
Abstract
Introduction:
New opioid dependency after urologic surgery is a serious adverse outcome that is well-described in the literature. Patients with stone disease often require multiple procedures because of recurrence of disease and hence are at greater risk for repeat opioid exposures. Despite this, opioid prescribing after urologic surgery remains highly variable and in an emergency setting, opioids are still used commonly in management of acute renal colic.
Methods:
Two literature searches were performed using PubMed. First, we searched available literature concerning opioid-sparing pathways in acute renal colic. Second, we searched available literature for opioid-sparing pathways in ureteroscopy and percutaneous nephrolithotomy (PCNL). Abstracts were reviewed for inclusion in our narrative review.
Results:
In the setting of acute renal colic, multiple randomized control trials have shown that nonsteroidal anti-inflammatory drugs (NSAIDs) attain greater reduction in pain scores, decreased need for rescue medications, and decreased vomiting events in comparison with opioids. NSAIDs also form a core component in management of postureteroscopy pain and have been demonstrated in randomized trials to have equivalent to improved pain control outcomes compared with opioids. Multiple opioid-free pathways have been described for postureteroscopy analgesia with need for rescue narcotics falling under 20% in most studies, including in patients with ureteral stents. Enhanced Recovery After Surgery protocols after percutaneous nephrolithotomy are less well described but have yielded a reduction in postoperative opioid requirements.
Conclusions:
In select patients, both acute renal colic and after kidney stone surgery, adequate pain management can usually be obtained with minimal or no opioid medication. NSAIDs form the core of most described opioid-sparing pathways for both ureteroscopy and PCNL, with the contribution of other components to postoperative pain outcomes limited because of lack of head-to-head comparisons. However, medications aimed specifically at targeting stent-related discomfort form a key component of most multimodal postsurgical pain management pathways. Further investigation is needed to develop pathways in patients unable to tolerate NSAIDs.
Introduction
The opioid epidemic is one of the most prominent public health challenges facing the United States today, with 80,411 opioid-related deaths reported in 2021. 1 A major source of opioids is prescription medication that is available as a result of diversion of unneeded or overprescribed medication. 2 There is mounting evidence of overprescription of opioids in urology with several studies from 2010 to 2020 showing that >60% of patients had leftover opioid medication after recovery from urologic surgery. 3,4 Notably, postoperative opioid prescribing practices are extremely variable, even among endourologists. 4 –6 For example, in a 2021 survey of Endourological society members, 1/4th of respondents reported prescribing opiates >50% of the time postureteroscopy. 5
Alarmingly, new opioid dependency in individuals undergoing urologic surgery is not uncommon, with estimated risks ranging from 4% to 14.8%. 6 –9 Specific to stone disease, up-front prescriptions of narcotics for acute renal colic (especially larger prescriptions) has been shown to be associated with prolonged or refilled prescriptions before definitive intervention, as well as long-term use after completion of treatment. 6,8,10,11 Furthermore, individuals who received postoperative opioid prescriptions from >1 provider after ureteroscopy for stone disease were found to be at increased risk for prolonged use (>1 month postoperative). 12
A study by Berger et al. included 11,915 patients undergoing endoscopic treatment for stones—of this group, those who were prescribed >100 oral morphine equivalents (OME) were at 34% increased risk of chronic opioid use (>10 refills postoperatively). 6 Although female gender and high school education level was associated with slightly increased odds of chronic opioid use, further investigation into patient-level factors associated with persistent opioid use after surgery is needed. Identification of these risk factors could be leveraged into development of clinical tools to quickly assess risk for postoperative opioid dependence.
Although evidence of far-reaching harms from opioids prescribed for acute renal colic and postoperative pain for stone disease are apparent, efforts to address them have not been consistent. In fact, although the Centers for Disease Control (CDC) has made concerted efforts to address opioid prescribing for chronic pain, limited guidance has been provided for management of acute pain episodes such as for treatment of renal colic or after surgery for kidney stones.
To address these problems, especially in the context of extreme variability in opioid prescribing, the European Association of Urology (EAU) and American Urological Association (AUA) have made concerted efforts to provide prescribing guidelines for practitioners. 13 –15 Despite this, urologic guidelines on management principles of acute renal colic are limited, with much of the recent research focus being placed on postoperative prescribing.
Because of potential lasting implications of even short courses of opioids, there is a need to understand the evidence basis behind opioid-sparing pathways in kidney stone disease. The purpose of this contemporary review is to outline the role of non-narcotic and narcotic-minimizing treatment strategies in the management of (1) acute renal colic and (2) postoperative pain management after kidney stone surgery.
