
Abstract
Introduction:
Holmium laser enucleation of the prostate (HoLEP) has evidenced-based advantages in treating benign prostatic hyperplasia (BPH) relative to other interventions. Unfortunately, the adoption of HoLEP has remained relatively low in Medicare and the National Surgical Quality Improvement Program populations. HoLEPs role as an inpatient surgical intervention is changing as advancements in the technique and systems have demonstrated the feasibility of same-day discharge. Thus, our objective was to evaluate national HoLEP trends in ambulatory surgery settings from 2016 to 2019.
Materials and Methods:
The Nationwide Ambulatory Surgery Sample (NASS) is the largest national all-payer database of ambulatory surgical encounters, managed by the Agency for Healthcare Research and Quality. A cross-sectional retrospective analysis of the 2016 and 2019 NASS was performed. Rates of BPH surgeries were calculated and stratified by age, census region, and primary payer to compare across time points for trends. Chi-squared tests and two-sample t-tests were completed for categorical and continuous variables, respectively.
Results:
The total number of ambulatory BPH surgeries fell 20% between 2016 (n = 124,538) and 2019 (n = 100,593). In 2016, HoLEP lagged behind photoselective vaporization of the prostate (PVP) and transurethral resection of prostate (TURP) with 4.7% of surgeries but rose to the second most common procedure in 2019 with 8.3% of total surgeries. TURP was the most common intervention (62.6% in 2016, 90.7% in 2019). Simple prostatectomy was the most expensive intervention. By U.S. census region, more HoLEPs were carried out in the South (43.1% in 2016, 37.5% in 2019) and Midwest (26.8% in 2016, 31.7% in 2019).
Conclusions:
Overall, HoLEP uptake is increasing. HoLEP has replaced greenlight PVP as the second most frequently used intervention. The rate of ambulatory HoLEPs has nearly doubled despite a general decrease in the number of surgeries.
Introduction
Holmium laser enucleation of the prostate (HoLEP) is a minimally invasive endourologic procedure indicated for treatment of size-independent benign prostatic hyperplasia (BPH). 1,2 While transurethral resection of the prostate (TURP) still remains the gold standard surgical treatment of BPH, over the past several decades, HoLEP has been shown to have evidenced-based advantages relative to TURP, photoselective vaporization of the prostate (PVP), and other interventions. 3,4 Studies have demonstrated that patients undergoing HoLEP have shorter catheter duration times, decreased blood loss, and shorter hospital lengths of stay (LOS) compared with TURP. In addition, in comparison to simple prostatectomy (SP) (open, robotic, and laparoscopic), HoLEP demonstrates similar functional improvements but lower complication rates. 5
Despite these advantages, the adoption of HoLEP has remained relatively low in the past decade based on Medicare and the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) data. 6,7 In a study by Robles et al. 7 evaluating Medicare claims from 2008 to 2014, HoLEP consisted of just 4% of BPH procedures performed in the United States in 2014, but adoption had increased from 2008 to 2014. Similarly, Anderson et al. 6 found based on the NSQIP data from 2011 to 2015 that HoLEP accounted for 4% to 5% of annual BPH surgical volume while conferring the lowest LOS, transfusion, readmission, reoperation, and urinary tract infection rates.
While HoLEP was previously considered an inpatient procedure requiring an overnight stay, more recently, advances in laser technology have allowed for more efficient hemostasis leading to a paradigm shift from an inpatient to a same-day discharge outpatient surgical procedure. 6,8 The Healthcare Cost and Utilization Project (HCUP) Nationwide Ambulatory Surgery Sample (NASS) is the only national all-payer database of ambulatory surgical encounters, managed by the Agency for Healthcare Research and Quality. 9 Usage of this database may be more inclusive of patients not insured under Medicare. The objective of this study was to evaluate national and regional HoLEP trends in ambulatory surgery settings from 2016 to 2019.
Materials and Methods
Study design
After obtaining institutional review board approval, we performed a cross-sectional analysis using the 2016 and 2019 HCUP NASS. This database is built off the State Ambulatory Surgery Services Database with 34 states and the District of Columbia participating, accounting for 83% of the U.S. population and 76% of all ambulatory surgery encounters. Encounters are restricted to those with at least one major ambulatory surgery performed in a hospital-owned facility. 9 Ambulatory surgery refers to any outpatient procedure that requires anesthesia (general, regional, or sedation) in which the patient is discharged same-day as the procedure. Hospital-owned facility is defined as any facility (clinic or hospital) associated financially with a hospital providing inpatient care. Outpatient clinic- or office-based procedures under local anesthesia and privately owned facilities are not included. The sampling strata developed by the HCUP have produced weighted estimates of the 10.6 million encounters in 2016 and 11.8 million in 2019.
