
Abstract
Introduction:
Holmium laser enucleation of the prostate (HoLEP) is routinely performed with a 24F, 26F, or a 28F scope. Proponents of the larger scopes propose that a bigger sheath size allows for superior flow and visibility leading to a more efficient operation and better hemostasis. Those utilizing the smaller scopes suggest that the smaller sheath is less traumatic, resulting in lower stricture rates and temporary incontinence. We sought to compare outcomes of ambulatory HoLEP using the 24F and 28F laser scope.
Materials and Methods:
From May 2022 to March 2023, we randomized patients undergoing HoLEP (<200 cm3 in size) 1:1 to either a 24F or 28F scope. The primary outcome was differences in surgical duration between groups (minutes). Secondary outcomes included surgeon scope evaluation and postoperative patient results.
Results:
There was no difference in patient characteristics in those randomized to 28F (n = 76) vs 24F (n = 76) (p > 0.05) scopes. Procedural duration and efficiencies were not different between groups (all p > 0.05). The 28F scope was associated with improved surgeon-graded irrigation flow and visibility (p < 0.001). Patients treated with the 28F scope were more likely to achieve effective same-day trial of void (SDTOV) (28F 94.3% vs 24F 82.1%, p = 0.048) and have a shorter length of stay (LOS) (28F 7.0 vs 24F 11.9 hours, p = 0.014), however, rates of same-day discharge (SDD) were not statistically different (28F 87.8% vs 24F 78.4%, p = 0.126). There was no difference between the cohorts in rates of 90-day emergency room presentations, re-admissions, complications, or functional ouctomes (p > 0.05).
Conclusions:
We identified no clear advantage of scope size with regard to intraoperative or postoperative outcomes at 3-month follow-up due to scope size. However, if SDD is part of your postoperative pathway, the 28F scope may shorten LOS and increase rates of effective SDTOV.
Clinicaltrials.gov:
NCT05308017.
Introduction
Holmium laser enucleation of the prostate (HoLEP) is a size-independent surgical treatment option for benign prostatic hyperplasia (BPH). 1,2 HoLEP has been associated with a shorter length of stay (LOS), operative times, and postoperative catheter durations, as well as lower rates of blood transfusions than open and robotic simple prostatectomy (RSP). 3,4 Despite these advantages, some authors have found that laser enucleation can be associated with a higher rate of transient postoperative incontinence relative to RSP. 3 Transient postoperative urinary incontinence is a phenomenon that occurs in ∼10% to 20% of patients who undergo HoLEP and may last 3 to 6 months; however, long-term urinary incontinence is uncommon. 5,6 The proposed mechanism of postoperative incontinence is multifactorial and likely related to a temporary external urethral sphincter injury secondary to urethral dilation and scope manipulation, an exacerbation of overactivity symptoms from laser inflammation, or a combination of both. 5,7
Early apical release techniques, postoperative pelvic floor physiotherapy, intradetrusor onabotulinumtoxinA injections, and other experimental strategies have been studied in an attempt to minimize postoperative incontinence after laser enucleation. 7 –9 Identifying strategies to improve the postoperative laser enucleation recovery will be important in solidifying laser enucleation as the new gold standard of surgical BPH management.
HoLEP is routinely performed with 24F, 26F, and 28F laser scopes and has even been reported with 22F and 18.5F scopes. 10 Proponents of larger caliber scopes suggest that the larger scope size allows for improved visualization, hemostasis, and operative efficiencies. Proponents of a smaller scope diameter suggest that by eliminating the need for pre-HoLEP urethral dilation to accommodate a larger scope, transient urinary incontinence is less. It has also been proposed that a smaller caliber scope is less traumatic to the urethra resulting in lower rates of bladder neck contracture (BNC) and urethral stricture disease. 11 In a retrospective trial comparing 26F and 28F laser scope sheath sizes, the authors did not find a statistically significant difference in the incidence of urethral strictures (1.8% vs 3.5%, p = 0.41) or BNC (0.0 vs 2.4%, p = 0.059) between the two sheath sizes after HoLEP. 11
Recently, there has been an increasing push to offer HoLEP as ambulatory surgery with a same-day trial of void (SDTOV). 12 –15 Despite improvements in laser technology, rates of failed same-day discharge (SDD) range from 10% to 40%. 12 –16 Currently, to our knowledge, there are no level-one evaluations examining scope size and ambulatory laser enucleation outcomes. 11,17 The aim of our study is to determine if a smaller diameter scope is associated with improved laser enucleation postoperative recovery without sacrificing operative efficiencies, rates of SDD, or increasing intraoperative or postoperative complication rates.
