroperitoneum and temporarily placing the right kidney into the abdominal cavity to enlarge the retroperitoneal workspace for a safer and faster IVC operation.
Results:
Compared with the open surgery group, the PREP-IT group had a larger tumor diameter, while a larger proportion of Mayo I tumor thrombus and smaller maximum tumor thrombus width. Two patients (3.5%) in the PREP-IT group had a history of abdominal surgery. No conversion to open surgery or standard laparoscopic surgery occurred in PREP-IT group. Laparoscopic surgery with PREP-IT was characterized by shorter operative time, less surgical blood loss, shorter postoperative hospital stay, and lower postoperative complication rate. With a 33-month (ranges: 2–86) follow-up time period, the estimated mean overall survival time was 57.2 ± 5.3 and 58.1 ± 71.5 months in the PREP-IT group and open surgery group, respectively. Log-rank test indicated no significant difference between the two groups in terms of overall survival and cancer-specific survival.
Conclusions:
The PREP-IT is relatively safe and feasible for retroperitoneal LRN with right renal tumor and IVC tumor thrombus, allowing for a large workspace and wide exposure for IVC operations.
Introduction
Renal-cell carcinoma (RCC) is a malignant tumor characterized by a tendency to invade the venous system, accounting for 2% to 3% of all cancers. Inferior vena cava (IVC) tumor thrombus is found in 4% to 10% of locally advanced patients, which is significantly associated with the presence of clinical symptoms and poor prognosis. 1 Venous tumor thrombus (VTT) derived from the right renal tumor is more likely to extend into the IVC and therefore more commonly seen than the left one, as the right renal vein (RV) is shorter compared with the left one. Radical nephrectomy and IVC tumor thrombectomy are the main treatment for RCC with IVC tumor thrombus. Laparoscopic surgery offers a minimally invasive choice, with a similar therapeutic effect to open surgery.
The approach for laparoscopic radical nephrectomy (LRN) and IVC tumor thrombectomy includes the transperitoneal approach and retroperitoneal approach. 2 The former is used more widely in general, as it provides a large workspace, which is especially essential for IVC operation. However, the retroperitoneal approach has its advantages in comparison, such as reduced blood loss because of the easy access to the renal artery (RA) and lumber veins, a short time of operation, less bowel irritation, and prevention of peritoneal implantation. 3,4 Still, the narrow workspace and long learning period limit its wide application. 5
To solve these drawbacks, we purpose the Pure Retroperitoneal Laparoscopic Peritoneum Incision Technique (PREP-IT), aimed to enlarge the workspace in tumor thrombectomy for right RCC with IVC tumor thrombus. In brief, the PREP-IT technique refers to dissecting the retroperitoneum and temporarily placing the right kidney into the abdominal cavity to enlarge the retroperitoneal workspace for a safer and faster IVC operation. Herein, we introduced the detailed procedure of the technique and discussed its safety and efficacy based on the short-term outcomes from our center.
Patients and Methods
Patients
Three hundred thirteen patients with renal masses and VTT were adopted in our center from May 2015 to September 2020, and we retrospectively analyzed the clinical data of patients with right RCC and level I to III IVC tumor thrombus according to the Mayo classification. The exclusion criteria include (1) bilateral tumors and (2) only underwent IVC tumor thrombectomy. In total, we enrolled 57 patients who underwent laparoscopic surgery with PREP-IT and 35 who underwent open surgery. LRN with PREP-IT was performed by four experienced urologic surgeons. The indication of the PREP-IT includes right RCC with Mayo I to III IVC tumor thrombus by enhanced CT or MRI scans preoperatively.
The relative contraindications for this technique include the following: (1) a history of abdominal surgery, especially right upper abdominal surgery including gallbladder removal, pancreatectomy, and duodenectomy; (2) severe scoliosis; (3) large renal mass (generally diameter ≥10 cm); (4) fixed masses based on palpation; and (5) preoperative imaging indicating hepatic vein invasion. All the patients underwent pure retroperitoneal LRN and IVC thrombectomy, using the PREP-IT technique. Before the surgery, the benefits and risks were informed to each patient, and informed consent was signed.