We narrowed the study population using the codes from the Current Procedural Terminology (CPT) to identify patients undergoing BPH surgery including laser enucleation of the prostate with morcellation (52649), TURP (52601, 52630—for regrowth), laser vaporization of the prostate (52648), transurethral needle ablation (TUNA [53852], transurethral microwave therapy [53850]), Rezum™ (53899), and SP including open, laparoscopy-, and robot-assisted laparoscopic techniques (55831/55821, 55899). The assumption was made that the majority of laser enucleation procedures were HoLEP, and laser vaporization procedures were PVP. Rezum was not included in the 2016 NASS because the CPT code did not exist at that time. The CPT code for laparoscopic SP, 55867, was not released until 2023, so we were unable to differentiate between uptake trends of open, laparoscopic, and robotic SP.
Continuous variables examined included: patient age (≥18 years) and procedure cost (U.S. Dollars). Categorical variables included: type of BPH surgery, discharge destination, and hospital census region. Procedure cost was defined as cost of an entire ambulatory surgery visit. The total cost is not specific to a single procedure and cannot be generalized toward total facility cost.
Statistical analysis
Statistical analysis was performed using SPSS®, version 28 (IBM Corp., Armonk, NY), and SAS® software, version 9.4 (SAS Institute, Inc., Cary, NC). Rates of BPH surgeries were calculated and stratified by age and census region to compare across time points for trends. Two-sample t-tests and chi-squared tests were completed using weighted calculations for continuous and categorical variables, respectively, with p-value <0.05 considered statistically significant.
Results
In 2016, there were a total of 124,538 BPH surgeries performed including TURP, PVP, HoLEP, SP, and TUNA (Table 1). The average age of patients undergoing TURP was 71.3 years in 2016 and 71.4 years in 2019. HoLEP patients were of similar age at a mean of 70.0 years in 2016 and 70.4 years in 2019. The mean age of patients undergoing PVP increased from 71.2 years in 2016 to 74.3 years in 2019. SP patients were youngest, with an average age of 66.6 years in 2016 and 67.7 years in 2019. Patients undergoing Rezum were oldest out of all BPH procedures in 2019 at an average age of 75.2 years.
Number of Benign Prostatic Hyperplasia Surgeries in 2016 Compared with 2019
p < 0.05.
HoLEP = holmium laser enucleation of the prostate; PVP = photoselective vaporization of the prostate; TURP = transurethral resection of prostate.
Of all the ambulatory BPH surgeries performed in both years, TURP was the most predominant with 77,979 encounters (62.6% of total BPH surgeries in 2016), and PVP was the second most prevalent with 40,625 (32.6%) encounters. HoLEP was the third most common BPH procedure with 5850 (4.7%) encounters. The least common procedures were SP (72 encounters) and TUNA (13 encounters). In 2019, there was a slight decline in the number of ambulatory BPH surgeries at 100,783 total procedures including all procedure types from 2016 as well as Rezum. TURP increased to encompass 90.7% (91,411) of all encounters (p < 0.0001), and HoLEP rose to become the second most common BPH procedure at 8389 encounters (8.3%, p < 0.0001).
The number of PVPs performed in 2019 declined drastically compared with 2016 from 32.6% to 0.7% (697 encounters, p < 0.0001). Other less commonly performed procedures included SP (229 encounters), Rezum (25 encounters), and TUNA (32 encounters). Overall, the number of BPH procedures fell by 20%, but the number of HoLEPs performed increased, and the proportion of HoLEPs to total BPH surgeries nearly doubled (Fig. 1).
