
Abstract
Background:
This systematic review and meta-analysis investigated whether peritoneal interposition flap (PIF) prevent lymphocele formation after robot-assisted radical prostatectomy with extended pelvic lymph node dissection.
Materials and Methods:
We performed a systematic review and cumulative meta-analysis of the primary outcomes according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, Assessing the Methodological Quality of Systematic Reviews guidelines and risk-of-bias tool. Five databases, including Medline, PubMed, Cochrane Library, Scopus, and Web of Science, were systematically searched. The time frame of the search was set from the creation of the database to February 2023.
Results:
Meta-analysis of symptomatic lymphoceles (sLCs) rates revealed significant difference between PIF and no PIF group (eight studies pooled; p = 0.005), The sLCs rates account for 2.6% (28/1074) and 7.1% (85/1186) in the PIF and no PIF group, respectively. The resulting odds ratio was 0.34 (95% confidence interval: 0.16–0.73), taking into account the heterogeneity of these studies (Q = 14.32, p = 0.05; I 2 = 51%).
Conclusion:
PIF is an effective intraoperative modification on the prevention or reduction of sLC, which is worthy of further clinical promotion.
Systematic Review Registration:
National Institute for Health and Care Research, identifier CRD42022364461
Introduction
Prostate cancer is one of the most prevalent malignant tumors affecting the urogenital system. According to the Global Cancer Statistics Report 2020, which was published by the International Agency for Research on Cancer in February 2021, prostate cancer accounted for 7.3% of all malignant tumors worldwide, with 1,414,259 new cases in 2020, making it the third most common cancer after breast and lung cancer. In addition, there were 375,304 prostate cancer deaths in 2020, which accounted for 3.8% of all malignant tumors and ranked eighth in terms of mortality rate. 1 Since the introduction of robot-assisted laparoscopic prostatectomy (RALP) in the United States in 2000, it has rapidly become the preferred surgical approach for prostate cancer, favored by many doctors and patients. In particular, RALP has been widely accepted by young doctors. 2
Robot-assisted radical prostatectomy (RARP) combined with pelvic lymph node dissection is a major cause of symptomatic lymphoceles (sLCs), with a prevalence ranging from 2% to 10%. 3 Large cysts can compress the bladder, causing or exacerbating voiding irritation syndrome. 4 Furthermore, compression of the external iliac vessels can result in deep vein thrombosis in the lower extremities and secondary lymphatic inflammation.
We investigated the impact of various intraoperative modifications on the prevention or reduction of sLCs. 4,5 In 2015, Lebeis et al. introduced the peritoneal interposition flap (PIF) as a simple intraoperative modification to reduce sLCs in patients undergoing RALP. 6 Based on follow-up studies, 7 –13 PIF currently appears to be the most promising method for reducing or preventing robotic pelvic lymph node dissection (PLND)-related sLCs. Various surgical techniques have been proposed by different authors with the aim of reducing the incidence of lymphocele formation during RARP. These techniques and methods involve manipulation of the peritoneum, including dissection, fixation, and suturing.
Authors differ in their specific approach to the surgical procedure. Lebeis et al. suggested creating a peritoneal window during the pelvic lymph node dissection. 6 Dal Moro and Zattoni employed the Preventing Lymphocele Ensuring Absorption Transperitoneally (P.L.E.A.T.) technique, which includes lymphatic vessel clearance, reanastomosis, and suturing of a triangular flap onto the peritoneum. 9 Stolzenburg et al. described the technique of four-point peritoneal flap fixation (4PPFF). 12 Lee et al. inverted and sutured the peritoneum inward to cover the area of lymph node dissection. 11 Bründl et al. followed Lebeis' original method. 8 Student Jr et al. performed peritoneal separation and fixation onto the pubic bone. 13 Gloger et al. utilized bilateral peritoneal flap technique. 10
Although there are differences in the specific procedural steps, the common goal of all these techniques and methods is to prevent lymphatic fluid accumulation and lymphocele formation. In addition, the timing of these surgeries is consistent, as they are performed during RARP, usually concurrent with pelvic lymph node dissection. However, a comprehensive analysis of existing studies is lacking. As a result, we conducted further studies on PIF and performed a meta-analysis comparing sLC rates between PIF and no PIF groups after PLND in RALP.
