
Abstract
Objective:
The aim of the study was to characterize artificial stones used for research in endourology in terms of radiological properties and hardness, based on stone fragmentation, and to compare them with real stones.
Materials and Methods:
We built artificial stones using BegoStone Plus™ powder (BEGO, Lincoln, RI), with powder (g)–water (mL) ratios ranging from 15:03 to 15:12. The CT Gemstone Spectral Imaging Software® (GE Medical Systems, LLC, Waukesha, WI) was used to evaluate the radiological density in HU and spectral properties. Stone fragmentation was assessed in an in vitro experimental setting. These properties of artificial stones were compared with real urinary calculi.
Results:
Regarding radiological density in terms of HUs, 15:03 artificial calculi showed similar results when compared with real stones comprising calcium oxalate and calcium phosphate. The 15:03 and 15:04 artificial stones showed similar spectral property results to calcium pyrophosphate stones. The 15:11 artificial stones showed similar stone fragmentation results to real stones comprising uric acid, and 15:03 artificial calculi showed similar results to apatite and cystine stones.
Conclusions:
Artificial stones are useful for research in endourology. Stones with a powder (g)–water (mL) ratio of 15:03 proved to mimic real hard stones in terms of HUs, atomic number, and stone fragmentation in our study and could be used as artificial hard stones, and 15:11 stones showed similar stone fragmentation to uric acid stones. Our study might suggest that standard Bego stones are useful to investigate different areas in endourology, but not radiological properties because radiological homogeneity is not ensured unless more sophisticated mixing methods are used.
Introduction
Urinary calculi cause one of the most prevalent diseases in urology worldwide. 1 –4 As technology designed for management of urinary stones with endourologic procedures gains momentum, 5 experimental models are being developed to gain knowledge on how to use the new devices safely and effectively. 6 –8 Many of these models are in vitro platforms for testing laser properties. 9 –11 Many trials involve artificial stones built using BegoStone™ powder or similar materials. 8 –12
BegoStone is a commercially available plaster that was originally developed for dental applications. 13 Artificial stones made using BegoStone proved to be reproducible and show mechanical properties mimicking the range of acoustic properties and tensile fracture strength of real urinary calculi. 14 BegoStone can provide a consistent and reliable phantom material for in vitro and in vivo studies on stone fragmentation. 13
However, our knowledge about these artificial stones is limited. Optimizing the understanding about these artificial stones would improve experimental accuracy. The aim of the study was to further characterize artificial stones used for in vitro and in vivo experiments in endourology while comparing them with real stones. Artificial stones were assessed by studying their radiological density in HUs, spectral properties with effective atomic numbers, and hardness based on stone fragmentation. They were compared with real urinary stones.
Materials and Methods
Stones
Ten types of artificial stones using BegoStone Plus powder (BEGO, Lincoln, RI) were built with powder (g)–water (mL) ratios of 15:03, 15:04, 15:05, 15:06, 15:07, 15:08, 15:09, 15:10, 15:11, and 15:12.
Bego stones were produced following the method proposed by Esch and colleagues. 15 The mixture was placed in a plastic bowl. A standard laboratory mixer was used to mix the powder and water. The mixture was then deposited in plastic molds with the exact same configuration, measuring 6 × 6 × 5.5 mm. The mixture was left to dry for 72 hours at room temperature in the plastic mold. Homogeneous weight was ensured.
The real stones were collected from the state biochemistry laboratory and stone bank. The stones used were from patients with stone disease history and previously analyzed, with their composition confirmed using Fourier transform infrared spectroscopy. Some of these real stones were pure and some were mixed stones. Stones varied in weight, size, and shape.
For the experiment with laser lithotripsy to test fragmentation rates, only stones with homogeneous weights, compared with the artificial stones produced for the study, were used. If the real stone was too heavy and/or large, it was lasered beforehand to convert it into lighter/smaller stones that could be comparable by weight and size with the Bego stones produced.
The real stones comprised uric acid, magnesium ammonium phosphate, calcium phosphate, calcium oxalate, ammonium urate, and cystine.