Materials and Methods
This prospective single-blind, parallel-design, 1:1 randomized controlled trial was conducted to compare HoLEP patient outcomes and surgeon satisfaction using 24F and 28F scopes. Institutional review board (IRB) approval was attained (STU00215646) and the study was prospectively registered on
Our study received funding for equipment costs from Richard Wolf Medical™. The protocol development and data collection, analysis, and writing were performed by the research group without input from study sponsors.
Adult males (≥18 and ≤89 years old) who underwent HoLEP for the treatment of symptomatic BPH between May 2022 to March 2023 were candidates for enrollment. Patients with prostates >200 cm3 on preoperative imaging and patients undergoing concurrent procedures (ureteroscopy or percutaneous nephrolithotomy) were excluded from the study. Individuals lacking capacity for informed consent, those requiring planned overnight admission, and non-English-speaking patients were excluded from the study.
Randomization was performed 1:1 to the Storz 28F laser scope (control) or the Wolf 24F (treatment) laser scope. The surgery and operating room teams became aware of the treatment allocation ∼30 minutes before the HoLEP procedure to provide time to open the correct surgical trays.
The primary outcome was differences in surgical duration between groups (minutes). Secondary outcomes included surgeon scope evaluation and postoperative patient outcomes. Postoperative follow-up consisted of a standardized telephone call at 1 week and an in-person follow-up visit at 3 months. At the 3-month follow-up, patients completed standardized lower urinary tract symptom (LUTS) questionnaires (American Urological Association symptom score [AUASS]), sexual function questionnaires, incontinence questionnaires (Michigan Incontinence Symptom Index [MISI]), a postvoid residual, and a prostate-specific antigen (PSA) serum blood test. Patients with satisfactory outcomes at 3 months were followed afterward as needed, while patients with ongoing bothersome LUTS or elevated PSAs were scheduled follow-up at 6 months postoperatively. Patients enrolled within the study were asked to complete automated daily Research Electronic Data Capture text message/email surveys with relevant standardized postoperative questions focusing on hematuria, dysuria, and urinary continence. More extensive text message/email surveys were delivered at 1 and 3 months postoperatively.
Patients who did not arrange follow-up at 3 months were contacted for a telephone interview at the completion of final data collection by our research coordinators.
The statistical analysis was performed with an intention-to-treat protocol. Student t-tests were performed for means of continuous variables. Kaplan–Meier survival analysis was performed to calculate and display time to resolution of dysuria, hematuria, and incontinence in each cohort. A p-value of <0.05 was significant. All data analyses were performed with SPSS (IBM SPSS Statistics for Windows version 29) with an intention-to-treat protocol. Our power calculation for sample size was based on our average HoLEP case times obtained from all HoLEP procedures on glands <200 mL in our prospectively collected database (65 ± 22-minute standard deviation). To detect a >15% difference that we defined as a clinically significant increase (e.g., >10-minute longer duration on an average 65-minute case) with alpha of 0.05 and 80% power, we planned to enroll 76 patients in each arm, 152 in total.
Results
Patient characteristics
Between May 2022 and March 2023, 152 patients were enrolled within the study (Storz 28F n = 76 [50%], Wolf 24F n = 76 [50%]) (Fig. 1). There were no differences in preoperative patient characteristics, including age (28F 70.1 vs 24F 68.6, p = 0.218), prostate size (28F 100.2 cm3 vs 24F 92.3 cm3, p = 0.355), preoperative AUASS (28F 20.0 vs 24F 20.6, p = 0.732), anticoagulation status (28F 10.8% vs 24F 12.0%, p = 0.821), or preoperative urinary incontinence rates requiring pads (28F 10.5% vs 24F 6.6% p = 0.732) (Table 1). Mean follow-up was 3.8 months in the 24F arm and 4.1 months in the 28F arm. Overall, 94.7% of the total patients (28F n = 72, 24F n = 72) were followed to the completion of their 3-month postoperative visit.
