
Abstract
Introduction:
Percutaneous microwave ablation (MWA) has emerged as a new energy modality for percutaneous renal tumor ablation with potential advantages over radiofrequency and cryoablation. The goal of our study was to determine MWA outcomes for suspicious renal masses, with a subset analysis for biopsy-proven renal cell carcinoma (RCC) and larger (T1b) tumors.
Methods:
Studies reporting outcomes of MWA for RCC were identified. Random-effects models with inverse-variance weighting were used to pool outcomes, including technical success rate (TSR), technical efficacy rate (TER), local recurrence rate (LRR), cancer-specific survival rate (CSSR), overall survival rate (OSR), and complications.
Results:
Among 914 studies captured, 27 studies with 1584 patients (1683 malignant renal tumors) were included. The pooled TSR and TER were 99.6% (95% confidence interval [CI], 98.0%–100%) and 96.2% (95% CI, 93.8%–98.2%). The pooled LRR was 3.2% (95% CI, 1.9%–4.7%). At 1, 3, and 5 years, the pooled CSSRs were 100% (95% CI, 99.4%–100%), 100% (95% CI, 98.4%–100%), and 97.7% (95% CI, 94.5%–99.7%), while pooled OSRs were 99.0% (95% CI, 97.5%–99.9%), 96.0% (95% CI, 93.1%–98.3%), and 88.1% (95% CI, 80.3%–94.2%). The pooled minor and major complication rates were 10.3% (95% CI, 7.1%–13.9%) and 1.0% (95% CI, 0.3%–2.1%). In 204 patients with 208 T1b tumors, the pooled TSR and TER were 100% (95% CI, 96.6%–100%) and 85.2% (95% CI, 71.0%–95.8%). The pooled LRR was 4.2% (95% CI, 0.9%–8.9%). At 1, 3, and 5 years, the pooled CSSRs were 98.2% (95% CI, 88.7%–100%), 97.2% (95% CI, 78.5%–100%), and 98.1% (95% CI, 72.3%–100%). At 1 and 3 years, the pooled OSRs were 94.3% (95% CI, 85.7%–99.6%) and 89.3% (95% CI, 68.7%–100%). The pooled minor and major complication rates were 14.8% (95% CI, 7.4%–23.8%) and 2.6% (95% CI, 0%–7.8%).
Conclusions:
MWA demonstrated favorable short- to intermediate-term oncologic outcomes with low complication rates, including in the T1b subset, with moderate quality of data and heterogeneity of assessed outcomes. This supports MWA as a safe and effective treatment for RCC and a potential viable option for larger tumors.
Introduction
Worldwide, renal cell carcinoma (RCC) is the 6th most common cancer in men and 10th in women, with steadily increasing incidence and mortality rates. 1 According to the World Health Organization, there are more than 140,000 RCC-related deaths yearly, ranking it as the 13th most common cause of cancer death globally. 1 With smaller RCCs, the gold standard for treatment is surgical excision by partial nephrectomy (PN). However, recent studies have suggested significant heterogeneity among small renal masses, with ∼20% being benign, 60% being indolent variants of RCC, and 20% being potentially aggressive tumors. 2 In a meta-analysis of 286 RCC patients with a median age of 73 years, the average growth rate of tumors was 0.28 cm per year, and only 1% of all lesions metastasized. 3 The natural history of small kidney tumors suggest a need for less-aggressive management in select patients who cannot undergo surgery due to high risk of postoperative morbidity and mortality and in patients seeking a truly minimally invasive approach with faster recovery and lower risk for complication. 4
In the past decade, percutaneous image-guided thermal ablation of T1a RCCs (<4 cm) has gained considerable traction. 5 Percutaneous image-guided thermal ablation works by exposing smaller tumors to the extremes of temperatures without the need for surgery. The most common modalities include radiofrequency ablation (RFA), which induces tissue hyperthermia and cell death, and cryoablation, which causes cell death through osmotic dehydration of cells and formation of intracellular ice. 2,4,6 Both have been associated with cancer-specific survival rates (CSSRs) of >90%, similar to that of PN, but with reduced operative time, length of hospital stay, general surgical risks, and sparing of postoperative renal function and reduced risk of chronic kidney disease. 4,6
Comparatively, microwave ablation (MWA), which has a similar mechanism of action to RFA, was introduced in the late 2000s for T1a renal tumor ablation. 7 It offers several advantages to the existing ablative techniques. Compared with RFA, MWA can reach higher intratumoral temperatures and achieve larger ablation zones because it is not dependent on electrical conductivity of tissue, but rather, relies on heating tissue by creating an electromagnetic field. 4 –8 As a result, MWA is not impacted by tissue carbonization that would prevent the effect of its energy diffusion. Compared with cryoablation, MWA has much shorter ablation times and is technically simpler to perform as it requires only one probe to be inserted. However, compared with RFA and cryoablation, the evidence surrounding MWA use in RCCs is not as well established. A recent meta-analysis in 2018 included 13 studies published between 2013 and 2017 and 567 RCC patients with 616 malignant RCCs undergoing MWA, which serves as the largest MWA review to date. 9 As of 2022, there have been numerous studies with larger MWA cohorts, longer follow-up periods, and evidence regarding the use of MWA in larger malignant renal tumors (>4 cm).