Three stones of each type, real and artificial, were used for the experiment.
Radiological properties
Stones were placed on a single gel platform bed and identified with codes (Fig. 1A). The GE Revolution CT® scanner (GE Medical Systems, LLC, Waukesha, WI) and CT Gemstone Spectral Imaging (GSI®) software (GE Medical Systems, LLC) were utilized to assess the radiological density and spectral atomic numbers. The GSI software provides the effective atomic number.

Experimental settings.
The stone density was obtained in HUs. Spectral curves from the artificial stones' effective atomic numbers were built by the software. The GSI software was then able to determine which type of real stone the sample was characteristically most similar to. Real stones underwent the same tests as artificial stones and their results were compared.
All the stones, artificial and real, were scanned under identical settings. The GSI software was used for all stones tested at an energy range of 40 to 140 kV with 10-keV incremental increase to analyze the HUs and develop the associated spectral HU curve.
Stone fragmentation assessment
An in vitro experiment was performed to set stone ablation. Real and artificial stone comparability was assessed. Stone ablation was defined as weight before laser lithotripsy minus weight after laser lithotripsy. The experimental setting (Fig. 1B) consisted of a rounded, transparent plastic jar (10 × 10 × 20 cm) filled with saline.
The laser fiber was introduced through an 8F 84-cm guide catheter (Cook Medical, Indiana) in an 18F 30-cm Amplatz renal dilator (Cook Medical), which was stabilized and fixed by a 22F 30-cm Amplatz renal dilator (Cook Medical) inside a plastic cylinder on a vertical setting to avoid the bias of stone retropulsion. A Lumenis® Pulse P120H Holmium Laser System (Lumenis Ltd., Yokneam, Israel) and a 365-μm D/F/L fiber (Lumenis Ltd.) were used.
Laser settings were set at 1.5 J × 20 Hz = 30 W for the long pulse modality. Each stone was lasered for 30 seconds. The laser fiber was fixed before starting the experiment, keeping the fiber tip at a 2-mm distance from the stone. All real and artificial stones were moistened in physiologic saline for 24 hours before the experiment. The stones were weighed (when dry) blindly by two researchers (B.B.M and D.S.M.) with an electronic compact scale 72 hours before and after the experiment.
The experiment for each stone type was independently performed three times with different stones of the same composition, size, and weight. As 14 types of stones were tested, 42 trials were performed in total.
Statistical analysis
Mean values were calculated for all stone types in the three independent trials for each. The mean values, standard deviations, spectral curves, and histograms for the radiological property assessment were provided by the GSI software. A quantitative analysis for the stone ablation experiment was performed using SPSS, v25, software (IBM Statistics, NY).
Results
Figure 2 shows how data were provided by the GSI software. The GSI software provides a histogram with the distribution of the atomic number of each pixel within the area selected according to the known effective atomic numbers of known real stone compositions. The software gives the most similar real stone. It also displays the spectral curve of the target area and HUs. These figures were obtained for every stone tested. The software gave an analysis of monochromatic images at 70 keV and quantitatively calculated the average effective atomic number and HUs.