Methods
For the purposes of this narrative review, a literature search was performed in April 2023 using the PubMed database for English full-text articles. No publication date limitations were placed on the initial literature search. Citation searching was used to supplement the PubMed query. Two separate searches were performed to assess pain management in the setting of (1) acute renal colic (2) postoperatively after surgical interventions for stones. Search terms for acute renal colic included “pain,” “management,” “acute,” “renal,” and “colic.” All 319 abstracts were reviewed for relevance by the first author (Fig. 1).

PRISMA flowchart of included studies regarding acute renal colic. *Initial study screening done by manual review of titles and abstracts (if available) through PubMed. Articles without full-length English-language versions available or with irrelevant topics based on review of titles/abstracts were excluded. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Search terms for postoperative pathways included “ureteroscopy,” “percutaneous nephrolithotomy,” “pain,” and “opioid.” This yielded 95 abstracts, which were reviewed by the first author for relevance (Fig. 2). A total of 11 studies were identified (9 for ureteroscopy and 2 for percutaneous nephrolithotomy [PCNL]), which specifically measured efficacy of opioid-sparing pathways after stone surgery. This is inclusive of four retrospective cohort studies, three prospective cohort studies, and four randomized control trials (RCTs).
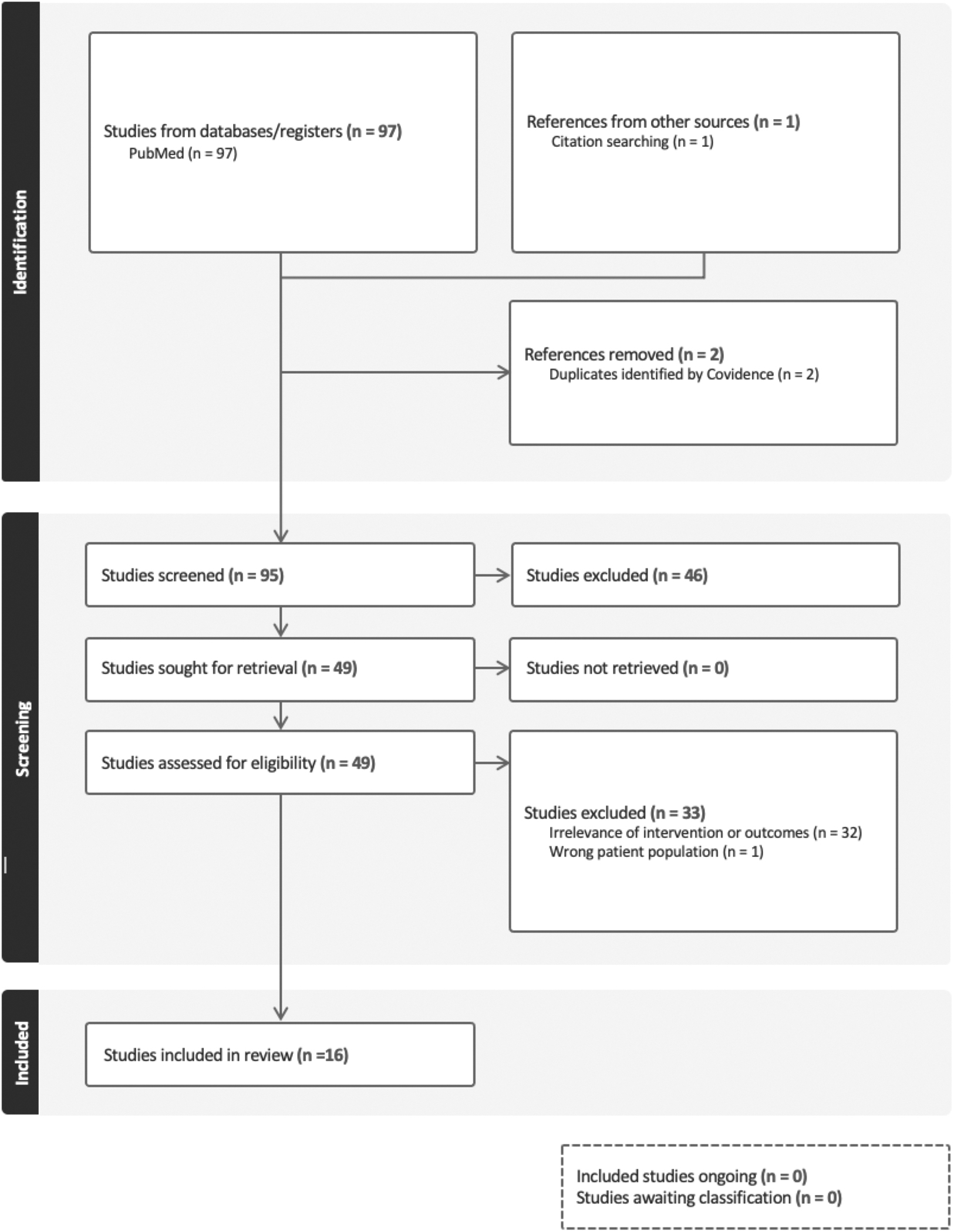
PRISMA flowchart of included studies regarding postoperative pain management. *Initial study screening done by manual review of titles and abstracts (if available) through PubMed. Articles without full-length English-language versions available or with irrelevant topics based on review of titles/abstracts were excluded.