An overall preoperative evaluation covers the demographics, clinical symptoms, physical examinations, laboratory tests, and radioactive examinations. Ultrasound, enhanced CT, and IVC MRI were performed to evaluate the side, size, and nature of the primary tumor, the length, width, and border of the VTT, presence of perirenal fat invasion, adrenal invasion, IVC wall invasion, lymph node metastasis, and distant metastasis (Fig. 1). Besides, the presence of bland thrombus and RV branch tumor thrombus was recorded as these manifestations are associated with long-term outcomes. 6,7 The American Society of Anesthesiologists (ASA) score was used to evaluate the tolerance of patients to anesthesia.

Images of renal tumor thrombus.
Intraoperative parameters including the operative time, blood loss, blood transfusion rate, and IVC blocking time were recorded. Postsurgical outcomes, including intensive care unit transfer rate, days to surgical drain removal, days to oral feeding, days to full ambulation, postoperative hospital stays, and postoperative complications, were documented. The severity of the postoperative complications was assessed with the Clavien–Dindo classification system.
The study was approved by Peking University Third Hospital Medical Science Research Ethics Committee (approval no. IRB00006761-M2022597). Informed consent was waived by our Institutional Review Board for the retrospective nature of the study.
Surgical technique
Patients' position and trocar placement
With the retroperitoneal approach, all the patients were placed in the left lateral position after induction of general anesthesia. A 2-cm longitude skin incision was made anterior to the right psoas major muscle under the 12th lib, and blunt dissection was carried down through the incision. The musculature and lumbodorsal fascia were split to enter the retroperitoneal space. The extraperitoneal fat was detached first by index finger, and then, a balloon dilator was placed for further expansion. Usually, 15 to 18 times of inflation, with 50 to 60 mL gas each time is enough. A 12 mm trocar was placed via the incision, and pneumoperitoneum was established with a maintained pressure at 12 mm Hg.
Institute of Urology, Peking University technique can be applied by placing the laparoscope and expanding the retroperitoneal space bluntly with the laparoscope body. 8 Then, another 12 mm trocar was placed in the right anterior axillary line under the rib, and an 11 mm trocar was placed above the right iliac crest. In addition, a 5 mm trocar was placed in the anterosuperior iliac spine for auxiliary.
Renal mobilization
After entering the retroperitoneum, the dorsal Gerota's fascia was incised and perirenal fat was removed. The right RA in the hilum was dissected and clipped with Hem-o-lok clips, and then cut off (Fig. 2A). We dissected along the kidney's dorsal side to mobilize the tumor-bearing IVC (Fig. 2B), followed by the ventral side (Fig. 2C). It is necessary to preserve the perirenal fat for clamping, since in the PREP-IT procedure, the kidney was taken out from the abdominal cavity via the clamped fat.