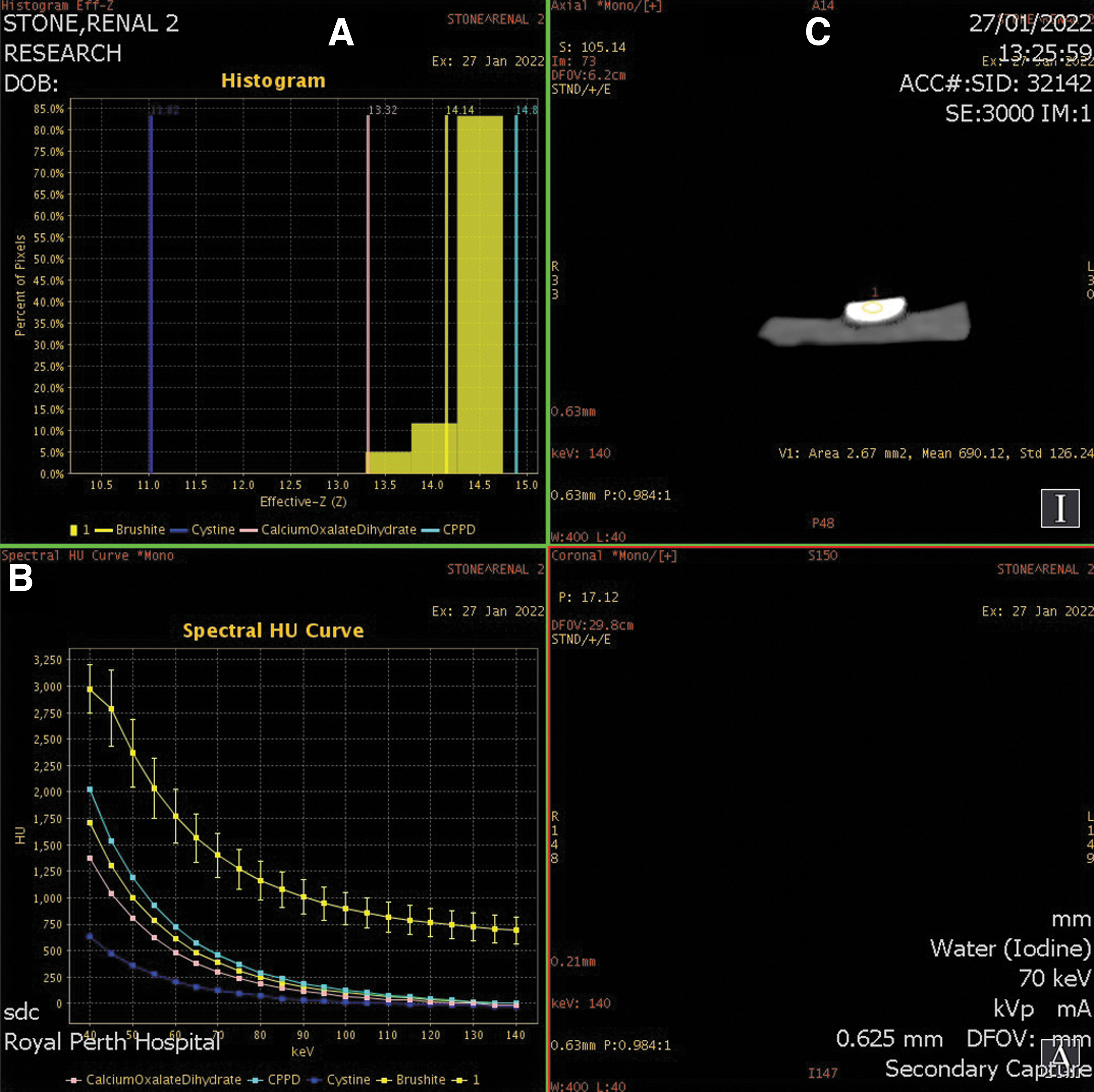
Example of data was provided by the GSI software. Histogram
Regarding radiological properties, in terms of HUs, 15:03 artificial calculi showed a mean HU value of 2182 + −292.03, similar to real stones comprising calcium oxalate and calcium phosphate, 2121 + −104.5 (Table 1). However, there were large standard deviations in the HUs probably due to the energy level that was set when HUs were calculated, which was 70 keV.
Radiological Density in Hounsfield Units Calculated for Every Type of Stone Tested, Scan, Mean Atomic Numbers, and Real Stone Match as per Computed Tomography Using the Gemstone Spectral Imaging Software
Brushite = calcium hydrogen phosphate dihydrate; CPPD = calcium pyrophosphate; SD = standard deviation.
The 15:03 and 15:04 artificial stones were similar to calcium pyrophosphate (CPPD) stones in terms of atomic number and spectral properties. The GSI software was accurate only for uric acid stones, cystine calculi, and calcium oxalate stones in terms of atomic number and spectral properties (Table 1). Likewise, there were large standard deviations in the HUs.