As such, we believe that a pooled analysis of studies published to date is necessary to better understand the safety and efficacy of MWA in the management of malignant renal tumors and subsequently provide RCC patients with another evidence-based option. Thus, the objective of this study was to determine the treatment outcomes of MWA in patients with malignant renal tumors, with a secondary goal of determining the treatment outcomes of MWA in T1b (4–7 cm) renal tumors.
Materials and Methods
This study was conducted with adherence to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines and was prospectively published on Open Science Framework registries (
Study identification
A comprehensive search of Medline, Embase, and Scopus up to July 21, 2022, was conducted. The search strategy was designed with the help of a medical librarian to capture all studies related to the use of MWA in patients with malignant renal tumors (Supplementary Appendix SA1).
Inclusion criteria
Following the Population, Intervention, Control, and Outcomes (PICOS) framework:
Exclusion criteria
The exclusion criteria were case reports, review articles, editorials, letters, comments, and conference abstracts/proceedings, studies with overlapping patients, and data. We also limited the search to English-only publications.
Data synthesis
Two independent reviewers screened (title and abstract, full-text) and extracted the identified studies within the search parameters. A pilot screening assessment was performed on 10 studies to ensure agreement between reviewers. Results were collected through the Covidence software for systematic reviews (Veritas Health Innovation Ltd.) and Microsoft Excel (Microsoft, Redmond, WA, USA). In the case of discrepancies between reviewers in screening or data collection, a joint discussion took place to resolve conflicts between the two reviewers and the senior author. If any of the inclusion criteria were unclear based on the abstract alone, the study was included for full-text review.
Data extraction
The relevant baseline characteristics to be extracted from the final list of included studies were study characteristics (authors, year of publication, country of origin, journal of publication, and study design), patient characteristics (age, sex, number of T1a/T1b patients, and follow-up duration), and tumor characteristics (tumor histology, number of lesions, and tumor size). The outcomes extracted for analysis included technical outcomes (technical success rate [TSR] and technical efficacy rate [TER]), oncologic outcomes (local recurrence rate [LRR], CSSR, and overall survival rate [OSR]), and complications following MWA treatment. Technical success was defined as correct positioning of the antenna inside the target lesion and subsequent complete ablation, as identified on imaging immediately following MWA. 6 Technical effectiveness was defined as the absence of residual tumor on imaging (CT or MRI), based on the absence of enhancement, at 1 month after MWA treatment. 9 Local recurrence was defined as the presence of recurrent tumor on imaging (CT or MRI), based on the presence of enhancement, at the specific reported time point for patient follow-up after MWA treatment.
CSSR and OSR were reported at 1, 3, and 5 years, when available. Complications were subdivided as major or minor complications according to the Society of Interventional Radiology classifications, as this is how most studies reported this metric. 11
These outcomes were extracted for three patient cohorts: the complete study cohort (all included patients and tumors), the T1b cohort (patients with only T1b tumors), and the biopsy-proven cohort (patients who have biopsy proven RCC). The quality of nonrandomized studies was assessed using the Newcastle–Ottawa Scale (NOS). 12 It judges studies based on three broad aspects: the selection of study groups, comparability of groups, and the ascertainment of either the exposure for case–control studies or outcome for cohort studies, with a maximum score of 9. NOS scores of 7 to 9 were deemed as high quality, 4 to 6 as moderate quality, and 0 to 3 as low quality. All data and quality assessment were extracted and conducted independently by two reviewers, and discrepancies were resolved through a consensus discussion with the senior author.
