
Abstract
Background:
Recently a novel omnidirectional (OD) ureteral access sheath (UAS) has been developed. By retrospectively reviewing and comparing the flexible ureteroscopic lithotripsy (FURL) cases in our institution with either a conventional Cook UAS or an OD UAS in the past year, we shared our experience of the safety, efficacy, and relevant issues on the usage of OD UAS.
Materials and Methods:
The medical history and surgery details of 199 patients with kidney stones or ureterojunctional stones who underwent FURL in Xinhua Hospital, including 61 Cook UAS and 138 OD UAS, were reviewed and compared. The maximal deflection angle was measured by steering four different types of ureteroscopes to bend the OD UAS in different states.
Result:
The deflection angle of OD UAS was ∼110° to 130° free load, and 90° to 130° when loaded with different instruments. The stone burden and position were similar in two groups. Given a similar prestent ratio and operation time, the OD UAS group achieved a higher single-session stone-free rate (SFR) (63.9% vs 94.2%, p < 0.0001) at 1-month follow-up evaluated by a CT scan.
Conclusion:
OD UAS is a novel flexible UAS with a suction port, able to enter calyxes, improve stone-free rate, and reduce surgery time. The unique flexible design allows it to bend with the ureteroscope and enter renal calices and be set close to the stone. Combined with the suction port, OD UAS contributes greatly to dealing with large-burden kidney stones, shortens operation time, and improves single-session SFR.
Introduction
The ureteral access sheath (UAS), first developed in 1974 by Hisao Takayasu and Yoshio Aso, facilitates the insertion of the ureteroscope into the ureter. 1 UAS possesses several other merits, such as lowering the intrapelvic pressure, protecting the ureteroscope, and protecting the ureter when extracting stone fragments. 2 However, the process of extracting stone fragments could be lengthy, tiring, and tiresome. Sometimes larger fragments might get stuck at the tip of the UAS and demand further laser fragmentation. If the stone is fragmented into smaller pieces, yet not to the extent of stone dusting, the large number of small fragments might need to be repeatedly captured by baskets.
Recently a novel omnidirectional (OD) UAS (Yigao Medical Technology, Hangzhou, China), which is a flexible UAS product, has been developed, and we are among the first batch of institutions in China to try this OD UAS. The flexible design allows it to bend with the ureteroscope and enter renal calices and be set close to the stone. The initial safety and efficacy data are reported in this retrospective study, and hence our experience is shared here.
Materials and Methods
Patients
The medical information of patients with kidney stones or ureteropelvic stones who underwent flexible ureteroscopic lithotripsy (FURL) in Xinhua Hospital from June 2022 to May 2023 was fully reviewed. The cases excluded for reasons as follows: (1) UAS was not used because of severe ureteral strictures, (2) those who did not return to our institution for Double-J stent removal and relevant follow-up, and (3) those whose preoperative and postoperative CT scan was not performed in our institution. After review, the data of 199 patients, including 61 who used Cook UAS and 138 who used OD UAS, were calculated, and compared.
Omnidirectional UAS
The primary component of OD UAS (Fig. 1A) is PEBAX® (polyether block amide). The whole sheath is well supported by a metal wire coil to prevent collapse under pressure. The intraluminal channel is coated with Teflon™ (polytetrafluoroethylene) and the outside layer is coated with hydrophilic polyvinylpyrrolidone (Fig. 1B). The suction port largely comprises a nozzle (which connects to vacuum suction), a suction switch, and a watertight valve (Fig. 1C). The entire OD UAS piece is 45 cm long for women (Fig. 1D) or 50 cm for men.