In the stone ablation experiment, the softer Bego stones, that is, with more water in their composition, had a greater ablation rate. Ablation rates of real stones met expected values according to their known hardness. The 15:11 artificial stones showed similar results to uric acid stones, and 15:03 artificial stones showed similar results to apatite and cystine stones (Fig. 3).
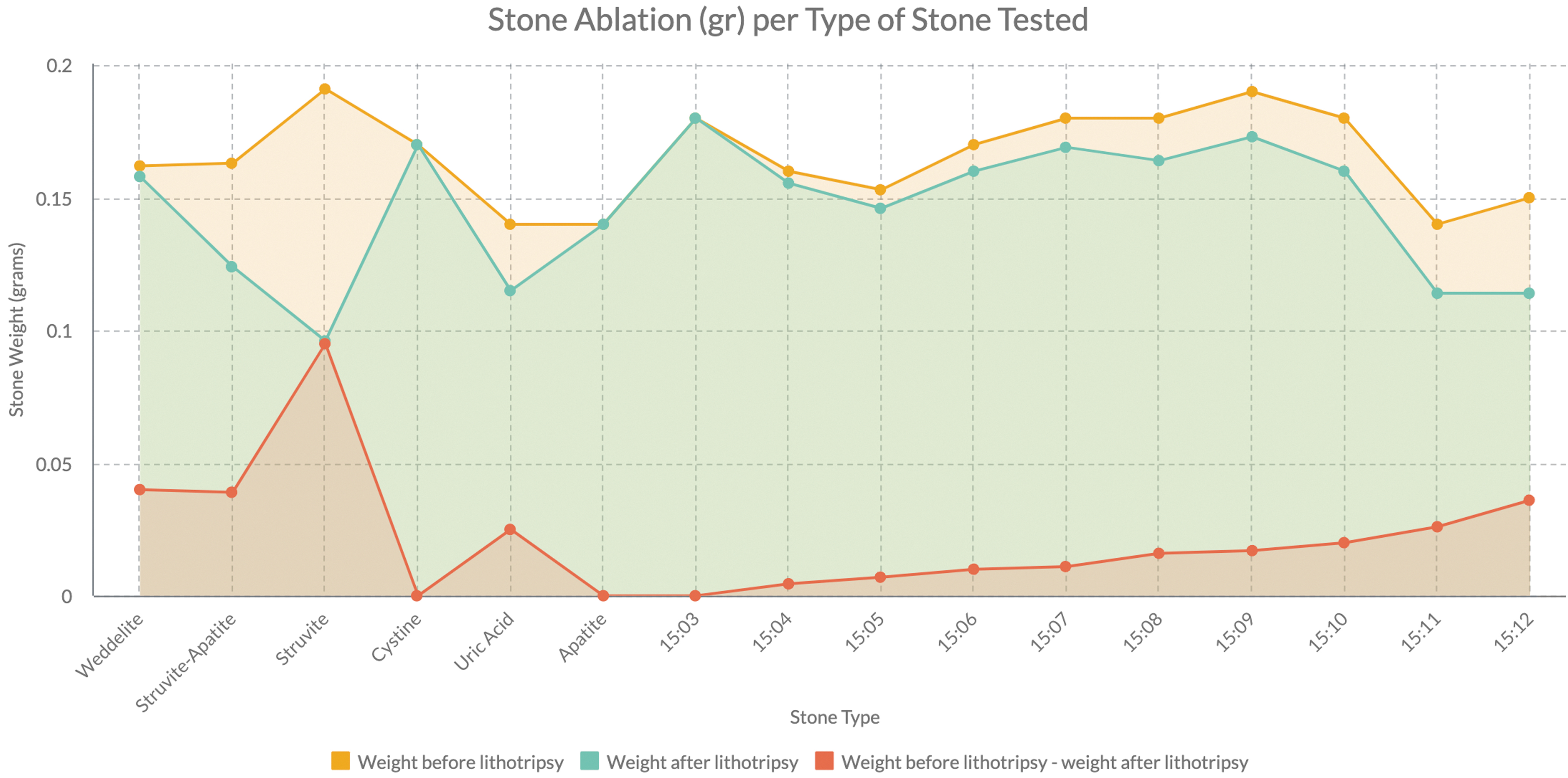
Mean stone ablation (g) per type of stone tested. All stones were lasered for 30 seconds at laser settings of power, energy, and frequency of 1.5 J × 20 Hz = 60 W at the long pulse modality. Stone ablation was defined as weight before laser lithotripsy − weight after laser lithotripsy.