Statistical analysis
Technical, oncologic, and complication outcomes were pooled for the complete study cohort, the T1b subset, and the biopsy-proven subset using random effects models with the inverse-variance weighting-method and Clopper–Pearson confidence intervals (CIs). The restricted maximum likelihood estimate for tau squared was used. Study heterogeneity was assessed using the Cochrane Q-test and Higgins I 2 statistics. An I 2 value of 0% to 25% was interpreted as minimal heterogeneity, 25% to 50% as low heterogeneity, 50% to 75% as moderate heterogeneity, and 75% to 100% as high heterogeneity. A p-value of <0.10 on Cochrane Q-test was used to indicate substantial heterogeneity. Egger's test was used to formally evaluate publication bias for outcomes with 10 or more studies.
Results
Search results
From a database search of 914 studies, 27 articles involving 1584 patients and 1683 suspicious renal tumors were included for analysis (Supplementary Appendix SA2). Figure 1 details the screening process and reasons for exclusion at full-text screening. Of the included studies, 10 reported on outcomes for T1b patients, resulting in a subset cohort of 204 patients and 208 tumors for analysis. As for the biopsy-proven cohort, 20 studies were included with 1191 patients and 1286 malignant renal tumors. A detailed breakdown of study, patient, and tumor characteristics can be found in Table 1.
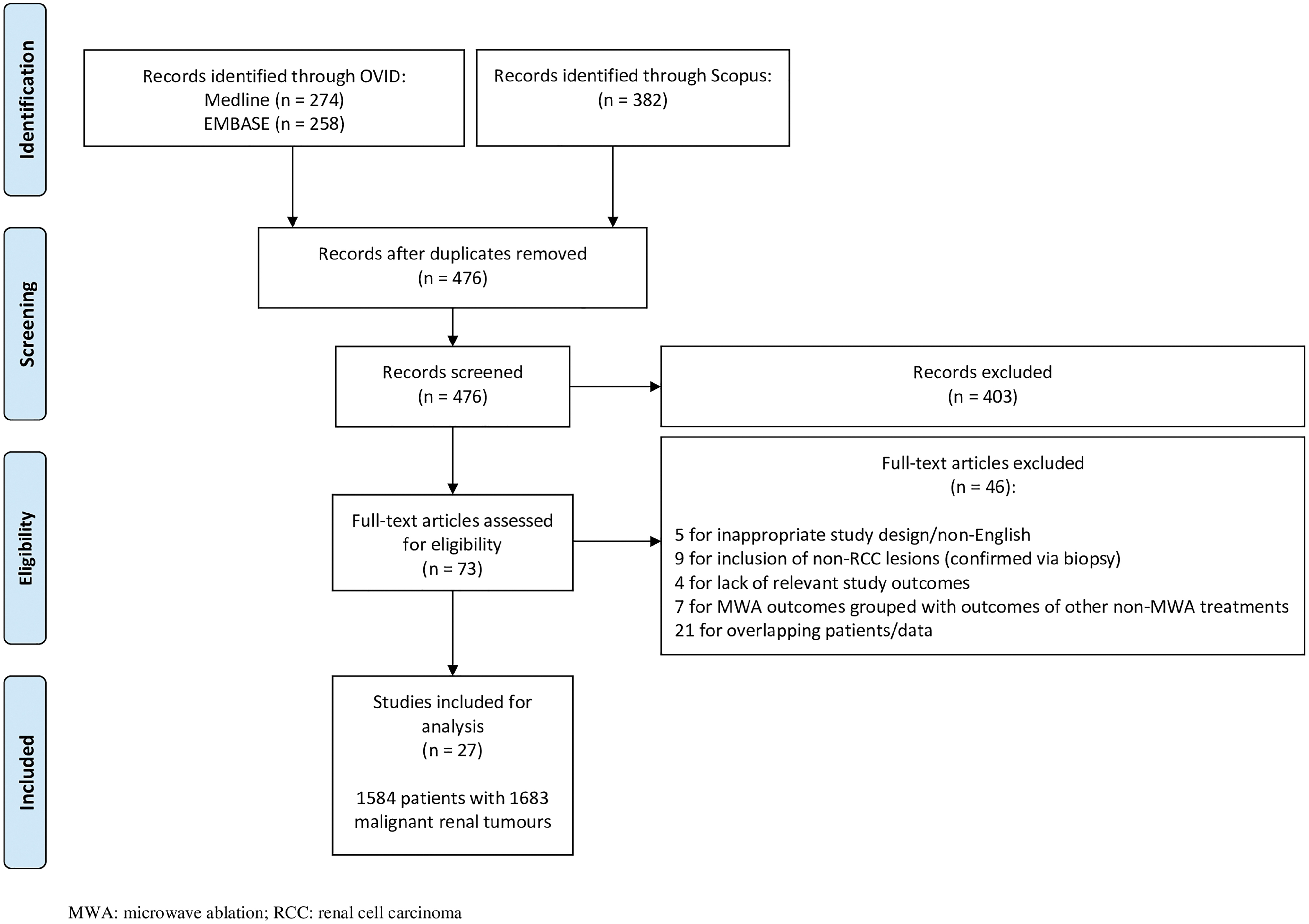
Preferred Reporting Items for Systematic Reviews and Meta-analyses diagram.