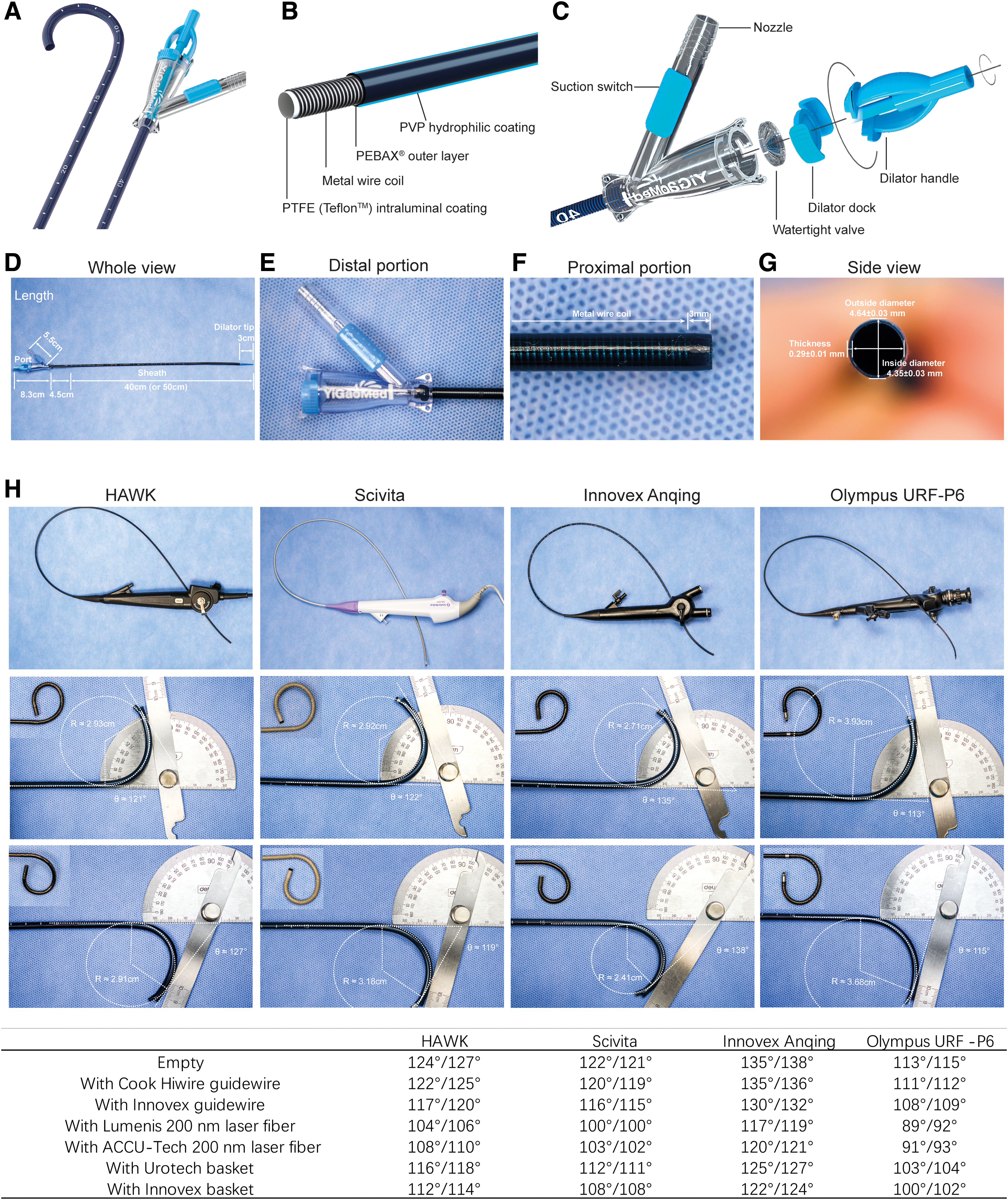
Diagrams and photographs of the structure of the OD UAS.
The suction port (Fig. 1E) is 5.5 cm long. The top 3 mm of the sheath is without a metal wire coil (Fig. 1F) and the tip is soft, and the flexible portion of the sheath is 10 cm long. For a 12F/14F OD UAS, the outside diameter we measured was 4.64 ± 0.03 mm, the inside diameter was 4.35 ± 0.03 mm, and the sheath thickness was 0.29 ± 0.01 mm (Fig. 1G).