Summary of opioid-sparing perioperative pain management options for ureteroscopy and PCNL. PCNL = percutaneous nephrolithotomy.
Results
Management of acute renal colic
Acute renal colic caused by the presence of obstructing ureteral stones is a common chief complaint leading to emergency department (ED) visitation with a lifetime incidence of 2% to 5%. 16 Prompt and effective pain control is a key tenant of management of these patients in an emergency room setting. Although opioids traditionally have held a central role in ED pain control, there is extensive evidence that multimodal regimens can reduce or eliminate their use.
Comparison of nonsteroidal anti-inflammatory drugs vs opioids for management of acute renal colic
A landmark Cochrane Review was published by Holdgate and Pollock in 2004, providing substantial evidence in support of nonsteroidal anti-inflammatory drug (NSAID) use for first-line pain management over opioids in patients presenting to the ED with acute renal colic. This study included 20 RCTs, which compared cyclooxygenase-2 (COX-2) inhibitors or aspirin to opioids with primary outcomes, including (1) pain score by visual analog scale (VAS) post-treatment, (2) complete resolution of pain, (3) need for rescue dosing of additional analgesic, and (4) incidence of vomiting. 16
Notably, improvements in VAS pain scores were larger in patients treated with NSAIDs compared with opioids (mean difference 4.60 points on 100-point scale, 95% confidence interval [CI]—7.50 to −1.70, p = 0.002) and need for rescue medication was also rarer (relative risk [RR] 0.75, 95% CI 0.61–0.93, p = 0.007). 16 Finally, emesis was 65% less likely in patients receiving NSAIDs (RR 0.35, 95% CI 0.23–0.53, p < 0.001). 16 This analysis was limited by the fact that most RCTs included were small with <50 participants in all but two studies.
More recently, Pathan et al. performed a meta-analysis including 36 RCTs (1982–2016) and compared (1) pain reduction at 30 minutes by VAS pain score, (2) rate of rescue treatment, and (3) rate of vomiting between adults treated with NSAIDs or opioids. 17 Similar to Holdgate and Pollock, a marginal benefit of NSAIDs vs opioids was seen in terms of 30-minute VAS pain scores (mean difference 5.58, 95% CI −10.22 to 0.95, p = 0.01). 17 A 27% reduction in need for rescue analgesia associated with NSAIDs vs opioids was observed (RR 0.73, 95% CI 0.57–0.94, p = 0.01) and a lower risk for vomiting was again seen (RR 0.41, 95% CI 0.24–0.70, p = 0.009). 17
This meta-analysis included only RCTs, but in contrast to the prior Cochrane Review included some larger (>100 patients/arm) trials. 18 It is worth noting that all RCTs included assess either intramucular or intravenous (IV) route of administration. Although differences in pain scores between groups were too small, this meta-analysis provides strong evidence that NSAIDs provide comparable pain control to opioids in management of acute renal colic, reduce the need for rescue opioids, and are associated with fewer episodes of emesis.
Several studies have demonstrated effective reduction of in-ED and ED discharge narcotic prescriptions after targeted interventions to decrease their use. In a 2018 study, Motov et al. introduced a multifaceted practitioner education program aimed at reducing opioid prescription for adults presenting to a tertiary care center with acute renal colic. 19 They observed a 12.7% reduction of in-hospital opioid use and 25% reduction in outpatient opioid prescriptions with simultaneous increased use of NSAIDs.
A similar study at the University of Rochester standardized emergency management of acute renal colic to a stepwise protocol of Tylenol+NSAIDS+IV fluids (first line), IV lidocaine as needed, and opioids only as needed if prior methods failed. 20 More modest reductions in ED (8%) and discharge (8%) opioid prescriptions were seen, with no decrease in patient reported pain scores. 20 However, there was a modest (4%) increase in 7-day ED re-presentation.