Characteristics of Included Studies
F = female; IQR = interquartile range; M = male; NOS = Newcastle–Ottawa Scale; NR = not reported; US = ultrasound.
Complete study cohort analyses
The pooled TSR and TER were 99.6% (95% CI, 98.0%–100%; I 2 = 51%) and 96.2% (95% CI, 93.8%–98.2%; I 2 = 66%). The pooled LRR was 3.2% (95% CI, 1.9%–4.7%; I 2 = 11%) over a median follow-up duration of 19.5 months. At 1, 3, and 5 years, the pooled CSSRs were 100% (95% CI, 99.4%–100%; I 2 = 0%), 100% (95% CI, 98.4%–100%; I 2 = 64%), and 97.7% (95% CI, 94.5%–99.7%; I 2 = 48%), while pooled OSRs were 99.0% (95% CI, 97.5%–99.9%; I 2 = 19%), 96.0% (95% CI, 93.1%–98.3%; I 2 = 12%), and 88.1% (95% CI, 80.3%–94.2%; I 2 = 64%). The pooled minor and major complication rates were 10.3% (95% CI, 7.1%–13.9%; I 2 = 78%) and 1.0% (95% CI, 0.3%–2.1%; I 2 = 21%). A list of complications can be found in Table 2. Substantial heterogeneity was noted for TSR, TER, 3-year CSSR, 5-year OSR, and minor complications. Forest plots for the complete cohort outcomes can be found in Figure 2.
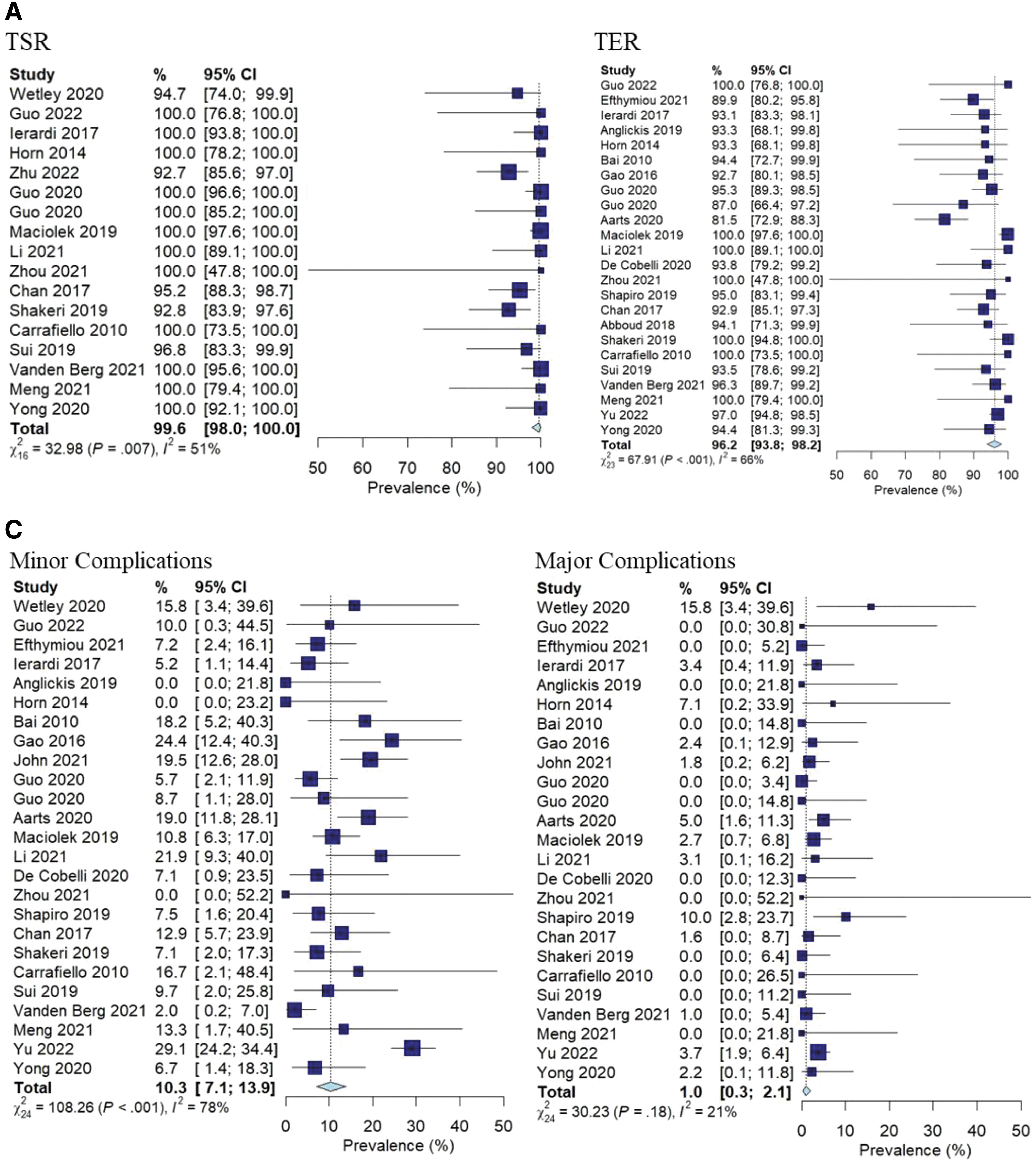
Meta-analytic summary of outcomes for the complete study cohort.