Intervention
A noncontrast CT scan was routinely performed to determine the stone's location and size. In all retrograde ureteroscopies, a 0.038-inch (= 0.97 mm) Cook Hiwire hydrophilic guidewire (Cook Medical, Limerick, Ireland) was routinely used. Rigid ureteroscopy lithotripsy (URL) was performed using A Wolf 8F/9.8F rigid ureteroscope (Richard Wolf, Knittlingen, Germany). FURL was performed using four types of flexible ureteroscopes, including three types of digital ureteroscopes: 8.5F HAWK DPG II (MINI TECH, Guangzhou, China), 8.4F Scivita SUC-2A-B (Scivita Medical Technology, Suzhou, China), and 8.7F Innovex Anqing US31B-12 (Innovex, Shanghai, China), and one conventional optic fiber ureteroscope 8.4F Olympus URF-P6 (Olympus Medical System, Tokyo, Japan).
The patients either used a conventional 12F/14F Flexor UAS (Cook Urological, Spencer, IN, USA) or the OD UAS. Conventional UAS was positioned at ureteropelvic junction (UPJ), whereas the OD UAS could be maneuvered into different calices by the ureteroscope (Fig. 2A) to the vicinity of the stones. Lithotripsy was performed using Lumenis Powersuit 60 W holmium laser (Lumenis GmbH, Dieburg, Germany). For the SHREK irrigation pump (Shanghai Shiyin Photoelectric Instrument Co., Ltd., Shanghai, China), the flow was usually set at 1 L/min and the pressure was usually set at 350 mm Hg.
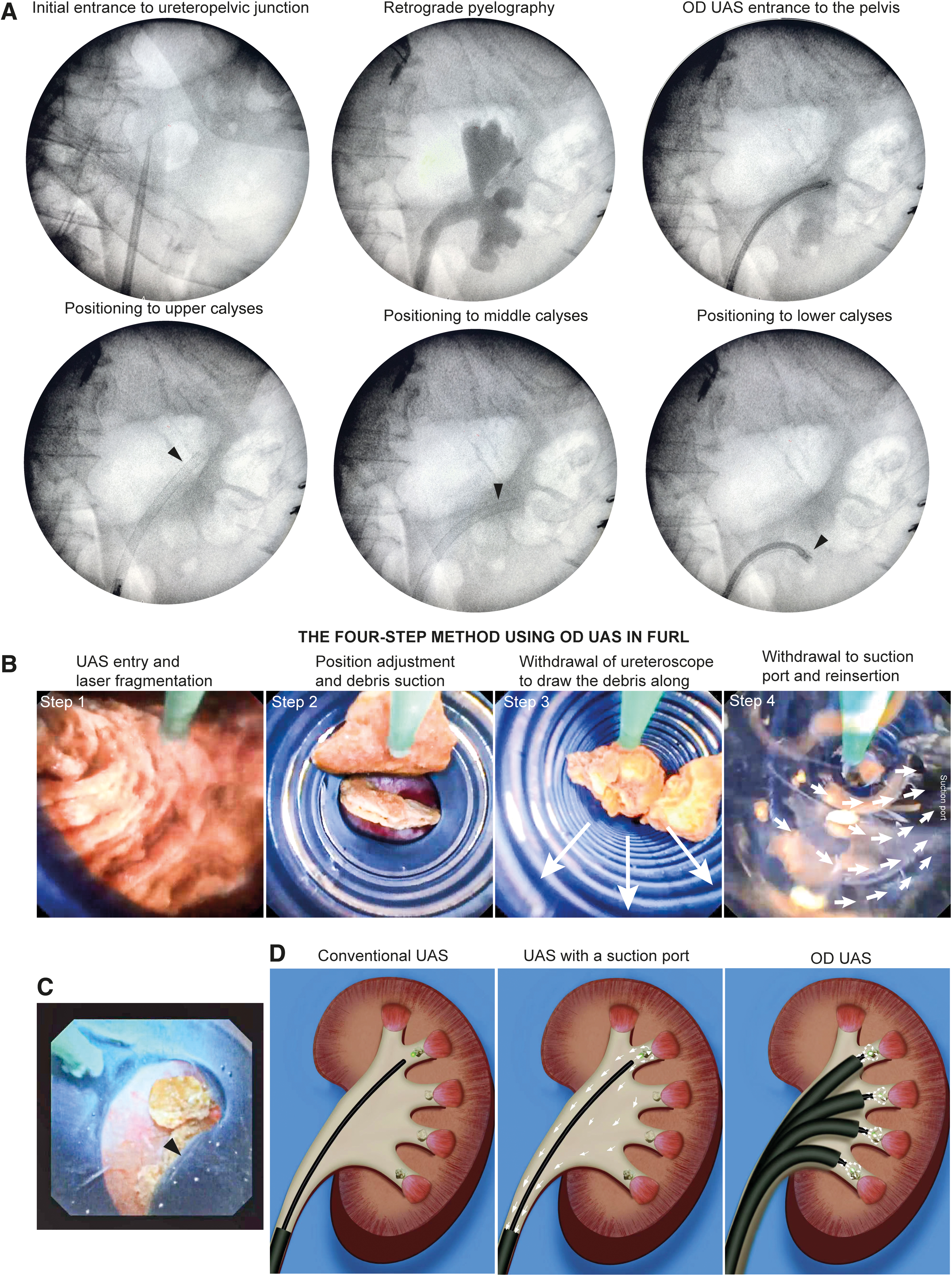
X-ray images and diagram of OD UAS application.