Materials and Methods
Literature search
This meta-analysis has been reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards and is fully compliant with the PRISMA 2020 statement. 14 The quality assessment was performed according to Assessing the Methodological Quality of Systematic Reviews 2 and risk-of-bias tool (RoB2), which was rigorously described and was fully consistent for each question. 15,16 This systematic review has been registered with PROSPERO (CRD42022364461).
The literature search and selection process were performed independently by two authors, with disagreements between authors resolved by negotiation of a third reviewer (T.W.) when an agreement could not be reached. We systematically and comprehensively searched five databases, PubMed, Embase, Scopus, Medline, and Cochrane, for published trials up to February 2023. The following MeSH and main keywords were used: “prostate cancer,” “robot-assisted radical prostatectomy” “pelvic lymph node dissection,” “symptomatic lymphoceles,” “peritoneal flap” (or) “peritoneal interposition flap” (or) “P.L.E.A.T.,” and associated terms. The language was not restricted. Also, manual searches of the reference lists in the selected studies to retrieve all relevant data have been implemented.
Eligibility criteria
We included only retrospective, prospective, and randomized controlled trials (RCTs) study designs. The inclusion criteria of the meta-analysis were defined as follows: retrospective, prospective, or RCTs studies on RARP attributable to localized prostate cancer, in which the influence of a PIF on the formation of sLCs was analyzed comparatively. The following exclusion criteria were considered for our study: (1) All non-RCTs, nonretrospective studies, nonprospective studies, case series, and case reports will be excluded. (2) Studies (any RCTs) that could not provide available outcome data for extraction will be excluded. (3) Trials not reported in English. (4) Editorials, conference abstracts, letters, or expert opinions. (5) Laboratory or animal studies.
Two authors (J.Z. and L.Z.) independently assessed the identified studies and reviewed the abstracts to select full articles.
Discussion was performed among all authors to resolve any disagreements. The study endpoint of sLCs was identical in the selected studies ([fever as a symptom of an infected lymphocele, lower abdominal pain, lower extremity swelling, and/or deep vein thrombosis] in combination with a pelvic fluid formation).
Study quality assessment
Based on the initial search results, the Newcastle-Ottawa Scale (NOS) was used to assess the quality of the retrospective and prospective studies. 17 This scale includes the three domains of selection, comparability, and exposure, with scores above six stars identifying high-quality studies. Student Jr. et al. 13 and Gloger et al. 10 were RCTs, therefore, RoB2 was used for assessing the quality too. 15
Data extraction
Two review authors (Junjie Zhou and Lin Zhou) independently extracted the data from the included studies using an Excel spread sheet/previously designed data extraction form. Extracted data will be then cross-checked between the two authors, and any discrepancy resolved by consensus discussion. Data were to be extracted from the studies, comprising study characteristics (first author, year of publication, country, study design, study settings, study period, participants of RARP+PLND, participants of RARP+PLND+PIF), participants' characteristics [age, body mass index (BMI) and lymph nodes count], and perioperative (including fever as a symptom of an infected lymphocele, lower abdominal pain, lower extremity swelling, and/or deep vein thrombosis in combination with a pelvic fluid formation) outcomes.
Statistical analysis
The primary endpoint of this meta-analysis was the sLC rate and assessed using odds ratios (ORs). We divided patients into intervention groups (PIF), control groups (no PIF) based on whether PIF was performed. We conducted this systematic review according to the suggested present protocol and the recommendations by The Cochrane Reviewers' Handbook. 18 The statistical analysis was performed by me Dr. Junjie and was further confirmed by another reviewer. We did the meta-analysis using Review Manager Software (RevMan version 5.4; Cochrane Collaboration, Oxford, UK). I reported 95% confidence intervals (95% CIs) and p-values for all outcome indicators.