It is worth noting that the aforementioned studies only considered in-ED complications such as emesis and did not quantify potential side effects such as acute kidney injury, gastric erosions, or bleeding. Such complications are rare at baseline and mostly associated with chronic use. 15 Patients with hepatic or renal dysfunction were also excluded from most of the included trials. Also worth noting is that adverse medication effects from opioids that occurred after ED discharge were generally not reported in the aforementioned literature. Therefore, given equivalent to improved pain management outcomes associated with NSAIDs, as well as demonstrated feasibility in replacing opioids, NSAIDs should be considered first-line for most patients presenting with acute renal colic, unless otherwise contraindicated.
Acetaminophen vs opioids vs NSAIDs
Parenteral acetaminophen has also been recently described as a potential first-line option for management of acute renal colic. Pathan's systematic review from 2018 included four RCTs (n = 1325 pooled), which compared NSAIDs and acetaminophen (parenteral or PO) in management of acute renal colic. 17 Although no difference was observed in VAS pain scores at 30-minutes postmedication administration between NSAID or acetaminophen groups, NSAIDs were associated with lower need for rescue analgesia (RR 0.56, 95% CI 0.42–0.74, p < 0.001). 17
A more recent large RCT compared 1 g IV acetaminophen with 40 mg IV parecoxib for up-front treatment of renal colic. Similar pain score improvement was seen between the two groups (∼4 points on 10-point VAS scale), with rescue analgesia rates also being similar (35.3% acetaminophen vs 26.7% parecoxib, p = 0.18). 21
Multiple head-to-head comparisons between acetaminophen and opioids have also been performed. 22,23 A meta-analysis inclusive of four RCTs demonstrated that the need for rescue analgesia after 1 g acetaminophen IV for renal colic ranged from 15.8% to 46%. 22 Pooled analysis showed that IV acetaminophen was associated with slightly higher improvements in pain scores compared with IV morphine (difference in mean pain score reduction = 7.5 on 100-point VAS, 95% CI 1.99–13.00; p = 0.008). 22
The largest of the trials included in this analysis (with nearly 500 patients/group) found that IV acetaminophen was superior to morphine in reducing VAS pain scores by >50% at 30 minutes compared (odds ratio [OR] 1.40, 95% CI 1.06–1.85, p = 0.016). 18 Collectively, although IV NSAIDs are associated with more favorable outcomes such as lower need for rescue medication, multiple RCTs suggest that IV acetaminophen is a feasible alternative to IV narcotics for first-line management of acute renal colic.
Alternative analgesics
Although acetaminophen and NSAIDs are first-line options for immediate management of renal colic in an acute setting, the clinician's toolbox is continually expanding, although with varying levels of evidence. A Cochrane Review published by Afshar et al. included six studies that compared NSAIDs with antispasmodics such as hyoscine (an anticholinergic). 24 Results were mixed, in that NSAIDs were more effective than hyoscine (four studies) in lowering pain scores by 50% (RR 2.44, 95% CI 1.61–3.70); however, no differences were seen in total VAS pain score improvement or need for rescue medication. 24 In the context of these findings, anti-spasmodics are not considered first-line or second-line options for management of acute renal colic. 13
The use of alpha-blockers as medical expulsive therapy, particularly for distal ureteral stones is well established. However, there is also substantial evidence of pain reduction associated with alpha-blocker use in acute renal colic, through mechanism of decreasing ureteral spasm and decreasing central nervous system receipt of pain signals. 25 –27 A 2018 double-blind RCT published by Ye et al. randomized 3450 patients with distal ureteral stones to receive daily tamsulosin or placebo and compared stone passage rates as well as needed for rescue analgesia with NSAID suppositories. 27
Patients receiving tamsulosin had lower need for rescue analgesia (9.4% vs 1.9%, p < 0.001) before stone passage or intervention. 27 In contrast, a 2018 RCT of 512 adults discharged with a trial of passage with tamsulosin or placebo found no difference in return to work or re-presentation to an ED because of pain. 28 It is worth noting the study by Ye included only individuals with 4 to 7 mm ureteral stones, highlighting that this subgroup may see the greatest benefit from Medical Expulsive therapy (MET) both in terms of pain relief and stone passage.
A Cochrane Review found that MET was associated with a slight reduction in pain episodes (15 studies, mean difference −0.66, 95% CI −0.91 to −0.42, p < 0.001) and use of rescue diclofenac (14 studies, mean difference −82.41 mg, 95% CI −122.51 to −42.31, p < 0.001). 29 Given these small differences and high variability in standard therapy between studies, the strength of this conclusion may be limited. Adverse effects from tamsulosin in this setting are rare, and include dizziness, vomiting, and retrograde ejaculation, with rates of medication discontinuation because of side effects being 0.6%. 29 Because of the low risk of adverse events and potential benefits of stone passage and modest improvements in pain control, the EAU recommends the use of alpha-blockers specifically for management of renal colic pain. 13
Intranasal desmopressin has been introduced as a treatment option for acute renal colic with a proposed mechanism of inhibition of diuresis to limit collecting system distention and pain. A 2016 review by Jalili et al. found that NSAIDs were superior to desmopressin in terms of pain score reduction and need for rescue treatment (OR 0.31, 95% CI 0.13–0.74, p < 0.01). 30 This systematic review was limited by inclusion of several small studies and inclusion of unpublished data.