In the OD group, suction was continuously performed, the vacuum suction pressure was set around −25 kPa. The suction intensity could be modulated by tuning the suction switch, from weak to strong. Fragments were removed tuning the suction switch in the OD group. In majority of the time, the suction switch was open so the suction force was weak. When we aimed the OD sheath toward the stone, we turned the switch on and after the stone fragments entered and the switch was tuned gradually down.
In the Cook group, active extraction with an Innovex Nitinol basket (IVX-US-T1110; Innovex) was performed in every patient. After laser lithotripsy, patients received the Braun 5.0F Urecath Double-J stents (Barun Medical S.A.S, Nogent-le-Rotrou, France). An 18F Foley catheter (Bard, Kulim, Malaysia) was placed for urinary drainage postoperatively for 24 hours. All patients took standard perioperative antibiotic prophylaxis (single shot of cefuroxime 1.5 g or levofloxacin 500 mg in cases of allergy) 0.5 to 2 hours before intervention, and a standard medication prescription, primarily cefuroxime and paracetamol for 24 hours. The significance level was set to 5% (p < 0.05) for each test.
Data analysis was performed using SPSS 26.0. Kidney, ureter, and bladder (KUB) X-ray was taken on postoperative day 1 ensuring stent position and a CT scan was documented for evaluation of the existence of stone fragment just before ureteral stent removal. The stent is usually removed 1 month after surgery. Single-session stone-free rate (SFR) was defined as no stone fragments measured ≥2 mm under a CT scan 1 month after surgery according to relevant reviews. 3 Normally distributed parameters were compared using Student's t test between two groups, otherwise were compared using the two-sided Wilcoxon rank-sum test (Mann–Whitney U-test), whereas Pearson's chi-squared and Fisher's exact test were used for categorical variables. The significance level was set to 5% (p < 0.05) for each test.
Mechanical measurement
The maximal deflection was measured with the working channel empty, with a guidewire (either Cook Hiwire 0.038 inch [Cook Medical] or Innovex 0.025 inch IVX-UG-2515BAO [Innovex]), a laser fiber (either Lumenis Slimline 200 [Lumenis GmbH] or ACCU-Tech AT-HF-200 [ACCU-Tech, Beijing, China]), or a basket (either Urotech STN-T123-120 [Urotech GmbH, Achenmuhle, Germany] or Innovex [IVX-US-T1110, Innovex]. When the tip of the ureteroscope aligns with the tip of OD UAS, maximum torque could be achieved. The thickness of the OD UAS was measured using a digital caliper JZYQ-001 (Ningbo Minyan Instrument Co. Ltd., Zhejiang, China).
Results
The deflection angle of the OD UAS was recorded by manipulating four types of ureteroscopes with the working channel empty or with different instruments (Fig. 1I). Largely the deflection angle was ∼110° to 130° freeload, and 90° to 130° when loaded. Anqing demonstrated a slight advantage in maximum deflection angle.