Summary of Microwave Ablation Complications
ICU = intensive care unit; IV = intravenous; MI = myocardial infarction; PCI = percutaneous coronary intervention; PE = pulmonary embolism; pRBC = packed Red Blood Cells; UPJ = ureteropelvic junction.
T1b subgroup analyses
The pooled TSR and TER were 100% (95% CI, 96.6%–100%; I 2 = 0%) and 85.2% (95% CI, 71.0%–95.8%; I 2 = 71%). The pooled LRR was 4.2% (95% CI, 0.9%–8.9%; I 2 = 21%) over a median follow-up duration of 26.5 months. At 1, 3, and 5 years, the pooled CSSRs were 98.2% (95% CI, 88.7%–100%; I 2 = 63%), 97.2% (95% CI, 78.5%–100%; I 2 = 77%), and 98.1% (95% CI, 72.3%–100%; I 2 = 70%). At 1 and 3 years, the pooled OSRs were 94.3% (95% CI, 85.7%–99.6%; I 2 = 0%) and 89.3% (95% CI, 68.7%–100%; I 2 = 0%). A pooled 5-year OSR was not available for the T1b cohort due to lack of studies reporting this outcome. The pooled minor and major complication rates were 14.8% (95% CI, 7.4%–23.8%; I 2 = 41%) and 2.6% (95% CI, 0%–7.8%; I 2 = 13%). Substantial heterogeneity was noted for TER, 3-year CSSR, and 5-year CSSR. Forest plots for T1b outcomes can be found in Figure 3.