The q and χ 2 tests were used to verify the level of heterogeneity among the included studies. Differences were considered significant if I 2 > 50%. Based on the results of the heterogeneity test, I 2 ≥ 50% or p < 0.1, a random-effects model was used to pool the estimates. Conversely, a fixed-effects model was utilized. Meta-analyses of continuous variables was performed using the inverse variance method, and dichotomous variables were pooled using the Mantel–Haenszel method. In addition, further sensitivity analyses were performed for those studies with a high degree of heterogeneity (I 2 ≥ 50% or p < 0.1)
Results
Description of studies
The researchers retrieved 146 records from five databases. After reading titles and author names, 37 duplicate studies were excluded. When study topics, abstracts, and keywords were considered, 45 records unrelated to the study topic were excluded, and the remaining 17 studies were reviewed for completeness. Complete information could not be extracted for two articles, there were also seven reviews and letters, so we excluded them.
Finally, five retrospective studies, one prospective study, and two RCTs studies including 2260 patients were included in the review (Fig. 1). Table 1 provides the baseline data extracted from each of the included studies. This includes the author's name, year of publication, study center, type, sample, procedure, BMI, and other records.
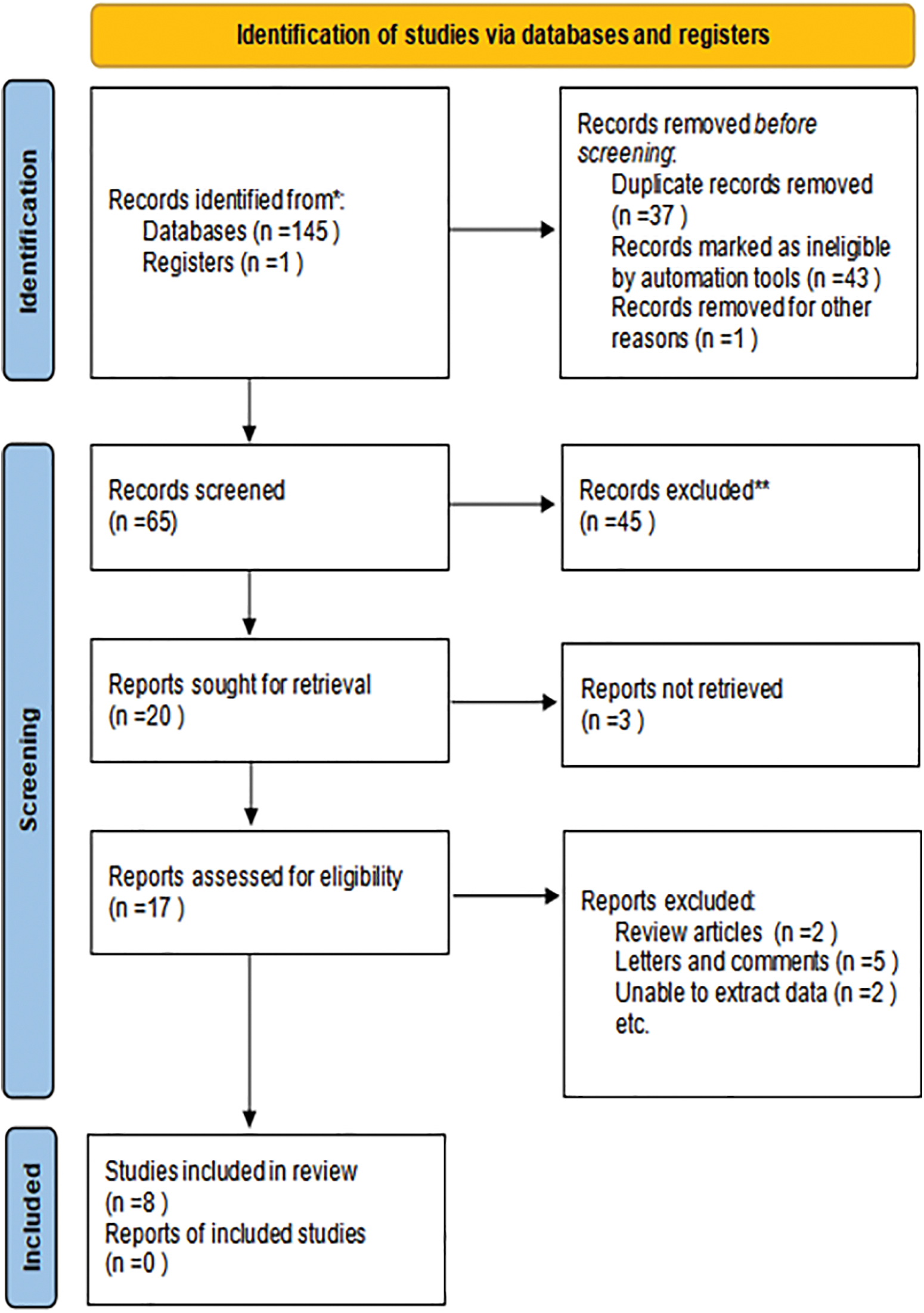