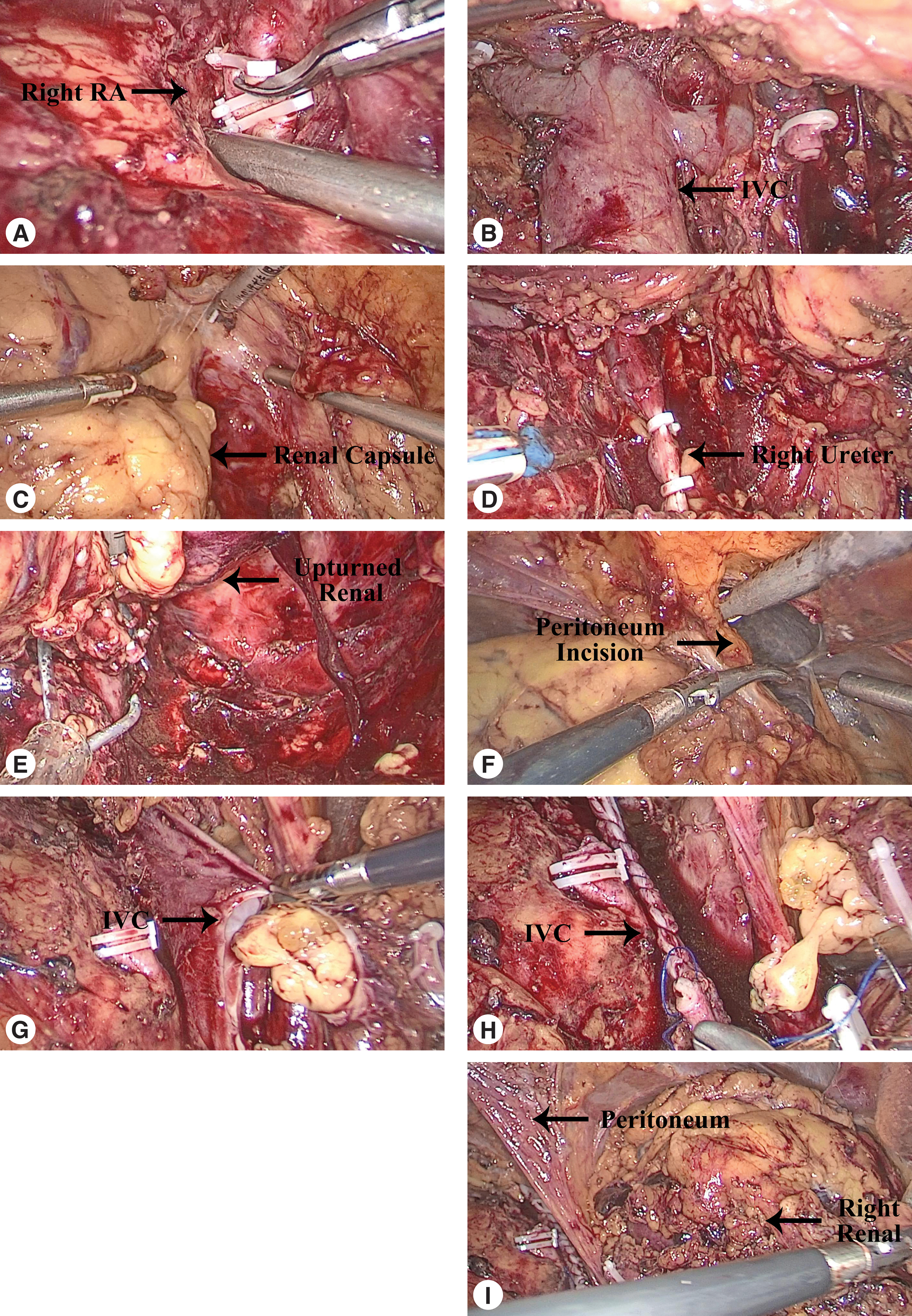
Surgical procedures of LRN for right RCC and IVC tumor thrombus.
Next, a kidney-upturning technique was used in most cases to facilitate the exposure of the medial, inferior, and ventral side of the kidney, taking advantage of the upper pole suspension. First, we mobilized the inferior pole by dissecting the fascia and cutting off the right ureter (Fig. 2D), and then, upturning the kidney by lifting the inferior pole to the upper side with a vascular clamp. This technique allows for exposing the peritoneum and hilum (Fig. 2E). Moreover, the upper pole suspension could provide the kidney with a reliable attachment to the retroperitoneum after it was placed in the abdominal cavity during the PREP-IT procedure, preventing it from dropping down. Then, the distal end of the IVC, left RV, right RV, and the proximal end of IVC were dissected and blocked with vessel tourniquets successively.