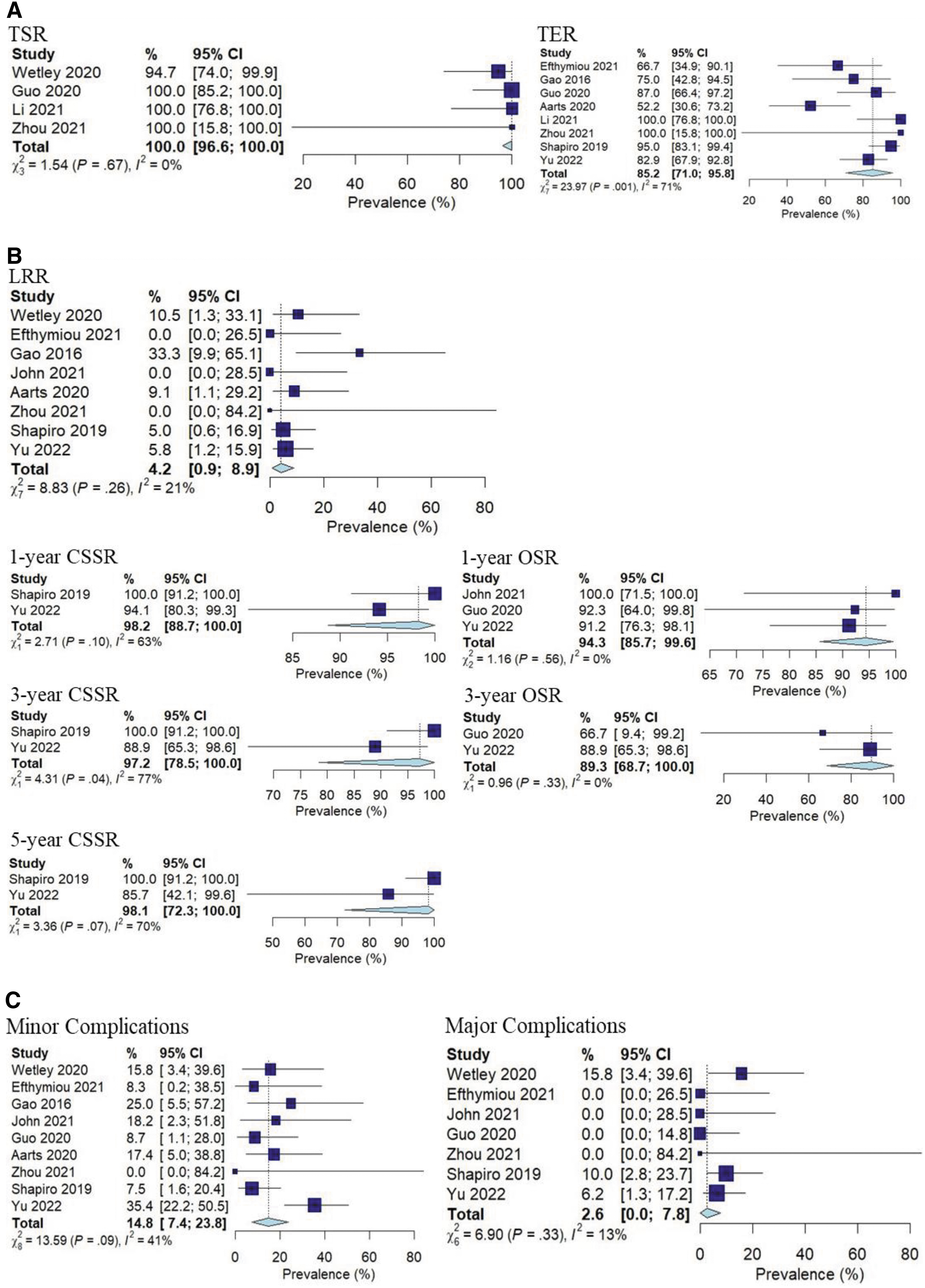
Meta-analytic summary of outcomes for the T1b population.
Biopsy-proven subgroup analyses
The pooled TSR and TER were 99.2% (95% CI, 96.8%–100%; I 2 = 56%) and 96.7% (95% CI, 93.6%–99.0%; I 2 = 73%). The pooled LRR was 3.7% (95% CI, 2.2%–5.6%; I 2 = 4%) over a median follow-up duration of 20.1 months. At 1, 3, and 5 years, the pooled CSSRs were 100% (95% CI, 99.3%–100%; I 2 = 0%), 99.4% (95% CI, 97.2%–100%; I 2 = 69%), and 98.0% (95% CI, 93.8%–100%; I 2 = 60%), while pooled OSRs were 98.5% (95% CI, 96.9%–99.6%; I 2 = 0%), 96.1% (95% CI, 93.4%–98.2%; I 2 = 13%), and 90.1% (95% CI, 81.7%–96.3%; I 2 = 63%). The pooled minor and major complication rates were 11.8% (95% CI, 8.0%–16.1%; I 2 = 74%) and 0.8% (95% CI, 0.0%–2.3%; I 2 = 34%). Substantial heterogeneity was noted for TSR, TER, 3-year CSSR, 5-year CSSR, and 5-year OSR. Forest plots for biopsy-proven outcomes can be found in Figure 4.

Meta-analytic summary of outcomes for the biopsy-proven population.