The medical history and operation information of a total of 199 patients with UPJ stones or renal stones, and treated with FURL, were reviewed and compared (Table 1). Among them, 61 patients used Cook UAS and 138 patients used OD UAS. There were no significant differences in demographic characteristics (gender, age, height, weight, and body mass index) between the two groups. In total, 18.0% of patients in the Cook group and 16.7% of patients in the OD group were diagnosed with diabetes mellitus. None of the patients were immunodeficient, and the general ASA classification status was similar.
Demographic Characteristics and Operative Information of the Patients
Note: BMI stone-free definition: fragment <2 mm.
ASA = American Society of Anesthesiologists; BMI = body mass index; CRP = C-reactive protein; OD = omnidirectional; PCT = procalcitonin; SFR = stone-free rate; UAS = ureteral access sheath; WBC = white blood cell.
The stone burden was similar in the two groups, 55.7% of patients in the Cook group and 60.1% of patients in the OD group had hydronephrosis before surgery. In total, 26.2% of patients in the Cook group and 32.6% of patients in the OD group were prestented.
The mean operation time was similar (40.6 ± 12.1 vs 42.0 ± 13.2 minutes, p = 0.4952). Three patients in the Cook group whereas none who used OD UAS had a fever (>38°C, p = 0.0387). There was no statistical difference in the postoperative white blood cell or C-reactive protein within 48 hours between the two groups, but the procalcitonin (PCT) was significantly higher in the Cook group (3.70 ± 14.13 vs 0.07 ± 0.11 ng/mL, p = 0.0027). No major complications were encountered. The OD group achieved a significantly higher clearance rate (63.9% vs 94.2%, p < 0.0001), which complies with our initial experience of this novel device.
Discussion
In recent years, UASs with added vacuum suction ports were introduced to increase stone fragment evacuation and reduce intrarenal pressure (IRP) during laser lithotripsy. 4 –7 Yet there is still no sound evidence proving this improvement may increase stone clearance and reduce operating time. One of the major problems is that the UAS is usually placed at the UPJ area, whereas the stone might not always be placed and fragmented at the renal pelvis, the distance between the stone fragments and the UAS opening is too far to generate a strong suction force so that only small floating stone dust could be evacuated.
Unlike its conventional counterparts, the OD UAS is capable of entering each calyx, thus shortening the distance between the stone fragments and the UAS tip, so that the suction force is obviously much stronger, and the stone fragments are generally evacuated highly efficiently. The highly efficient laser lithotripsy and stone clearance could be achieved by our take-home Four-Step OD UAS User Guide (Fig. 2B).
Influence on safety
The tip of this OD UAS is soft, and the entire body is covered with a hydrophilic coating. The placements were generally smooth, and no UAS-related complications were encountered. We found the placement process similar to that of the Cook, usually we do not need to exert extra force.
Influence on SFR
We found that the OD UAS significantly improves the single session SFR and reduces operation time. Dusting is not strictly required and popcorning is usually enough for evacuation. For cases when the stones were too hard to be dusted, we just popcorned the stones and the OD UAS then evacuated small fragments efficiently. Previously published reports using similar flexible vacuum-assisted UAS can improve stone-free status. 8
Influence on operation time
From our perspective, the OD UAS could improve lithotripsy efficacy and shorten the operation time. Yet our current report is a retrospective study, and there was not a significant difference in the operation time between the two groups. Taken the large SFR difference into consideration, probably it is because the OD UAS removes far more stone fragments in a limited surgery time.
Theoretically, the OD UAS would exhibit the best performance for large stones in the presented patients, whereas for patients with narrow ureter and small stones, the OD UAS does not possess much advantage. In most cases the tip was quite stable and stayed in a particular calyx when the flexible ureteroscope was withdrawn, except when the patient has severe hydronephrosis and the calices were severely dilated. We had this experience in three patients.
Influence on vision and pelvic pressure
Combined with the vacuum suction, the OD UAS obviously improves vision by removing the stone dust during laser fragmentation, and theoretically it might also reduce pelvic pressure. Previously published reports using vacuum-assisted UAS also demonstrate better controlled IRP. 6,8 However, one thing to note is that, because of the immediate depression of the regional area, the suction could also cause increased bleeding if an injury presents. The surgeon must be careful with the laser fiber not to injure the parenchyma mucosa. Otherwise, the aggravated bleeding under vacuum suction could be troublesome. Also, large fragments may be sucked and these might get stuck. However, this may not pose a big problem because using the tip of the ureteroscope to touch a stuck stone fragment can free this, or we could use laser lithotripsy within the channel to further break it down.