Flow diagram of the study selection process. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Color images are available online.
Baseline Data for Studies Included in the Meta-Analysis
BMI = body mass index; IQR = interquartile range; LN = lymph nodes; NA = not available; PIF = peritoneal interposition flap; RCT = randomized controlled trial; SD = standard deviation.
Quality assessment
Table 2 shows the NOS study quality rating scores for the included studies. All studies were high-quality, with ratings of more than six stars. Figure 2 shows the conclusions of the quality assessment based on the RoB2. 17

Risk of bias for included randomized controlled trials. Color images are available online.
Quality Score of Included Studies Bases on the Newcastle-Ottawa Scale
AE = ascertainment of exposure; AF = study controls for other important factors; AFU = adequacy of follow-up of cohort (≥80%); AO = assessment of outcome; DO = demonstration that outcome of interest was not present at start of study; FU = follow-up long enough for outcomes to occur; REC = representativeness of the cohort; SC = study controls most important factors; SNEC = selection of the none posed cohort.
Outcomes
Meta-analysis of sLCs rates revealed significant difference between PIF and no PIF group (eight studies pooled; p = 0.005), The sLCs rates account for 2.6% (28/1074) and 7.1% (85/1186) in the PIF and no PIF group, respectively (Fig. 3). The resulting OR was 0.34 (95% CI: 0.16–0.73), taking into account the heterogeneity of these studies (Q = 14.32, p = 0.05; I 2 = 51%; Fig. 3).