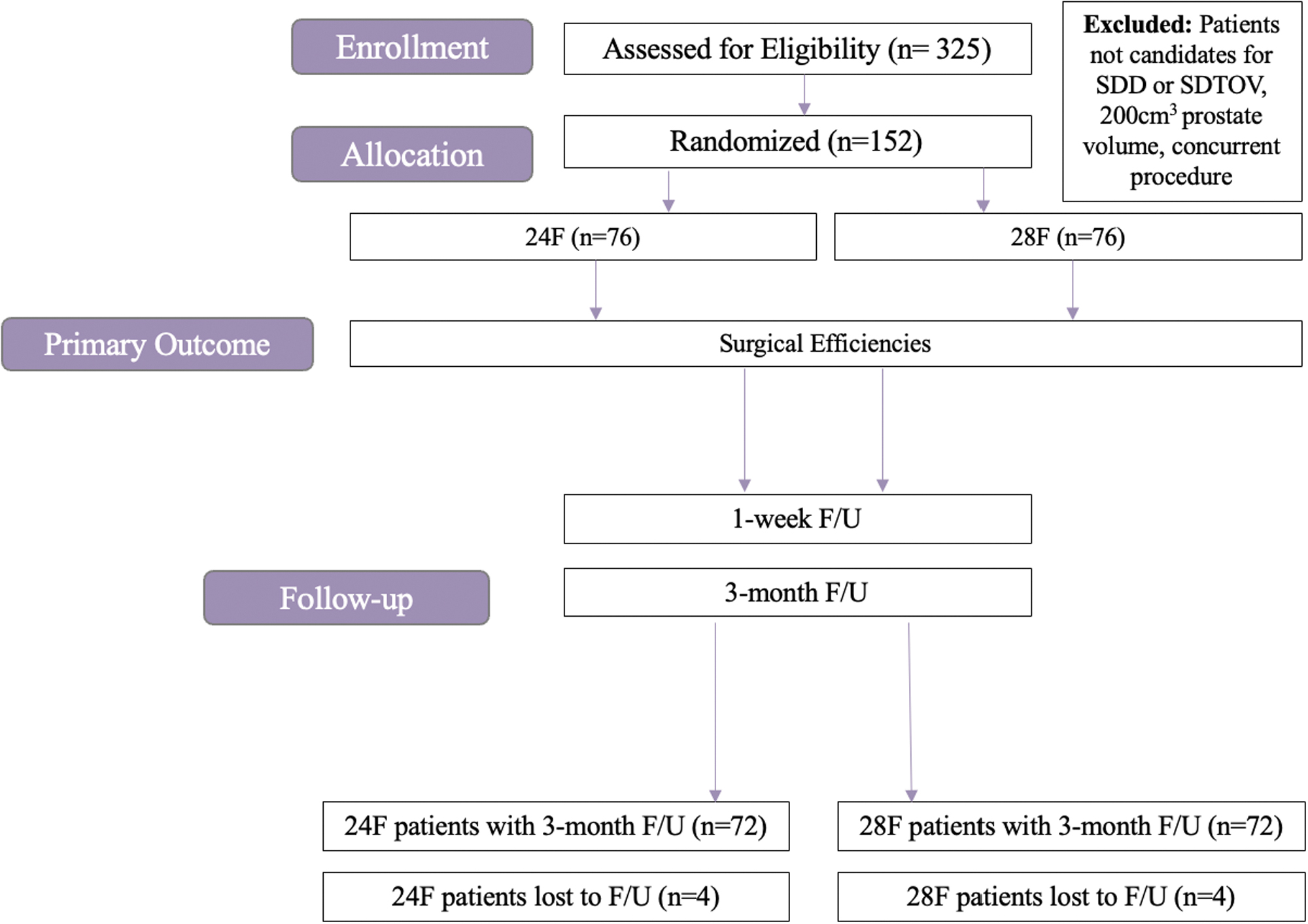
Study schema. SDD = same-day discharge; SDTOV = same-day trial of void.