PREP-IT and tumor thrombus resection
To develop a larger workspace in the retroperitoneum, PREP-IT was used. A transverse incision was made on the peritoneum in front of the renal capsule, allowing for a renal pass-through (Fig. 2F). We prefer a relatively inferior and lateral incision to avoid bowel or liver damage. Still, this procedure should be performed with caution. Once the incision was performed, the high carbon dioxide pressure was conducted from the retroperitoneum to the abdominal cavity, pushing the bowels aside and thus creating a local hollow space, which was large enough to bear the kidney. Then, we placed the kidney into the abdominal cavity by pushing it with vascular forceps. Hence, the retroperitoneal workspace was expanded. During this procedure, the retroperitoneal space was first oppressed by the filled abdominal cavity, but the workspace would be soon expanded visibly after the kidney was placed in the abdomen.
As with usual tumor thrombectomy, the IVC wall was incised, then the tumor thrombus and invaded vascular wall was resected and collected in a retrieval bag en bloc (Fig. 2G). The IVC was perfused with heparinized saline and sutured continuously with a 4-0 nonabsorbable suture (Fig. 2H). Then the vessel tourniquets of the proximal end of IVC, left RV, and the distal end of IVC were released successively. The kidney in the abdominal cavity was taken out by clamping the perirenal fat and was collected in a retrieval bag following complete dissection (Fig. 2I). The peritoneal incision was closed routinely to prevent the internal hernia, a rare but notable consequence of untreated peritoneal tears as reported. 9,10 A demo video is provided to show the surgery procedures (Supplementary Video S1).
Postoperative care and follow-up
Prophylaxis for deep vein thrombosis included lower limb exercise on the bed, elastic socks, elastic bandage, and early ambulation. Prophylactic anticoagulation was not used routinely because of the bleeding risk. Antibiotics, analgesics, and fluids were given according to the center protocol.
The follow-up period was defined from the date of surgery to the latest documented date of telephone or clinical follow-up, including the survival status, tumor recurrence or metastasis, and postoperative renal function.
Statistical analysis
The Shapiro–Wilk test was used to determine the normality of continuous variables. Categorical variables are given as percentages or frequencies. Continuous variables in accordance with normal distribution are given as mean ± standard derivation, otherwise are given as medians and interquartile ranges. Comparisons between groups were performed using independent t-test (normal distribution) or Mann–Whitney U-test (non-normal distribution) for continuous variables, and chi-square test for categorical variables. Differences in survival were evaluated using the log-rank test. p-Value <0.05 was considered statistically significant.
Results
Table 1 depicts the baseline characteristics of patients. Compared with the open surgery group, patients in the PREP-IT group were characterized by significantly larger tumor diameters (8.0 cm vs 6.6 cm, p = 0.027), a higher proportion of low-level (Mayo I) tumor thrombus (43.9% vs 8.6%, p = 0.002), and smaller maximum width of VTT (17.8 vs 26.3 mm, p < 0.001). Other baseline characteristics, including gender, age, body mass index (BMI), ASA grade, and previous abdominal surgery, showed no significant difference between the two groups.
Baseline Characteristics of Patients Receiving Radical Nephrectomy and Inferior Vena Cave Tumor Thrombectomy Using Pure Retroperitoneal Laparoscopic Peritoneum Incision Technique
Bold font indicates p value ≤0.05.
ASA = American Society of Anesthesiologists; BMI = body mass index; IQR = interquartile range; PREP-IT = Pure Retroperitoneal Laparoscopic Peritoneum Incision Technique; RV = renal vein; SD = standard derivation; VTT = venous tumor thrombus.
The clinicopathologic characteristics are summarized in Table 2. There was no significant difference between the two groups in cN1 stage, cM1 stage, pN1 stage, perirenal fat invasion, ipsilateral adrenal gland invasion, and presence of bland thrombus. However, patients in PREP-IT groups were less comorbid with RV branch tumor thrombus (5.3% vs 33.3%, p = 0.005), including the left adrenal vein, the left gonadal vein, and the left ascending lumbar vein.
Clinicopathologic Characteristics of Patients Receiving Radical Nephrectomy and Inferior Vena Cave Tumor Thrombectomy Using Pure Retroperitoneal Laparoscopic Peritoneum Incision Technique
Bold font indicates p value ≤0.05.