Influence on infectious complications
Our present study has a limited number of subjects, which is hard to draw a conclusion as to whether OD UAS could further reduce infection complication rates. Although we implemented preventive measures for urinary tract infections in all cases before surgery, there were still cases of infectious stones and concealed infections. We found that none in the OD group had a postoperative fever, and the PCT was statistically lower in the OD group, suggesting a possible protective function in preventing infectious complications.
Notably, one patient who had severe hydronephrosis and infectious stones, who underwent operation using the Cook UAS for the first time, had a postoperative sepsis and a PCT >100 ng/mL. We then used OD UAS for the second time, the PCT stayed low, and the patient was discharged soon. The stone analysis revealed that 60% of the stones consisted of calcium phosphate.
Matters that need attention
Both the optical fiber ureteroscope and digital ureteroscope can bend this OD UAS, the maximum deflecting angle might vary. Most of the time, the OD UAS could be maneuvered into upper calices and middle calices without difficulty. For lower calices, it could also be positioned as the infundibulopelvic angle permits. Otherwise, the surgeon might need to relocate the lower caliceal stone to the middle or upper calices.
Despite all the advantages, the application of OD UAS also causes some issues. The OD UAS is longer than conventional ones, so during the positioning process, one needs to bear in mind the length issue. Otherwise, the tip, though coil-free and soft, might poke onto the renal mucosa and cause bleeding. Furthermore, bleeding could be aggravated by vacuum suction and affect vision. Another model 10F/12F is available, we usually do not use that one, but for patients who are not prestented and if their ureters are narrow, 10F/12F might be a good alternative option.
The soft tip of the OD UAS might kink (Fig. 2C) if there is a stenosis in the UPJ or the neck of the calices and hinder the suction of stone fragments or the retrieval of stones by baskets. So we advocate the application of prestent together with OD UAS to achieve a better effect.
Our report on OD UAS represents an early study on flexible UAS. There are other companies in China that are also developing similar products. We found the design of Yigao Med is comparatively better, easier to be inserted and placed. The OD UAS could shorten UAS tip–stone distance, improve fragments suction, substantially expedite the holmium laser lithotripsy process (Fig. 2D), and even expand the indication of FURL in terms of stone size. Stones that were >2 cm and <3 cm were generally cleared within 1 hour in a single session.
The largest stone in our study, which is 3.5 cm, was cleared in merely 55 minutes. We wonder whether this novel device might even change the guidelines. The weaknesses of our study include the retrospective nature and limited sample size. The p-values in Table 1 are exploratory and should be interpreted with caution considering the small sample size and lack of adjustment for residual confounding. Randomized controlled trials are required to generate a more convincing conclusion. Given the various kinds of ureteroscopes, and the divergence in operation experience among different urologists, multicenter prospective clinical trials are preferred.
Conclusion
OD UAS is a novel UAS with high safety and efficacy. Owing to its unique characteristic, it is capable of bending with the ureteroscope, entering renal calices, and is set in close contact with the stone. Combined with the suction port, OD UAS contributes greatly to dealing with large kidney stones, improving the SFR, and preventing infectious complications in ureteroscopic lithotripsy.
Footnotes
Authors' Contributions
J.D. and L.Z. contributed to data analysis and article writing. J.D., T.T.S., and X.M.Z. were involved in experiment conduction and in vitro data collection. T.T.S. carried out drawing and illustration. S.B.Q., L.J.S., Y.T.H., L.Z., and J.W.C. oversaw surgery performance and clinical data collection. J.C., L.Z., and J.W.C. took charge of project development and supervision.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The retrospective study was approved by the Xinhua Hospital Ethics Committee and Institutional Review Board (XHEC-D-2022-194).
Author Disclosure Statement
There have been no potential competing interests in this study.
Funding Information
No funding was received for this article.