Study quality assessment
The average NOS score was 5.22, with 5 high-quality studies, 21 moderate-quality studies, and 1 low-quality study. NOS score for each individual study can be found in Table 1. As most studies did not include a comparator group with MWA, we could not formally evaluate the questions regarding selection of a nonexposed cohort and comparability of cohorts, resulting in 2 points that could not be assigned. The most affected domain was the outcome domain, due to inadequate follow-up durations, significant loss-to-follow-up, or lack of reporting on whether all patients were accounted for during the follow-up period.
Publication bias
No significant publication bias was identified for the assessed outcomes. Funnel plots can be found in Supplementary Appendices SA3 to SA5.
Discussion
This study demonstrates the efficacy and safety of MWA for RCC in the largest review to date with a combined cohort of 1584 patients with 1683 suspicious renal tumors. Before this, the largest meta-analysis performed was in 2018 with a cohort of 567 patients with 616 suspicious renal masses. 9 Since then, 21 additional studies have been published with almost triple the number of patients and tumors for analysis. We were able to demonstrate similar technical outcomes (TSR 99.6% vs 97.3%, TER 96.2% vs 97.6%). More recently published studies have longer follow-up durations with analysis of 3- and 5-year survival rates, allowing for a more accurate analysis of mid and long-term oncologic outcomes in this present study. Comparatively, we included 8 studies for 3-year CSSR vs 3 studies in the prior review and 9 studies for 3-year OSR vs 4 previously. Our analysis demonstrated better long-term survival outcomes than identified previously (3-year CSSR 100% vs 97.6%, 5-year CSSR 97.7% vs 96.9%, 3-year OSR 96.0% vs 86.7%, 5-year OSR 88.1% vs 81.9%), further reinforcing the viability of MWA for long-term disease control.
However, LRR was found to be higher (3.2% vs 2.1%), which may be attributed to the longer follow-up in allowing for recurring events. There remains a concern with currently available literature for inadequate follow-up durations for assessment of LRR, as 3 studies did not report their median/mean follow-up duration and 16 studies had median/mean follow-up durations of less than 2 years. With the inclusion of a biopsy-proven cohort, oncologic outcomes can be more accurately assessed with the exclusion of benign or indeterminate tumors. Our analysis also showed a lower incidence of complications (minor 10.3% vs 17%, major 1.0% vs 1.8%). The improved survival and lower complication rates may be a result of better patient selection over time, improved technique, including better use of hydrodissection, to move adjacent organs out of harm's way, and pyeloperfusion for collecting system protection, as well as technological advances with gas-cooled microwave antennas that permit higher amounts of power with reduced risk of applicator migration to healthy tissue. 13 –15
With the limited evidence available for MWA, RFA and cryoablation are much more commonly used in clinical practice for RCCs. Previous meta-analyses found a TSR of 95.5%, risk of recurrence of 4.1% to 6.4%, and risk of major complications of 3.1% to 3.7% for RFA. 16 –19 Similarly, for cryoablation, the estimated TSR was 92.6%, LRR of 3.0% to 8.5%, and risk of major complications of 1.8%. 20 –22 In our present study, MWA showed promising results, with a TSR of 99.6%, LRR of 3.2%, and major complication risk of 1.0%. Even within the biopsy-proven RCC cohort, the LRR was 3.7%. Although direct comparisons cannot be made between the ablative modalities due to lack of available randomized controlled trials or prospective studies with matched cohorts, our analysis suggests that MWA may be a suitable alternative ablative modality in the treatment of RCC, with the need for further comparisons to confirm this finding.
Despite the growing popularity of ablative therapies for RCC, surgery and PN remains the gold standard treatment based on several guidelines. 23,24 Based on existing meta-analyses, the risk of recurrence following PN is cited to range between 3.3% and 3.8%, while Yanagisawa et al. looked at 9185 T1a patients undergoing PN and found a CSSR of 98.7%. 16,25,26 However, as with most surgical approaches, there is an increased incidence of major complications following PN of ∼4% to 5% that can often be distressing and even life threatening to patients. 18,25,26 In select patients, ablative therapies, such as MWA, can be an attracting alternative, as they can provide similar oncologic outcomes, but with lower risk of postoperative major complications, reduced length of stay, and shorter recovery time.