Discussion
Bego stones built with powder–water ratios ranging from 15:03 to 15:12 were compared with real calculi, in terms of radiological density and spectral properties, using the GSI software and hardness, in terms of stone ablation, with an in vitro custom experimental model.
New technologies in endourology for stone treatment are gaining momentum. Preclinical studies are useful for learning how to optimally use the new technologies. Many in vitro and in vivo studies with artificial stones have been performed. 8 –10,12 However, there is still room for improving current knowledge on properties of these phantom stones.
Esch and colleagues proposed a method to build artificial stones using BegoStone Plus powder. 15 Simmons et al. performed diametral compression testing and ultrasound transmission tests to characterize the Bego stones based on their acoustic properties. They found that the tensile fracture strength and acoustic properties of these stones match a wide variety of real calculi. 14
Esch and colleagues prepared stones with a powder (g)–water (mL) ratio ranging from 15:03 to 15:06. They assessed the acoustic properties with an ultrasound transmission technique. They concluded that 15:03 Bego stones could be acoustically comparable with real stones comprising calcium oxalate. Similarly, according to our results, 15:03 Bego stones mimic real urinary stones with calcium as a major component based on the properties assessed.
According to Esch and colleagues, 15:06 Bego stones could be acoustically comparable with real soft stones such as uric acid. However, according to our study, it is the 15:11 Bego stones that are comparable with soft stones such as uric acid in terms hardness from their ablation properties. This could be explained because they did not test hardness, but they estimated the mechanical properties of Bego stones based on the elastic wave theory from the acoustic properties that they measured.
When the 15:06 stones were lasered in our experiment, they showed lower ablation than uric acid or magnesium phosphate stones. This suggests that 15:06 artificial stones are harder than real uric acid or magnesium phosphate stones.
According to Liu and Zhong, the physical properties of BegoStone are comparable with hard renal calculi such as calcium oxalate monohydrate stones. BegoStone is much denser and harder than phantom stones made of plaster of Paris. 13 When they compared fragmentation rates of Bego stones, plaster of Paris stones, and real calcium oxalate stones using extracorporeal shockwave lithotripsy, they found that BegoStone was more difficult to fragment than plaster of Paris phantoms, but the trends in stone comminution were similar for both phantoms. 13
Our experiments showed that at least in terms of stone ablation, 15:11 Bego stones were comparable with soft stones such as uric acid. Perhaps not only plaster of Paris but also Bego stones comprising enough water (from 15:11 on) are softer and comparable with soft stones in terms of stone ablation.
Based on stone ablation, the experiment was reproducible and avoided bias of retropulsion. The values for artificial stones followed a logical order, that is, the harder the stones, the lesser the weight difference they showed before and after fragmentation, meaning there was less fragmentation.
The 15:03 Bego stones were comparable with real stones comprising calcium oxalate and calcium phosphate and not any other powder–water ratio tested. However, there were large standard deviations in HUs, which were related to multiple factors and can be explained by the energy level that was set when HUs were calculated, which was 70 keV set automatically by the GSI software.
Most in vivo CT scans are conducted at an energy level between 70 and 120 keV. This is highly dependent on the patient's body habitus, where increased energy is required for larger patients. For our in vitro experiment with no surrounding material to be attenuated by X-rays, lower energies were used.
There can be larger standard deviations of HUs at lower energy levels due to multiple factors such as material composition effects, photoelectric absorption dominance, quantum noise, and beam hardening. The material composition of artificial stones should be homogeneous. However, this may be an area of error and variability as the material was mixed until smooth by the shaker, and due to dealing with small quantities of material areas, this may lead to varying densities even within the small molds used.