Patient Demographic Characteristics and Prostate Gland Features
Bolded indicates statistical significance (p < 0.05).
ASA = American Society of Anesthesiology score; AUASS = American Urological Association symptom score; BMI = body mass index; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; CrCl = Creatinine Clearance; HoLEP = holmium laser enucleation of prostate; PSA = prostate-specific antigen; SD = standard deviation; SHIM = Sexual Health Inventory for Men; UTI = urinary tract infection.
Intraoperative findings: procedural duration and efficiencies
There were no differences in the mean procedural times between the 28F and 24F cohorts (51.8 vs 51.8 minutes, p = 0.981) (Table 2). There was no difference in Operating Room (OR) specimen weight between groups (28F 58.5 g vs 24F 56.7 g, p = 0.793) (Table 2). There were no differences in mean enucleation (28F 31.1 minutes vs 24F 26.7 minutes, p = 0.153) or morcellation time between groups (28F 6.5 minutes vs 24F 7.9 minutes, p = 0.193). When examining enucleation and morcellation efficiencies (morcellation time (minutes) per gram of tissue removed and enucleation time (minutes) per gram of tissue enucleated), there were no differences between the two cohorts (all p > 0.05).
Operative Parameters
Bolded indicates statistical significance (p < 0.05).
Follow-up outcomes and complications
The 28F resectoscope was associated with improved surgeon-graded ratings, including flow (28F 5.0 vs 24F 3.5, p < 0.001) and visualization (28F 5.0 vs 24F 3.1, p < 0.001) (Table 2). Of the patients who underwent HoLEP, 3.9% (6/152) of patients required conversion of the laser scope to a different size and all conversions (28F 0/76 [0%] vs 24F 6/76 [8%], p < 0.002) occurred within the 24F arm (Table 2). One patient within the 24F arm experienced a superficial bladder injury during morcellation. There was no difference in intraoperative rates of complications (28F 5.2% vs 24F 2.7%, p = 0.08). Patients who were treated with the larger 28F scope were more likely to achieve effective SDTOV (28F 94.3% vs 24F 82.1%, p = 0.048) and have a shorter postoperative LOS (28F 7.0 vs 24F 11.9 hours, p = 0.014); however, rates of SDD were not statistically different (28F 87.8% vs 24F 78.4%, p = 0.126) (Table 3; Figs. 2 and 3).
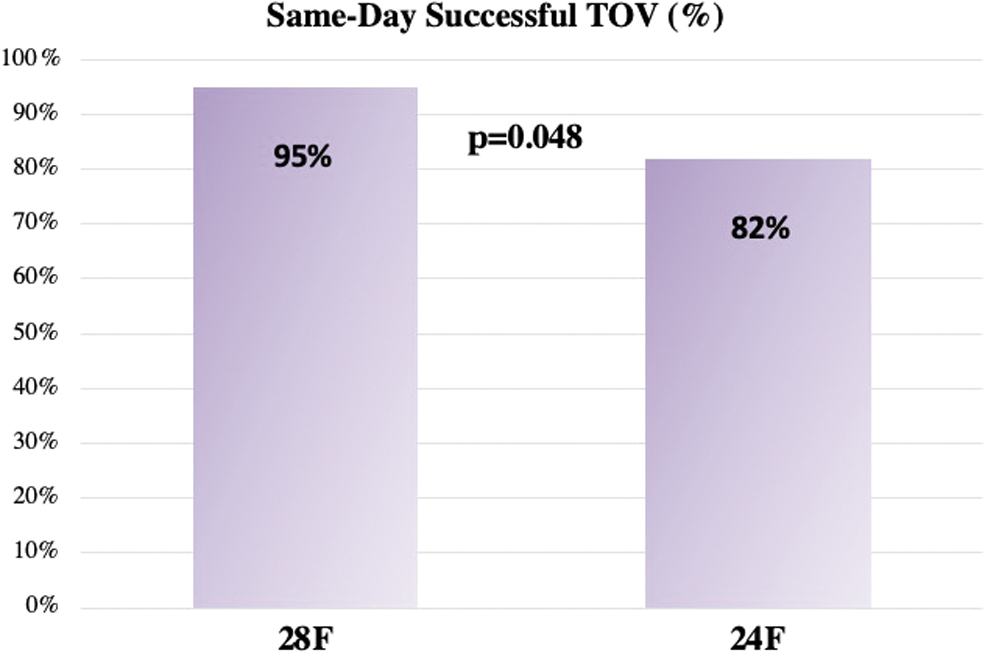
Rate of SDTOV.