Disappointingly, pooled analysis of seven trials showed no difference in need for rescue analgesia in patients treated with NSAIDs+desmopressin vs NSAIDs alone and this was corroborated by a recent randomized placebo-controlled trial. 30,31 IV magnesium sulfate has also been explored in several RCTs, however, has not shown benefit over controls in reducing pain scores in a recent meta-analysis. 32 Therefore, neither desmopressin or IV magnesium are first-line options for management of renal colic.
Postoperative pain management for kidney stone disease
Opioid-free ureteroscopy
Although prescribing patterns remain variable after ureteroscopy, AUA and EAU guidance encourages pursuit of opioid-free (OF) ureteroscopy. 13 –15 Multiple groups have demonstrated success in this endeavor for the past 5 years (Table 1), with mounting evidence that opioid use in this setting is often unnecessary through implementation of Enhanced Recovery After Surgery (ERAS) protocols. Although definitions of what constitutes “opioid-free ureteroscopy” has varied between studies, most have defined this as (1) minimizing intraoperative and Post-Anesthesia Care Unit (PACU) opioids and (2) eliminating routine postoperative opioid prescribing. 33,34 The components of a postureteroscopy, OF regimen have also varied between studies and are summarized in Table 2.
Published Studies on Efficacy of Opioid-Free Pathways After Ureteroscopy
Need for outpatient rescue narcotics, unless otherwise specified.
Acetaminophen 975 mg preoperative. Acetaminophen 975 mg q6h, ibuprofen 600 mg q4–6h, oxybutynin 5 mg q8h, tamsulosin 0.4 mg daily.
Celecoxib 200 mg BID for 3 days, tamsulosin 0.4 mg daily, APAP q6h, oxybutynin 5 mg PRN+preoperative 975 mg acetaminophen, 400 mg celecoxib, 800 mg gabapentin.
APAP = acetaminophen; BID; CI = confidence interval; ERAS = Enhanced Recovery After Surgery; NA = not applicable; OF = opioid free; NSAID = nonsteroidal anti-inflammatory drug; PCNL = percutaneous nephrolithotomy; PDMD = prescription drug monitoring database; POD = post-operative Day; PRN = as needed; RCT = randomized control trial; URS = ureteroscopy; USSQ = Universal Stent Symptom Questionnaire; VAS = visual analog scale.
Components of Published Opioid-Free Ureteroscopy Pathways Organized by Phase of Care
Specific intervention of PO or IV non-narcotic analgesics before procedure. This includes APAP, gabapentin, NSAIDs.
B&O = belladonna-opium; IV = intravenous; PO = parenteral.
Pre- and perioperative components of OF ureteroscopy
A key component of OF ureteroscopy is complete and thorough patient counseling. Several published OF ureteroscopy protocols included targeted counseling of patients in the preoperative setting concerning risks of opioid prescription, adverse effects, and evidence regarding nonopioid multimodals. 33 –36 A key component of counseling is transparent discussion of expected pain levels after ureteroscopy. Talwar et al. demonstrated that postoperative pain severity after OF ureteroscopy normalizes to baseline by 7 days postoperatively, whereas pain interference with daily activities normalized by 14 days postoperatively. 37
Pre- and perioperative pharmacologic interventions as components of OF ureteroscopy are described in several recent studies. Preoperative acetaminophen and gabapentin has been utilized in OF ureteroscopy pathways, 33,36 although there is limited quantitative evidence on the impact of this intervention to overall pain scores in OF ureteroscopy. Intraoperative IV ketorolac is a key component of several OF ureteroscopy pathways, and has been shown in the TRUST double-blind RCT to reduce need for perioperative narcotics by 37%. 33,38,39
The TRUST trial was a double-blind RCT performed at an academic medical center in which 94 patients undergoing ureteroscopy for stone disease were randomized 1:1 to receive 30 mg IV ketorolac on induction vs no NSAIDs. 39 Syed et al. observed a reduction in intraoperative opioid use (17.1 vs 24 OME, p < 0.01) in patients receiving intraoperative ketorolac although no differences were seen in recovery room or postdischarge opioid use. 39
Postoperative pathways in OF ureteroscopy
Postoperative outpatient analgesia for OF ureteroscopy generally focuses on the use of NSAIDs, usually in combination with acetaminophen. 33,36 –38 A variety of different NSAIDs have formed the cornerstone of these protocols, and no head-to-head trials have been performed to assess relative efficacy. Three separate RCTs have demonstrated NSAID-based regimens to have equivalent or superior pain control outcomes compared with opioids alone. 40 –42