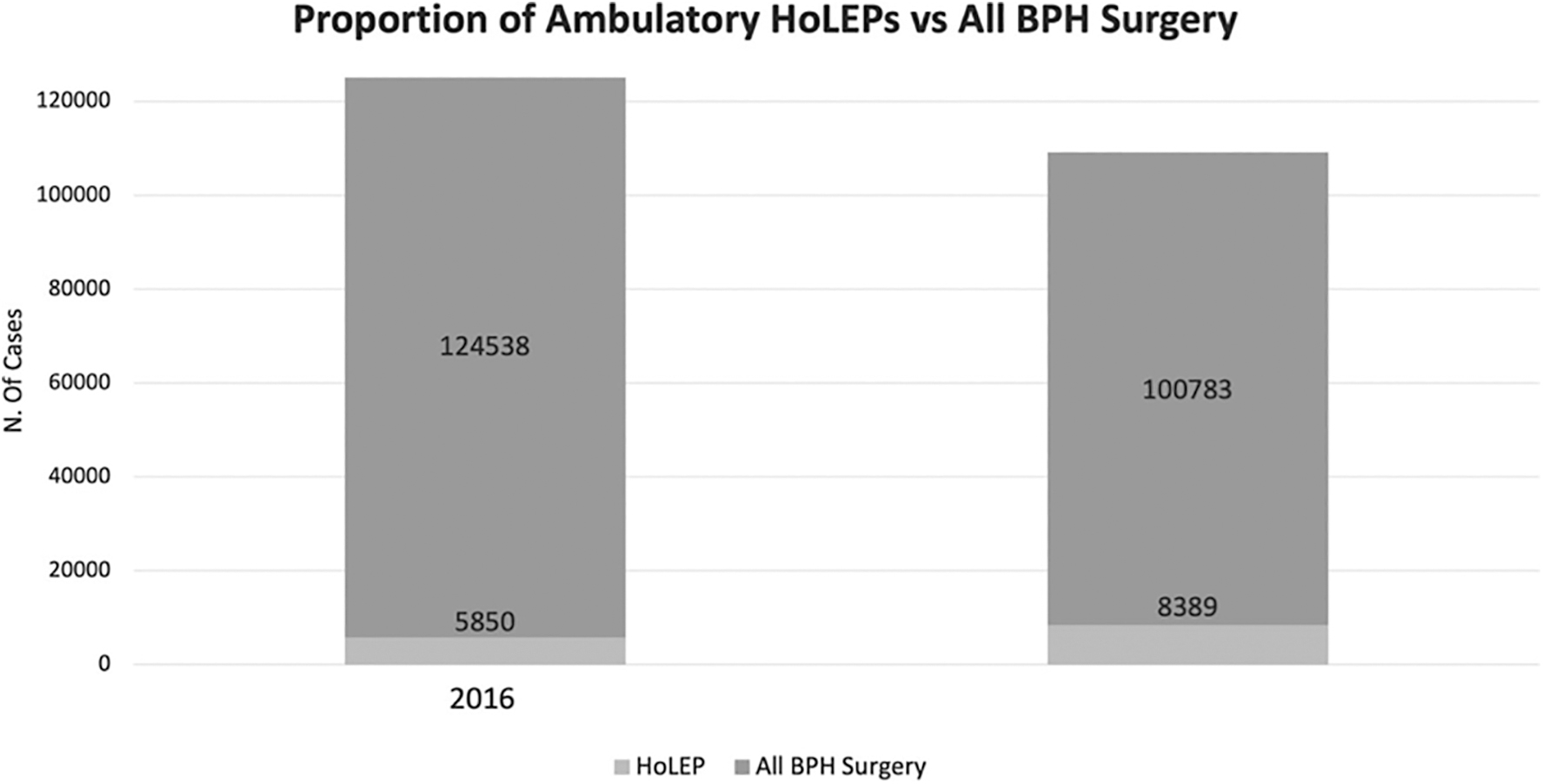
Proportion of ambulatory HoLEP procedures performed in 2016 and 2019 compared with the total number of BPH surgeries. BPH = benign prostatic hyperplasia; HoLEP = holmium laser enucleation of the prostate.
Geographic regional uptake of HoLEP in 2016 and 2019 is displayed in Table 2. The Southern and Midwestern United States were the regions with the highest and second highest number of HoLEPs, respectively, in 2016 and 2019. The Southern region encompassed 43.1% of all HoLEPs performed in 2016, which decreased slightly to 37.5% in 2019. The Midwest region accounted for 26.8% of HoLEPs performed in 2016, which increased to 31.7% in 2019. Thus, the discrepancy between the two regions narrowed from 2016 to 2019. The percentage of HoLEP uptake in the Northeast region was relatively stable from 17% in 2016 to 17.8% in 2019 as was the Western region (13.1% in 2016 to 13% in 2019).