At lower kiloelectron volt levels, the photoelectric effect becomes more dominant in X-ray interactions with the stones. Furthermore, at lower energy levels of X-rays, there are fewer photons leading to lower signal levels, which can increase the impact of statistical noise and can also lead to significant HU variations.
Finally, the effect of beam hardening, which occurs at these low energy levels, is observed when X-rays are preferentially absorbed, resulting in a high mean energy for the remaining X-rays. This can lead to nonuniformity in the X-ray spectrum and variations in HU measurements. However, there was a linear relationship between stone ablation rates and water quantity, that is, the softer the artificial Bego stone, the more the ablation. Therefore, artificial stones were built properly from that perspective.
Artificial stones are normally used for research purposes that do not include radiological endpoints. Our study might suggest that Bego stones built with our methods are useful to investigate different areas in endourology, such as intrarenal pressure, intrarenal temperature, stone retropulsion, and stone ablation, but not HUs because radiological homogeneity is not ensured with the described method.
Regarding atomic number and spectral properties, the GSI software was accurate for uric acid stones, cystine calculi, and calcium oxalate stones. It was not accurate for stones comprising struvite as a major component. There are data suggesting that the software has sensitivity and specificity values of 100% and 99.7%, respectively, for uric acid stones. 16 –22 The validity for other types of stones was not as accurate in this study. The software uses the atomic number of crystals of CPPD, which are common in gout disease, but not in renal stone disease.
Based on atomic numbers, the software was able to set the most similar real stones according to the Bego stones tested, and it was expected that 15:03 and 15:04 artificial stones showed similar results to CPPD stones in terms of atomic number and spectral properties.
Understanding the physical characteristics of urinary calculi and how stone composition influences their fragmentation is key to improve the understanding on lithotripsy. 23 –25 However, to our knowledge, a comparison with real urinary calculi has not yet been performed. A significant amount of knowledge on new laser technologies for laser lithotripsy is based on experiments using artificial Bego stones. The more we learn about these stones, the more accurate we will be when designing and understanding the research in this field.
A limitation of the study might be that neither pure real stones nor artificial stones softer than 15:12 were tested and nor were other varieties of powder used to build stones. Nonetheless, the hardest stones that were built proved to mimic really hard stones based on the properties assessed. Likewise, despite some authors pointing that Bego stone is a superhard material, 13 in our study, the soft stones that were built, from 15:11 on, showed similar ablation rates compared with real soft stones.
Another limitation of the study may be the fact that in the production of artificial stones, they were not dried on a sonicating plate, but at room temperature, freely. However, no air bubbles were observed. All stones looked exactly as the one in Figure 1, and when fragmented, no air bubbles were observed either.
Conclusions
Stones with a powder (g)–water (mL) ratio of 15:03 proved to mimic real hard stones in terms of HUs, atomic number, and stone fragmentation in our study and could be used as artificial hard stones, and 15:11 stones could mimic uric acid stones in terms of stone fragmentation. Our study might suggest that standard Bego stones are useful to investigate different areas in endourology, but not radiological properties because radiological homogeneity is not ensured unless more sophisticated mixing methods are used.
Footnotes
Acknowledgment
The authors would like to thank Mr. Robin Williams, Senior Scientist in charge, Special Chemistry Laboratory, PathWest Fiona Stanley Hospital (Perth, Australia).
Authors' Contributions
B.B.M. was involved in project development, experiment design and performance, supervision, data collection, data analysis, manuscript writing, and manuscript review.
D.S.M. was involved in project development, experiment design and performance, data collection, manuscript writing, and manuscript review,
A.T. and V.T. were involved in data analysis, manuscript writing, and manuscript review.
A.P., I.A., Y.Y., M.L., S.L., E.L., and P.K. were involved in project development, experiment design, and manuscript review.
C.T. was involved in project development, experiment design and performance, and supervision.
M.C. and S.V.D.W were involved in project development, experiment design and performance, supervision, and data collection.
M.S.S. was involved in project development, experiment design, data analysis, and manuscript review.
M.R. was involved in experiment design and performance, data collection, and manuscript review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.