In the double-blinded SKOPE trial, Fedrigon assessed postoperative pain scores using the Ureteral Stent Symptom Questionnaire for 81 patients randomized to receive either oxycodone or PO ketorolac on an as needed basis for 5 days after ureteroscopy and stent placement. 41 A lower percentage of individuals in the ketorolac group required rescue narcotics (11/38, 29% vs 21/43, 49%), although this difference was not statistically significant. 41 Days spent in bed because of postoperative pain was lower in the ketorolac group (1.0 vs 2.3 days, p = 0.02). 41
In an RCT including ureteroscopy and percutaneous nephrolithotomy patients, Demasi et al. found lower maximum and average pain intensity scores postprocedurally in patients receiving ketorolac 10 mg q6h as needed vs oxycodone-acetaminophen. 40 This trial was limited by heterogeneity of patient inclusion for a pooled analysis (URS and PCNL, stent and nonstent patients). Similarly, Bamberger found 600 mg ibuprofen to be equivalent to acetaminophen-oxycodone in terms of pain scores, ER visits, and request for rescue opioid medication. 42
Although NSAIDs are a key component of OF pathways in both acute renal colic and after stone surgery, concerns about use in those with renal dysfunction may cause clinicians to hesitate to use them. In a 2020 review, Baker and Perazella highlight the safe use of NSAIDs in minor renal dysfunction. 43 NSAIDs can be cautiously utilized for short courses in patients with CKD, provided risk factors for NSAID-related complications are addressed such as optimizing volume status (i.e., dehydration), correcting hyperkalemia, and ensuring blood pressure control. 43
Especially in patients with CKD Stage 1 to 2, NSAIDs use is acceptable for up to 5-days, when accounting for the aforementioned factors. 43 Dosing recommendations for NSAIDs in healthy patients and though with renal dysfunction are shown in Table 3.
Oral Nonsteroidal Anti-Inflammatory Drug Dosing in the Setting of Mild Renal Dysfunction for Medications Commonly Used for Management of Renal Colic or Postoperative Pain for Kidney Stone Surgery
GFR = glomerular filtration rate.
Addressing stent discomfort in OF ureteroscopy
The use of medications specifically for stent discomfort in OF ureteroscopy was enacted in three prospective 33,35,36 and three retrospective cohort studies 34,37,38 on a scheduled basis. This most commonly included tamsulosin, 0.4 mg daily, with scheduled immediate release or extended-release oxybutynin also commonly prescribed (Table 2). Phenazopyridine is also included as a component of OF ureteroscopy protocol in two studies.
It is worth noting that patients with ureteral stents were included in all three of available RCTs assessing OF ureteroscopy (with two solely including stented patients) and anticholinergics, tamsulosin, and phenazopyridine were not prescribed. This not only highlights the role of NSAIDs in addressing stent-related discomfort, but also points to the feasibility of OF protocols in patients traditionally at risk for higher pain levels after ureteroscopy. 44 The use of alternative agents such as cannabinoid oil and other nontraditional agents in postureteroscopy analgesia has been a recent area of research interest, but a comprehensive review of these data is beyond the scope of this review. 45
Assessing rates of success and treatment failure in OF ureteroscopy
In addition to the previously discussed RCT data, the majority of prospective and retrospective cohort studies have found OF ureteroscopy protocols to be associated with equivalent to superior outcomes compared with opioid-containing postoperative regimens (Table 1). Although exact definitions varied between studies, several studies have shown no difference in ER visits or phone calls regarding pain between OF ureteroscopy protocols vs opioid-containing regimens. 33 –36 For instance, a retrospective analysis of 13,143 patients registered in the Michigan Urological Society Improvement Collaborative who underwent URS from 2016 to 2019 found OF discharge was associated with lower odds postoperative ED visit. 46
Failure of OF ureteroscopy protocols has most commonly been quantified as the rate of filling or using an opioid rescue prescription postoperatively, although time constraints on this definition vary. Reported rates of need for rescue opioids after OF ureteroscopy are generally low and range from 2.3% to 29%. 33 –36,38,41 Inclusive of one RCT, three prospective cohort studies, and two retrospective cohort studies, this accounts for a pooled failure rate of 17.5% (n = 68/387). It is important to consider this number in light of variable definitions, differing rates of opioid-naive patients, and the inclusion of the SKOPE trial in which patients received ketorolac alone and no other prescriptions.