Percentage of Holmium Laser Enucleation of the Prostate Performed in 2016 and 2019 Based on U.S. Geographic Region
Table 3 displays the average costs of BPH procedures in 2016 and 2019. Overall, the cost of all BPH surgeries increased over time from 2016 to 2019. The most expensive BPH surgery was the SP, with a mean charge of $39203.60 in 2016, which increased to $48706.30 in 2019 (p = 0.038). HoLEP was the second most expensive BPH procedure, with an average cost of $23880.40 in 2016 and $30416.70 in 2019 (p < 0.0001). PVP was slightly cheaper than HoLEP at $20203.50 in 2016 and $28391.20 in 2019 (p < 0.0001). TURP was the least expensive of the BPH surgeries, with an average charge of $19899.90 in 2016 and $25799.50 in 2019 (p < 0.0001). Cost of TUNA increased from $8318.42 in 2016 to $27200.97 in 2019. The cost of Rezum in 2019 was $30209.89. From 2016 to 2019, the absolute cost increase was greatest for TUNA at $18882.55, followed by SP at $9502.70 and lowest for TURP at $5899.60. PVP increased by $8187.70, and HoLEP increased in average cost by $6536.30.
Average Cost of Benign Prostatic Hyperplasia Procedures in 2016 and 2019
p < 0.05.
BPH = benign prostatic hyperplasia; SP = simple prostatectomy; TUNA = transurethral needle ablation.
Discussion
This is the first study, to the best of our knowledge, that analyzes HoLEP uptake trends throughout the United States using the NASS database. Prior studies have utilized the NSQIP database, which uses Medicare claims data, which potentially exclude a large portion of the patient population given that privately insured patients are not included in this subset. 9 Our analysis showed that the percentage of HoLEPs being performed nationwide has increased from 4.8% in 2016 to 8.3% of all ambulatory BPH procedures in 2019, an absolute increase of 3.5% despite a slight decrease in the overall number of BPH surgeries performed from 2016 to 2019. The decline in ambulatory BPH procedures could potentially be due to a shift toward office-based procedures or medication-based management. Robles et al. 7 previously reported that HoLEP accounted for 1% of all BPH procedures back in 2008 and 3.3% in 2014. Similarly, Anderson et al. 6 reported rates of HoLEP uptake at around 5% in 2015. Based on these trends, our results demonstrate that the rates of HoLEP are still low, at <10% of all ambulatory BPH surgeries but appear to be slowly increasing.
Interestingly, our study showed that while there was a temporary rise in popularity in PVP in 2016, which accounted for approximately one third of all BPH procedures that year, the proportion of PVPs performed in 2019 diminished to just 0.7% of all cases in 2019. HoLEP has since replaced PVP as the second most popular BPH surgical modality in 2019. TURP continued to remain the most popular procedure being performed nationwide, with the percentage of procedures being performed increasing from 62% in 2016 to more than 90% in 2019. Prior studies have shown that PVP was consistently second in popularity to TURP from 2011 to 2015 at around 30% for all 4 years, which is consistent with our 2016 findings. 6
The reasoning behind the dramatic reduction in PVP procedures over the course of our study timeline is hard to elucidate with certainty. However, this may be due to the fact that compared with TURP, PVP has additional side effects of dysuria and higher rates of reoperation. 10,11 PVP does not allow for pathological analysis of the prostatic adenoma to check for the presence of cancer. Furthermore, there could have been a shift toward performing more office-based procedures, which is not reflected in the NASS.
On a regional basis, our study findings demonstrated that HoLEP remains most popular in the Midwest and Southeast regions of the United States, with both accounting for more than 60% of HoLEPs nationwide. The proportion of HoLEPs performed in the Northeast and West regions remained largely unchanged from 2016 to 2019. Robles et al. 7 identified hospital referral regions (HRR) that performed 10 or more HoLEPs from 2008 to 2014 based on Medicare claims data and found that the highest proportion of HRRs performing >10 HoLEPs per year were in the New England, Southeastern, and Western regions of the United States. Part of the reason behind this regional bias could be due to the lack of access to large-volume HoLEP centers in certain regions, which can affect both trainee experience due to lack of exposure and patient experience due to need to travel long distances to seek out a HoLEP-trained urologist. Trainees may also tend to stay in a similar geographic region after completion of training, further exacerbating this regional predisposition.