IVC = inferior vena cava.
Compared with the open surgery group, the PREP-IT group was characterized by shorter operative time (290.0 vs 363.3 minutes, p = 0.015), less surgical blood loss (200.0 vs 1330.6 mL, p < 0.001), less transfusion receiving rate (24.6% vs 80.0%, p < 0.001), less intensive care unit transfer rate (40.4% vs 68.6%, p = 0.009), fewer days to surgical drain removal (5 vs 7 days, p < 0.001), days to full ambulation (2 vs 3 days, p = 0.004), days to oral feeding (2 vs 3 days, p < 0.001), and postoperative hospital stays (8 vs 10, p = 0.005). The PREP-IT group received fewer IVC transverse resections (14.0% vs 48.6%, p < 0.001). IVC blocking time showed no difference between the two groups.
The postoperative complication rate was significantly lower in the PREP-IT group (12.3% vs 40.0%, p = 0.002), while the major complication rate indicated no significant difference. Overall, 7 (12.3%) patients in PREP-IT group experienced postoperative complications. Two patients had mild renal dysfunction. One patient had postoperative infection and one experienced atrial fibrillation, both improved after medications. Three patients had IV complications: two had acute renal dysfunction requiring dialysis, and one patient experienced a combination of heart failure, respiratory failure, and acute liver dysfunction after a pulmonary embolism. For patients with severe complications, no death occurred within 9 months after the surgery.
The median follow-up time was 33 (range: 2–86) months. In PREP-IT group and open surgery group, respectively, the mean overall survival time was 57.2 ± 5.3 and 58.1 ± 71.5 months, and the mean cancer-specific survival time was 70.3 ± 4.3 and 65.0 ± 9.7 (Fig. 3). The median overall survival time was 71.0 ± 28.9 months in PREP-IT group. Log-rank test indicated no significant difference between the two groups in terms of overall survival (p = 0.864) and cancer-specific survival (p = 0.971).

Overall survival
Discussion
For radical nephrectomy and IVC tumor thrombectomy, although open surgery is the traditionally preferred approach that can provide wide exposure and safe vascular operation, especially involving Mayo III to IV VTT, its operative wound and surgical blood loss are notable. Recently, there is a gradual transformation toward minimally invasive techniques, including laparoscopic surgery and robot-assisted laparoscopic surgery. 11 –13 Although the latter allows for a more precise and defter operation, and experiences of initial procedures for robotic surgery have been reported even in Mayo III to IV VTT, many institutions still prefer laparoscopes as the major approach for minimally invasive operations. 14 –18
The reasons include the convenience in case of conversion, the flexible choice for the trocar site, and a cheap price compared with robotic surgery. 4 The retroperitoneal laparoscopic approach provides easier access to hilar, shorter operative time, and less bowel irritation compared with the transperitoneal one. Still, the narrow workspace in the retroperitoneum makes the IVC tumor thrombectomy difficult, therefore limiting its use in such surgeries. Making use of the abdominal cavity, PREP-IT is a feasible technique to develop a larger workspace around the IVC for patients with right RCC and Mayo I to III VTT.
As far as we know, no studies have systematically described this technique before. Previous studies had reported the combined retroperitoneal and transperitoneal approach, where the former was applied first for safe vascular control, then the transperitoneal workspace was established to switch the operative route, and the nephrectomy and tumor thrombectomy were finished as with regular transperitoneal laparoscopic procedures. 19 –21 The combined approach and PREP-IT share common advantages, including safe hilar control and a large workspace for tumor thrombectomy, while PREP-IT allows for a pure retroperitoneal approach, which is more convenient with fewer surface wounds and bowel irritations. In addition, when compared with the pure retroperitoneal approach, which usually needs an auxiliary arm to hold up the kidney for wider exposure, PREP-IT helps spare this arm for other assistant procedures.