Chronic opioid users present a management challenge for urologists as well. Although some studies excluded individuals who regularly took opioids before kidney stone surgeries, multiple investigators have documented success in OF ureteroscopy pathways for these patients. 33,34,36 For example, Bevill et al. found that patients with chronic pain conditions were not more likely to require salvage narcotics after OF ureteroscopy. 36
Likewise, Gridley et al. found despite inclusion of patients on chronic opioids, there was no difference in clinic calls/prescription requests for narcotics after introduction of OF ureteroscopy compared with historical data. 33 Data regarding OF pathways for PCNL for patients on chronic narcotics have not been well documented in the literature.
Opioid-sparing pathways in percutaneous nephrolithotomy
In contrast to ureteroscopy, there are more limited published ERAS protocols for opioid-sparing or eliminating pathways after percutaneous nephrolithotomy (Table 4). 47,48 Similar to OF ureteroscopy, key components of ERAS pathways for PCNL include preoperative counseling on expectations, perioperative NSAIDs, and postoperative protocols based on the combination of NSAIDs and acetaminophen with targeted interventions for stent discomfort. A summary of published studies concerning ERAS pathways in PCNL can be found in Table 4.
Published Studies on Efficacy of Enhanced Recovery After Surgery Pathways After Percutaneous Nephrolithotomy
MME = morphine milligram equivalents; WISQOL = Wisconsin Stone Quality of Life Questionnaire.
Pre- and perioperative components of opioid-sparing pathways in percutaneous nephrolithotomy
Preoperative ERAS components for PCNL are overall similar to OF ureteroscopy. In their 2022 study, Girgiss et al. describe the use of tamsulosin 0.4 mg daily for 7 days preoperatively as well as acetaminophen and gabapentin before surgery (Table 5). 47 Similar to most published OF ureteroscopy pathways, they also utilized ketorolac 15 to 30 mg IV intraoperatively and limited opioids in the recovery room to as low doses as possible. 47 A recent RCT by Ucar et al. found IV ibuprofen given before PCNL completion is associated with reduced need for IV narcotics with 24-hour postoperative compared with those receiving IV acetaminophen. 49 Given the lack of a placebo group, the impact of this trial may be limited.
Components of Published Percutaneous Nephrolithotomy Enhanced Recovery After Surgery Pathways Organized by Phase of Care
Specific intervention of PO or IV non-narcotic analgesics before procedure. This includes APAP, gabapentin, NSAIDs.
OR = odds ratio; PACU = Post-Anesthesia Care Unit; PNBs = peripheral nerve blocks.
Specific to PCNL, the addition of targeted peripheral nerve blocks (PNBs) has been demonstrated to significantly reduce opioid use intraoperatively and during early postoperative recovery. 50 The specifics of each of these blocks is beyond the scope of review, but an overview of the role of PNBs as an opioid-sparing agent in ERAS protocols is included. In a 2022 systematic review, Winoker et al. evaluated 17 trials inclusive of 5 different blocks utilized for PCNL—paravertebral, intercostal, quadratus lumborum, transversus abdominus, and erector spinae. 50 Because of variability in reported outcomes, a pooled meta-analysis could not be performed.
However, the majority of studies included for paravertebral, erector spinae, and quadtratus lumborum all showed lower pain scores and decreased need for opioids in the first 24-hours postoperatively. 50 In the first published study on ERAS pathways and PCNL, Li et al. described the use of PNBs or epidural anesthesia intraoperatively. 48 Collectively, this highlights a role for PNBs as an intraoperative adjunct to reduce need for opioid analgesia. However, PNBs carry their own risks, require specialty expertise, and provide unclear benefit in terms of risks for long-term or postdischarge opioid use.
Postoperative opioid-sparing pathways in percutaneous nephrolithotomy
There are two available published ERAS protocols for PCNL, with postoperative management focusing on NSAIDs. In their 2020 study, Li et al. utilized IV and PO NSAIDs at set time points postoperatively to control pain but did not specifically measure or document postoperative opioid use. 48 In contrast, Girgiss et al. based their ERAS protocol based on OF ureteroscopy pathways with the addition of a standing prescription for PO oxycodone (#7) for breakthrough pain only. 47
A direct comparison with a historical pre-ERAS cohort showed reduction in total narcotic usage (116.13 OME vs 39.57 OME, p < 0.001) inclusive of both intra- and postoperative use. 47 Although improved quality of life and diminished pain interference were seen in the ERAS groups by 8 weeks postoperatively, direct comparisons with the historical pre-ERAS group were not performed. 47 This study is the first to demonstrate significant reduction in post-PCNL opioid use through introduction of a protocolized multimodal pain regimen.