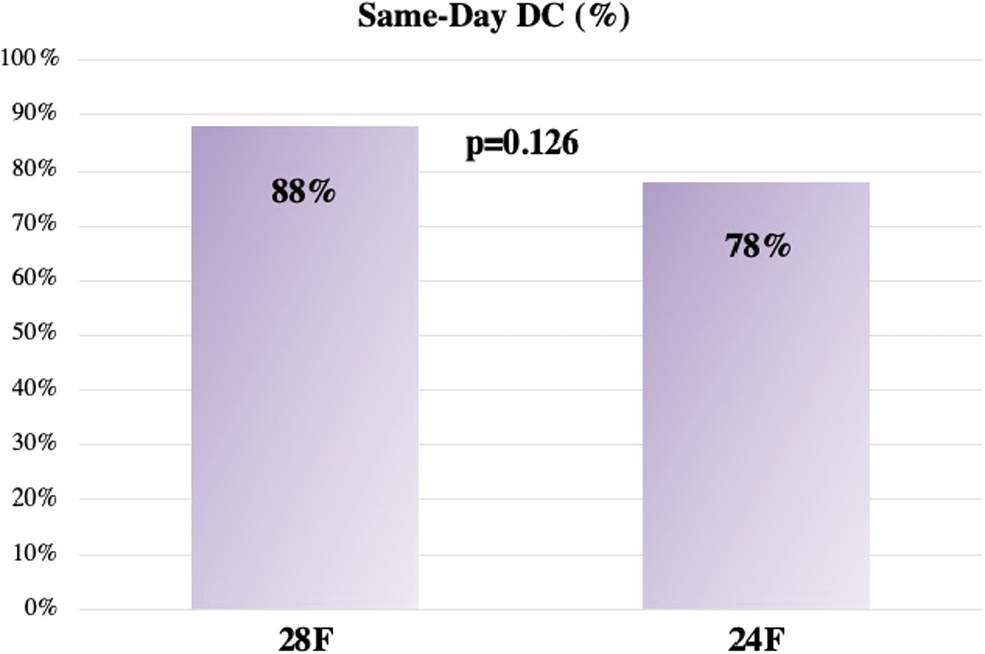
Rate of SDD.
Outcome Measures and Postoperative Disposition
Bolded indicates statistical significance (p < 0.05).
Rates of emergency room presentations (28F 13% vs 18%, p = 0.396), 90-day complications (28F 13% vs 24F 16%, p = 0.671), and 90-day readmissions (28F 1.3% vs 7.9%, p = 0.053) were not statistically different between groups. There were no BNCs or urethral strictures that required treatment in either group during short-term follow-up. Time to resolution of self-reported postoperative hematuria, dysuria, and urinary leakage did not differ between groups (p > 0.05) (Table 4; Figures 4 –6). Rates of de novo urinary incontinence and rates of return to normal activity at 3 months postoperatively did not differ between cohorts (p > 0.05) (Table 4).