However, this technique also has its limitations compared with the trans-/retroperitoneal approach or the combined technique. First, PREP-IT is not recommended for left RCC, not only because LRN for left RCC with IVC tumor thrombus is more challenging technically, but also because the IVC is not on the side with the expanded workspace. 22 In addition, for large renal masses (generally ≥10 cm), the risk of secondary peritoneum tears increases significantly during PREP-IT. Besides, it is difficult to take it out of the abdominal cavity, and so, the application is limited for such cases.
Vigilance should be raised for patients with a history of abdominal surgery because the postoperative adhesions can increase the risk of bowel damage when incising the peritoneum. Although PREP-IT leads to less bowel irritation when compared with the transperitoneal approach, the potential risks cannot be ignored, and so, patients with a history of abdominal surgery are not suitable for this technique, contrary to the traditional retroperitoneal approach. In our study, two patients had a history of abdominal surgery, which were both appendiceal surgeries exclusively, and the risks of bowel damage were well considered by experienced clinical doctors. Another key point for PREP-IT is to close the peritoneal incision. It is widely believed that the incision will be subsequently reperitonealized, and little solid evidence supports the necessity for closure. However, internal hernia might occur with untreated tears as reported, which is rare but sometimes complicated with severe intestinal obstructions. 9,10 Moreover, sufficient bowel preparations were required for PREP-IT because of the peritoneum operation, despite its retroperitoneal route.
In the PREP-IT group, major complications occurred in 2 (3.5%) postoperative patients. According to a previous study on a cohort of 253 patients with renal tumor and VTT in our center, the perioperative occurrence of pulmonary embolism was 2.6%. 23 In another study on 103 patients who experienced IVC interruption in our center, the occurrence of postoperative major complications (defined as Clavien–Dindo Grade ≥3) was 18.8%. 24 Therefore, we consider the occurrence of the three IV complications not unnatural.
In our cases, some other techniques could be applied together with PREP-IT. Segmental IVC resection or IVC transection was performed for complex VTT, including IVC wall invasion and large bland thrombus. 24 For Mayo II to III tumor thrombus, we used the delayed occlusion of the proximal inferior vena cava technique to simplify IVC dissection and exposure, as described previously. 25
Admittedly, this study has some limitations. First, this is a retrospective single-center study, so bias in patient populations cannot be excluded. In addition, while standard and overweight cases are applicable for this technique according to our experience, the potential effect of high BMI (especially BMI ≥30) on PREP-IT cannot be well demonstrated here, considering that the BMI in PREP-IT group ranges from 20.6 to 26.2. Added difficulty is possible for high BMI cases, as the increased belly fat may oppress the abdominal cavity, making the kidney placement difficult, therefore affecting the IVC exposure. Hence, we recommend sufficient preoperative communication for high BMI cases, and if the retroperitoneal workspace is severely oppressed, conversion to open surgery should be considered.
Finally, PREP-IT is more likely to cause postoperative peritoneal adhesions compared with the traditional retroperitoneal approach. However, our follow-up was insufficient to investigate the proportions of adhesion in the long term. Further studies are needed to verify this potential complication.
Conclusions
In conclusion, the PREP-IT is relatively safe and feasible in retroperitoneal laparoscopic right nephrectomy and IVC tumor thrombectomy, allowing for a large workspace and wide exposure for IVC operations.
Footnotes
Acknowledgments
The authors acknowledge the staff of the Department of Urology, Peking University Third Hospital, and the patients who participated in this study.
Authors' Contributions
All authors read and approved the final article. Conception and design: J.C., Z.L., and X.Z. Administrative support: S.Z., L.M., H.Z., and C.L. Acquisition of data: G.W., X.T., Y.T., L.G., K.C., and Y.L. Data analysis and interpretation: X.L., Q.G., Q.Z., and P.H. Article writing: All authors.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This study was supported by the National Natural Science Foundation of China (Grant No.: 82273389) and the Cohort Construction Project in Peking University Third Hospital (Grant No.: BYSYDL2019010).
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.