The present study is the first to synthesize clinical outcomes of MWA for T1b RCC patients. Controversy regarding the use of MWA and ablative therapy, in general, may be perceived to increase the risk of recurrence for such large tumors, along with a lower survival rate compared with PN as demonstrated by a network meta-analysis in 2019. 27 In 204 patients with 208 T1b tumors, we found good technical, oncologic, and safety outcomes following MWA. A meta-analysis by Yanagisawa et al. looked at PN for T1b RCC patients. 26 They found a recurrence rate of 7.8% (411 patients), a CSSR of 95.9% (444 patients), and a 3.1% incidence of major complications (196 patients). With MWA, we found a recurrence rate of 4.2% (170 patients), 3-year CSSR of 97.2% (58 patients), and 2.6% incidence of major complications (155 patients). This is further supported by a comprehensive meta-analysis by Chan et al., who found similar long-term oncologic outcomes between ablative therapy and PN but lower rates of complications following ablation without any major, significant, or unexplainable heterogeneity in their analysis. 28 Despite the promising results, most of our survival data were extracted from a few studies with small T1b populations.
Additionally, these oncologic outcomes may be falsely inflated by the inclusion of benign tumors, as some studies did not clearly report outcomes for pathologically confirmed T1b RCC. Nonetheless, this preliminary evidence suggests that MWA may be offered safely in select nonsurgical candidates for T1b RCCs with effective short-term disease control and low risk of recurrence. However, further research needs to be conducted to confirm the durability of MWA with regard to long-term survival for T1b RCC patients.
This study has several limitations. First, all included studies were retrospective in nature, which are often fraught with biases intrinsic to their design, specifically risk for selection bias on who undergoes intervention and risk for underreporting of complications. However, randomization of surgical interventions is often difficult and may even be considered unethical, given the numerous considerations that may lead to differing outcomes with each intervention offered. We urge future research to at least be conducted prospectively. Second, with regard to the entire cohort analysis, tumors with high suspicion of being RCC (e.g., tumors with nondiagnostic biopsy results, Bosniak IV cystic lesions) were included despite lack of biopsy confirmation, as these tumors may be ablated in clinical practice without definitive confirmation. This may lead to an overestimation of the oncologic benefits of MWA, as benign lesions have limited risk of recurrence and similarly should not have an impact on CSSR and OSR. However, this limitation was addressed through a subset analysis of a biopsy-proven cohort to provide more accurate estimates.
Third, there were moderate-to-high levels of heterogeneity for many of the assessed outcomes, despite using standardized definitions for most outcomes. For minor complications, this may be due to inconsistent definitions used by different studies. For example, some studies included pain, vomiting, and mild flank or abdominal pain as minor complications, while others only reported it as a complication if these symptoms required medications or further investigation. Otherwise, heterogeneity was mitigated using random-effects models to pool results. As well, the certainty of evidence was not formally appraised in this review, although given the poor adherence to the outcome domain of the NOS and the moderate-to-high levels of heterogeneity for many outcomes, the certainty of evidence is estimated to be low to moderate.
Lastly, as mentioned above, studies assessing MWA in T1b patients often consisted of smaller populations with limited follow-up for long-term oncologic outcomes. Nonetheless, the conclusions drawn regarding complications and technical outcomes can still be applicable in guiding management of T1b tumors.
Future research should be conducted with greater methodological rigor, particularly through prospectively collected data with matched comparisons between different ablative modalities or between MWA and PN, specifically for T1b patients.
Conclusion
MWA demonstrated favorable technical and short- to intermediate-term oncologic outcomes with a low incidence of complications in 1584 patients with 1683 renal tumors, including in the T1b subset of 204 patients and 208 tumors. However, the majority of the included studies were of moderate quality, with considerable to substantial levels of heterogeneity for many of the assessed outcomes in the complete study cohort and the subset analyses. Further high-quality research needs to be conducted to better characterize long-term oncologic outcomes following MWA, especially for T1b tumors.
Footnotes
Acknowledgment
This abstract was previously published and presented as a conference poster at the Canadian Urological Association (2023) annual meeting in Montreal, Canada on Saturday, June 24, 2023 (doi: 10.5489/cuaj.8413).
Authors' Contributions
J.W.: Conceptualization, methodology, investigation, data curation, writing––original draft, writing––review and editing, and visualization. S.S.: Methodology, investigation, data curation, and writing––review and editing. K.L.: Methodology and formal analysis. T.K.: Methodology and data curation. M.O.: Conceptualization, methodology, writing––review and editing, supervision, and project administration.
Author Disclosure Statement
There are no conflicts of interest or financial disclosures for any authors.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
Supplementary Appendix S3
Supplementary Appendix S4
Supplementary Appendix S5
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.