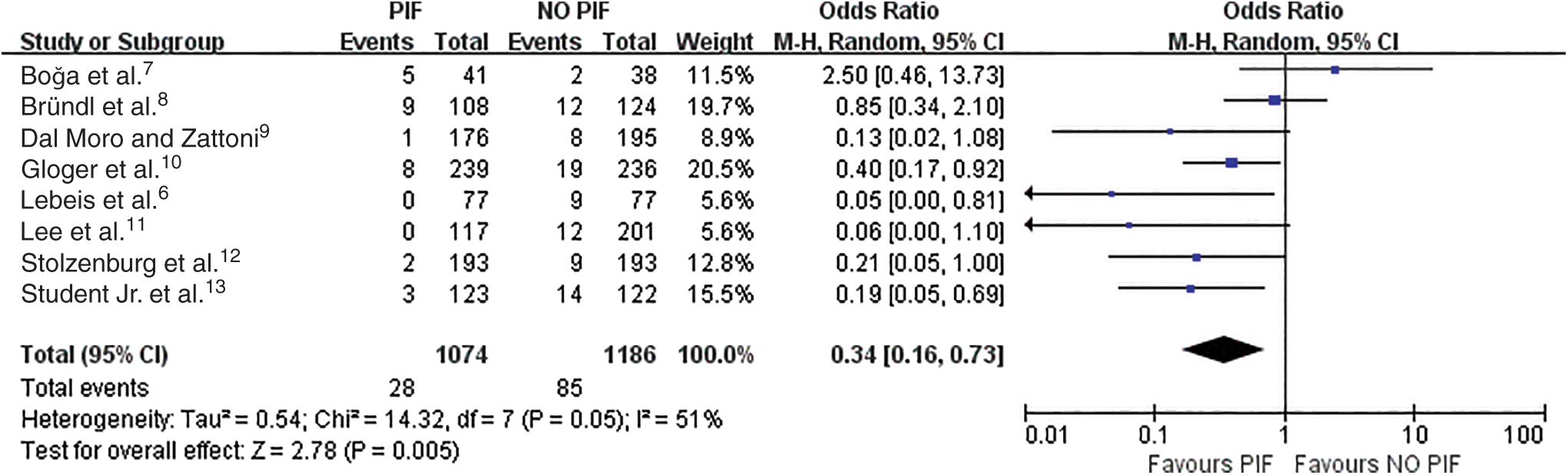
Forest plot from the results of the eight studies available assessing cumulative incidence of the endpoint sLCs after RARP and PLND in the groups PIF vs no PIF. CI = confidence interval; M–H = Mantel–Haenszel; PIF = peritoneal interposition flap; PLND = pelvic lymph node dissection; RARP = robot-assisted radical prostatectomy; sLC = symptomatic lymphocele. Color images are available online.
Discussion
The results of the meta-analysis of the eight studies mentioned earlier showed that the sLC rate was reduced 66% (95% CI: 1%–99%) in the PIF group. In all studies, the rationale for PIF to reduce or prevent sLCs is the same: to ensure that lymphatic fluid can enter the peritoneal cavity from the pelvis and to increase the area of peritoneal absorption.
In 2015, Lebeis et al. first proposed and implemented PIF, 6 a procedure performed by two surgeons in a single center who used the existing peritoneum covering the bladder to create a peritoneal window that allowed lymphatic fluid to continue into the peritoneal cavity to be reabsorbed in the event of a lymphatic fistula, thereby reducing the incidence of symptomatic lymphatic cysts. A total of 154 eligible patients were included in this study, and 77 patients who underwent PIF were compared with 77 patients who did not, suggesting that PIF is beneficial in reducing the incidence of postoperative symptomatic lymph node cysts.
Dal Moro and Zattoni proposed P.L.E.A.T. 9 performed by the same surgeon (Fabrizio Dal Moro) in a single center, which to some extent avoids bias arising from differences in the proficiency or skill of multiple surgeons. One hundred seventy-six patients with PIF compared with 195 patients without PIF, the P.L.E.A.T. technique is a rapid, cost-effective, easy-to-perform, and safe method to reduce the risk of sLC after transabdominal robotic PLND.
Stolzenburg et al. 12 modified the method proposed by Lebeis et al. 6 All four surgeons sutured the peritoneal abdominal wall incision ends (anterior and lateral pelvic walls on both sides) at four points after extended pelvic lymph node dissection (ePLND), exposing the peritoneal surface to the iliac vessels and closed fossa, called 4PPFF, the larger peritoneal exposure area of 4PPFF facilitates more fluid absorption compared with the two-point fixation method of Lebeis et al. 6 Also, peritoneal fixation prevents excessive bladder flexion, thus reducing postoperative urinary problems in patients. 4PPFF is a safe and effective method to prevent lymphatic cysts in patients with radical prostatectomy combined with PLND.