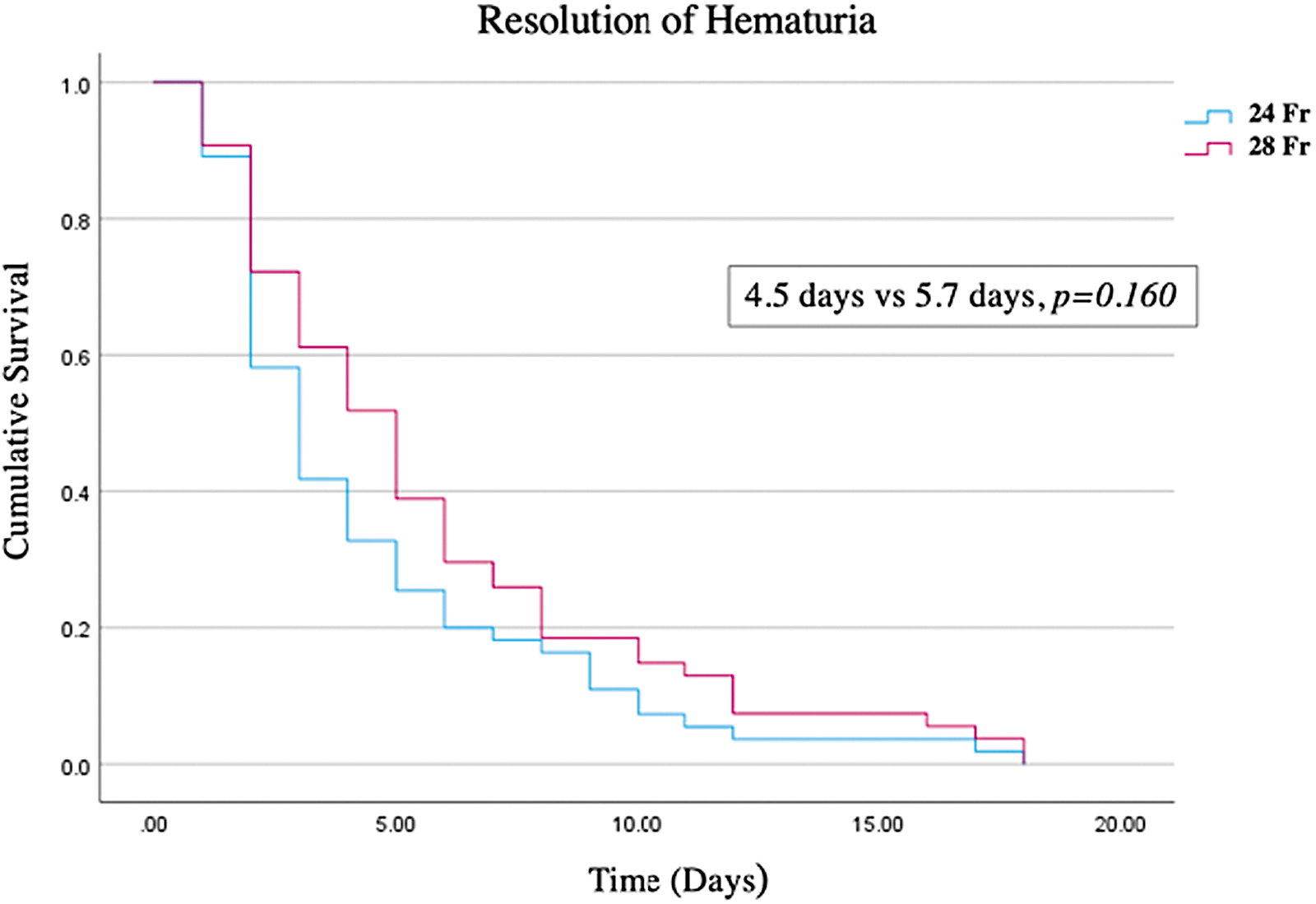
Kaplan–Meier freedom from hematuria.

Kaplan–Meier freedom from incontinence.