Future trials should aim to directly compare pain scores, opioid use, and quality of life metrics between ERAS and non-ERAS groups to evaluate these protocols more effectively. It is also worth noting that existing ERAS protocols for PCNL have numerous interventions aimed specifically at addressing stent discomfort. In the setting of efforts to pursue mini and tubeless approaches to PCNL, the composition of optimal pain management strategies will likely shift.
Discussion
In this narrative review, we report on opioid-sparing and eliminating pathways in stone disease pain management. Published protocols aimed at reducing opioid use have been described across the spectrum of disease from presentation with acute renal colic to postoperative management of pain after ureteroscopy and PCNL. The overwhelming majority of literature available demonstrates that nonopioid analgesics provide comparable to superior pain control compared with opioids in both acute renal colic and in a postoperative setting.
Introduction of OF pathways in management of acute renal colic and ERAS protocols after ureteroscopy have also found high rates of success with low rates of need for rescue opioid prescriptions. Given known risks associated with even short courses of opioids, need for expansion and optimization of OF and opioid minimizing protocols is essential.
Acute renal colic is a common reason for emergency room presentation and also serves as a potential exposure to opioids, which can have a lasting negative impact. Given increased odds of persistent narcotic use associated with recurrent stone episodes, there is a need to reduce opioid exposure in an emergency room setting. 51 As highlighted by a 2004 Cochrane Review and bolstered by a recent meta-analysis, NSAIDs are associated with slightly superior improvement in VAS pain scores, reduced need for rescue medication, and decreased episodes of emesis compared with opioids in emergency management of acute renal colic. 16,17
IV acetaminophen is a viable option for acute renal colic, with similar to improved pain control outcomes compared with IV opioids. 17 MET with tamsulosin also provides significant measurable benefit in terms of pain control and need for rescue analgesia, especially for kidney stones measuring 5 to 10 mm. Other adjuncts for pain management, including IV desmopressin, IV magnesium, and anticholinergics, have not shown consistent benefit in the literature.
Reduction of both in-hospital and postdischarge opioid use through increased utilization of NSAIDs and multimodals has been pursued with success. 19,20 Despite this, specific OF postemergency discharge pathways for acute renal colic are not well described in the literature, and warrant further study.
Perioperative pain management in kidney stone disease has evolved significantly over the past decade, with several studies describing OF ureteroscopy being published in the past 5 years. With RCT data showing NSAIDs given intraoperatively and postoperatively can significantly reduce the need for narcotic analgesia after surgery, multiple OF pathways have been described with failure rates under 20% (Table 1).
A key component of many of these pathways is inclusion of medications for stent discomfort, including tamsulosin, phenazopyridine, and anticholinergics (Table 2). Although different combinations of medications have been trialed, direct head-to-head comparisons have not been performed, so it is difficult to isolate the contribution of different components of ERAS protocols to the overall success of these pathways. Although literature specifically regarding ERAS pathways for PCNL is more limited, pathways utilizing similar protocols to OF ureteroscopy have been described. 47
Multiple PNBs have also been studied in this space and have been shown by the majority of studies to reduce the need for postoperative opioids in the immediate postoperative period. 50 Further investigation is needed, particularly regarding the impact of integration of PNBs into ERAS pathways.
We acknowledge limitations of this review including narrative design and use of a single database for literature search. In addition, synthesis of available data is limited by variability in reported outcomes between studies. For instance, although many studies utilize VAS for assessment of patient pain levels, different scales (100-point vs 10-point) are used. Furthermore, the clinical significance of small differences in VAS-reported pain scores remains unclear. 16,50
Furthermore, many of the studies utilizing pain scores as a primary outcome measure only assess these variables for a short period of time (i.e., out to 48 hours postprocedure or during an ER presentation only), limiting our understanding of long-term pain control or differences in opioid dependence. Finally, many of the included studies utilizing NSAIDs excluded patients with renal dysfunction or prior opioid dependence, limiting the applicability of these pathways to these groups. It is worth noting that short courses of NSAIDs can be safely prescribed for patients with CKD 1 and 2 (Table 3). 43
Conclusions
Opioid-sparing protocols have been shown to reduce or eliminate the need for opioid analgesics in the setting of acute renal colic and after surgery for kidney stones. Specific to ureteroscopy, completely OF protocols centered on NSAIDs and medications to address stent discomfort have been shown to eliminate postoperative opioid use in >80% of patients. Although the direct contribution of each medication to overall pain control is difficult to assess, most published protocols have utilized alpha-blockers, anticholinergics, and acetaminophen in addition to NSAIDs (Table 3). In PCNL, ERAS pathways are similarly constructed, with emerging application of PNBs showing at least short-term reductions in opioid use.
Footnotes
Authors' Contributions
Article review, writing, and editing by J.J.S.C. and N.L.M.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.