In the study by Lee et al. in which a single surgeon (Daniel D Eun) performed trans-anterior peritoneal RARP and PLND in all patients, 11 they retrospectively compared 117 PIF patients with 201 no PIF patients, and the procedure and outcomes were similar to Lebeis et al. 6 suggesting that the risk of symptomatic lymphoceles after RARP and bilateral PLND can be significantly reduced.
However, some scholars have argued that PIF does not provide any benefit to patients, but rather increases the operative time and the risk of lymphatic cyst formation. In the study by Boğa et al., 7 transperitoneal robot-assisted radical prostatectomy and ePLND were performed by two surgeons in a single center on 79 patients, respectively, and postoperatively 41 patients had PIF performed by one of the doctors, whereas the other 38 patients did not. This study was the main source of heterogeneity differences in this meta-analysis, and if the study of Boğa et al. was excluded, 7 the heterogeneity of this meta-analysis would have been greatly reduced, with I 2 dropping to 38%. We believe that this may be related to the small sample size of the single center and the proficiency and experience of the surgeon's surgical skills.
Bründl et al. 8 came to similar conclusions as Boğa et al. 7 In this single-blind multicenter prospective study, 108 patients who received PIF compared with 124 patients who did not receive PIF found that the use of PIF was not statistically significantly associated with the development of symptomatic lymphatic cysts, the reduction in the volume of lymphatic cysts, and notably, they did not significantly affect the PIF patients' postoperative urinary function in a favorable opinion.
In addition, we included two new studies in which 123 patients underwent PIF and 122 patients did not in the prospective randomized single-center unilateral blinded study of Student Jr et al. performed by two experienced surgeons, 13 who further modified the approach of Lebeis et al. by fixing a peritoneal free flap (PerFix) to the pubic bone to reduce the occurrence of lymphatic cysts. 6 Unusually, they used CT to assess for the presence of lymphatic cysts.
This is more accurate than cystography and ultrasound detection, which may also have contributed to the lower overall incidence of lymphatic cysts in patients with PerFix (24%) than in those without PerFix in the study by Student Jr et al. 13 (36%) (PerFix) significantly reduced the incidence of symptomatic lymphatic cysts. In another multicenter prospective RCT by Gloger et al., 10 239 patients received bilateral PIF, and 217 patients did not. Fixation of bilateral cystoperitoneal flaps to the endopelvic fascia significantly reduced the overall incidence of lymphatic cysts and the incidence of symptomatic lymphatic cysts in the treatment group.
Conclusion
Our meta-analysis showed that PIF was effective in preventing the incidence of sLCs. For patients undergoing RARP with pelvic lymphadenectomy, compared with no PIF group, the sLC rate was reduced 66% (95% CI: 1%–99%) in the PIF group. It was statistically significant (p = 0.005). PIF is an effective intraoperative modification on the prevention or reduction of sLC, which is worthy of further clinical promotion.
Footnotes
Acknowledgments
We thank Mr. KumyuanLi and Dr. Wu for providing continuous encouragement to Dr. Jun-jie Zhou to pursue his career in medicine.
Authors' Contributions
T.W. and X.D. conceived and designed the experiments. J.Z., L.Z., and Y.T. analyzed the data. H.S., Q.X., and X.M. contributed reagents/materials/analysis. J.Z. and S.W. wrote the article. All the authors have read and approved the final article.
Provenance and Peer Review
Not commissioned, externally peer-reviewed.
Author Disclosure Statement
All the authors have nothing to declare.
Funding Information
This study was supported by City of Nanchong Strategic Cooperation with Local Universities Foundation of technology (Grant Nos. 20SXQT0305 and 18SXHZ0321), The Application and Basic Research Program of Sichuan Science and Technology Department (Grant No. 2022NSFSC0804), The Primary Health Development Research Center of Sichuan Province Program (Grant No. SWFZ21-C-98), The Medical Research project of Sichuan Medical Association (Grant No. S21061).