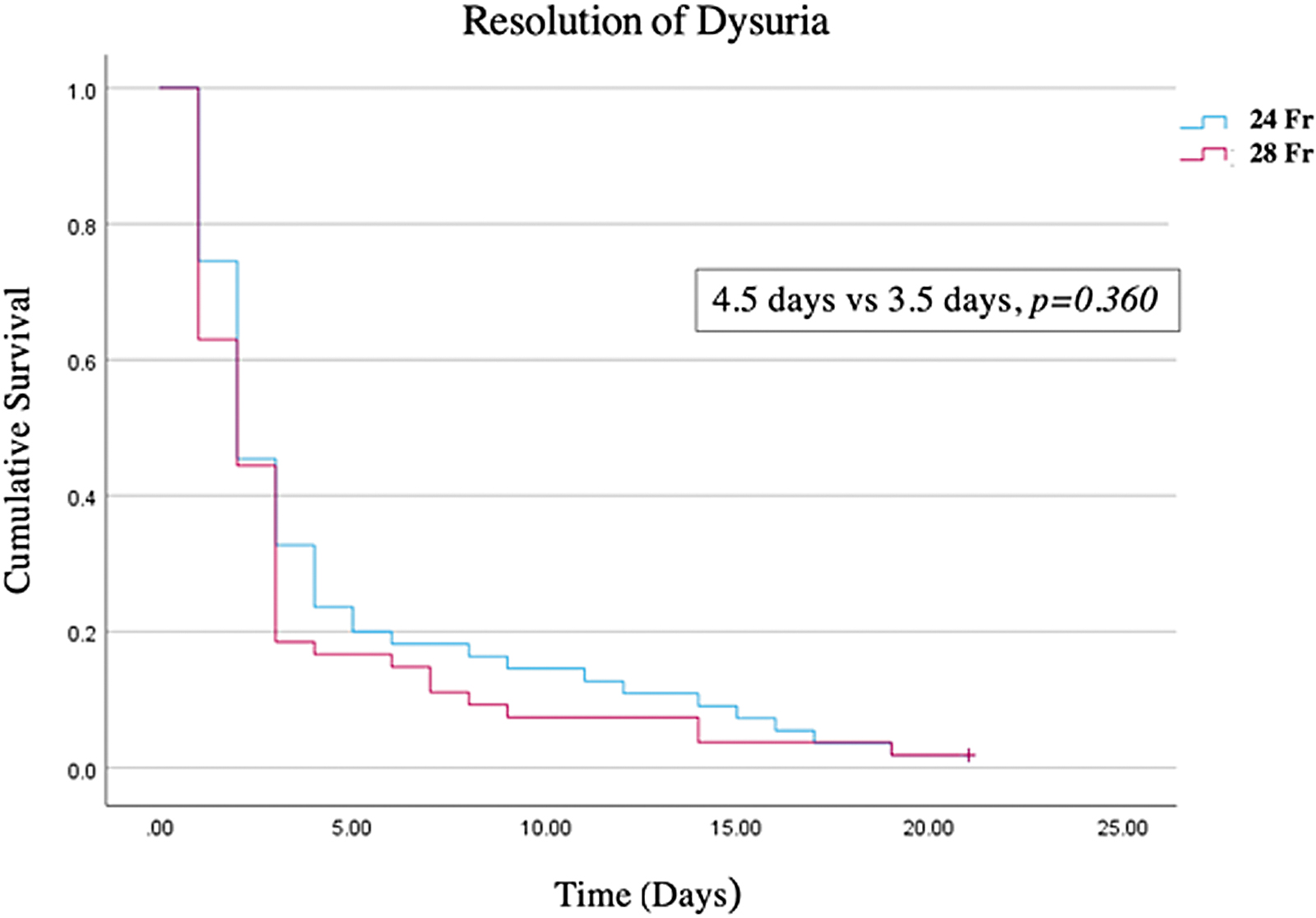
Kaplan–Meier freedom from dysuria.
Follow-Up: Emergency Department Presentation, Complications, and Readmissions
ER = emergency room; MISI = Michigan Incontinence Symptom Index.
Discussion
Endourology instruments have undergone an evolution toward progressive miniaturization in an attempt to enhance the minimally invasive nature of BPH and percutaneous stone procedures. Laser resectoscopes utilized for transurethral laser enucleation of the prostate (LEP) procedures are no exception to this evolution. Despite the push toward scope size reduction, our study is the first randomized controlled trial to examine the effects of scope size (28F vs 24F) on ambulatory PM HoLEP perioperative and postoperative outcomes.
We did not identify a procedural duration or efficiency advantage with the utilization of a larger scope as hypothesized. Although procedural efficiencies were not different between cohorts, we anecdotally noted that morcellation was easier when using the larger 28F scope. Similar to the retrospective study performed by Thai et al. of 502 HoLEP patients comparing a 28F vs 26F scope, morcellation efficiency (g/min) was higher in the larger scope cohorts, but failed to reach a level of significance in both studies. 11 Conversly, Yildiz et al. did find a statistically significant reduction in morcellation and operative efficiency when retrospectively comparing HoLEP using a 24F scope compared with a 28F scope. 17 Irrigation flow and hence visualization are impeded to a degree with the 24F scope when the morcellator handpiece occupies the rigid morcelloscope.