The steep learning curve for HoLEP could be another reason as to why HoLEP uptake continues to lag significantly behind TURP. Studies have shown that it takes anywhere between 20 and 50 cases to achieve competency in performing this procedure. 12,13 In addition, in a study by Jiang et al. investigating relative value units (RVUs) of commonly performed BPH procedures per hour of operating room (OR) time, HoLEP was estimated to compensate at ∼9.4 RVUs per hour compared with 19.1 for TURP and 15.5 for PVP, indicating that there is less of a financial incentive for providers to learn and perform HoLEP. 14 This, compounded by the lack of exposure during training at many institutions across the United States, continues to be a large barrier to increasing access to HoLEP.
The usage of the NASS database allowed for identification of trends in average cost of BPH procedures from 2016 to 2019, a unique aspect of our study. We found that the cost of all BPH procedures studied increased significantly from 2016 to 2019. The dramatic increase in the cost of TUNA could have been related to the small patient cohort causing data to be skewed. HoLEP was slightly more expensive than PVP by about $2000 in 2019 but much cheaper compared with SP with an absolute difference of about $18,000. The slightly higher cost of HoLEP compared with PVP and TURP could potentially be related to costs of specialized equipment including the use of a morcellator.
The NASS database does not account for itemized costs, OR time length, or surgical center LOS making this difficult to clarify for certain. Ambulatory BPH procedures in general have been shown to be safe, feasible, and significantly cheaper than inpatient procedures even when accounting for possible readmission costs. 15,16 Same-day HoLEP in particular has been shown to have significantly lower hospital-related costs in China. 17 In a study by Salonia et al. 18 investigating average hospitalization costs for open prostatectomy compared with HoLEP in Italy in 2004, costs for HoLEP were found to be 9.6% lower comparatively. This, in combination with lower overall procedural costs, shorter catheterization times, and decreased blood loss, provides additional evidence to the benefits of HoLEP over SP. 5
One limitation of our study is that the NASS only includes select high-volume ambulatory surgical procedures, so lower volume and office-based procedures such as Urolift™ and Rezum are either not included or severely underestimated in this study. Our study only includes cross-sectional data from 2016 to 2019 and does not include data from 2017 to 2018. This limits our ability to analyze uptake velocity over time and to corroborate our findings of the increase in HoLEP uptake in 2019. Furthermore, CPT codes such as 52648 “laser enucleation of the prostate” and 52649 “laser vaporization of the prostate” are not solely exclusive to HoLEP and PVP and potentially include other less common forms of laser enucleation and vaporization leading to an overestimation of the true uptake of HoLEP and PVP.
Finally, the NASS only samples from hospital-owned facilities. As a result, privately owned ambulatory surgery centers and hospitals are excluded from the database, which may affect overall procedure numbers. However, given that the NASS accounts for 76% of ambulatory surgery encounters, we believe that it is still highly representative of uptake trends in BPH surgery in the United States.
Conclusions
HoLEP uptake continues to increase in the ambulatory surgical setting. While PVP was previously the second most common BPH surgical intervention, HoLEP has since replaced PVP in popularity. The rate of ambulatory HoLEPs being performed has nearly doubled despite a general decrease in the annual volume of BPH surgeries. Despite these promising trends, HoLEP adoption continues to lag significantly behind TURP. Further investigation will be necessary as same-day HoLEP becomes increasingly recognized as a safe and feasible option.
Footnotes
Authors' Contributions
J.N.G.: Software, formal analysis, validation, writing—original draft, writing—review and editing. N.A.M.: Conceptualization, methodology, formal analysis, software, writing—original draft, data curation. M.S.L.: Writing—review and editing, supervision. N.S.D.: Writing—review and editing. M.A.A.: Writing—review and editing. A.E.K.: Conceptualization, writing—review and editing, resources, supervision.
Author Disclosure Statement
M.S.L. is a consultant for Lumenis. A.E.K. is a consultant for Ambu, Boston Scientific, Lumenis, Sonomotion, and Virtuoso Surgical. She is a board member of Sonomotion and Uriprene.
Funding Information
No funding was received for this article.