This was evidenced by lower subjective surgeon gradings for irrigation flow and visualization in the 24F cohort scope. All scope conversions (n = 6, 4%) from 24F to 28F occurred during the morcellation phase of the HoLEP procedure. Patients who required an intraoperative sheath conversion in the 24F cohort had a significanlty greater OR specimen weight (92.9 g vs 50.8 g, p = 0.006). Impaired visualization during a large gland morcellation contributed to the bladder injury that occurred within the 24F arm. The bladder injury was superficial, and the patient was managed with an indwelling Foley catheter overnight. The primary surgeon (A.E.K.) performed all morcellations within the 24F scope without trainee involvement to ensure procedural safety in the setting of reduced procedural visualization.
This is in stark contrast to the large degree of trainee involvement with nearly all morcellations in the 28F scope cohort. It is difficult to know how heterogeneity in trainee (resident and fellow) involvement affected surgical efficiencies within our study. With our experience gained utilizing the 24F scope in clinical practice, we have anecdotally found that the 24F scope has unique procedural benefits for patients with known urethral stricture disease, either untreated or in the setting of prior urethroplasty, and for patients with penile prosthesis to avoid a perineal urethrostomy. However, overall visualization and ease of use make the 28F ideal for early learners and large complex prostates.
High-powered PM holmium lasers have enabled urologists at high-volume centers to offer ambulatory HoLEP to most patients as a standard of care irrespective of preoperative prostate volume or anticoagulation status. 13 Our study is the first randomized controlled trial to our knowledge, to examine the effect of resectoscope size on transurethral BPH surgery outcomes when utilizing an SDD and SDTOV ambulatory surgery pathway. Patients who underwent HoLEP with the larger 28F had more success with the SDD and SDTOV pathways. Persistent gross hematuria has been previously identified as the most common cause for failure of an ambulatory HoLEP pathway. 14 We hypothesize that superior irrigation flow and visualization led to improved hemostasis and less clinically significant postoperative gross hematuria, resulting in a higher rate of effective SDTOV and shorter LOS with the 28F scope.
Thai et al. did not identify a difference between the 26F and 28F scope cohorts in hospital duration, rate of failed postoperative day 1 TOV, and length of postoperative catheterization in their retrospective cohort study when utilizing an inpatient stay, non-PM holmium laser, and a postoperative day 1 TOV. 11 In our opinion, if a urologist is attempting to offer HoLEP as an ambulatory procedure with a same-day decatheterization, utilization of a larger caliber scope (28F) is likely to be beneficial.
A unique strength of our study was our assessment of postoperative functional outcomes with text message postoperative patient questionnaires. Our daily questionnaires provide novel insights into the day-to-day recovery following HoLEP in the contemporary laser era and provide for detailed comparison between scope cohorts. Irrespective of the scope utilized, there were no clinically significant differences between the groups in regard to postoperative recovery (self-reported time to resolution of hematuria/incontinence/dysuria, postoperative AUASS or MISI score, mean postoperative anticholinergic use, preoperative pelvic floor physiotherapy, rates of de novo incontinence at 1 or 3 months, or rates of return to normal baseline activity at 1 or 3 months) (Table 4; Figs. 4–6). Mean time to self-reported resolution of incontinence was longer in the 28F group, however, this difference did not meet a level of statistical significance (Fig. 5).
Regardless of scope utilized, mean time to self-reported resolution of postoperative dysuria, incontinence, and hematuria is brief.
Within our study, the smaller 24F scope was not associated with a lower rate of postoperative urethral stricture or BNC treatment, however, we did not identify any patients in either cohort diagnosed or treated with these complications. We are unable to make final conclusions regarding urethral stricture rates or BNC rates between scopes at this time based on the duration of follow-up (mean 4 months) and low expected event rates of these postoperative complications. 18 A secondary analysis will be required to ascertain if differences exist in rates of urethral stricture and BNC after HoLEP between 28F and 24F cohorts with more extensive follow-up.
Our study is limited by our single-center design and the heterogeneity of trainees in the 28F arm vs minimal trainee involvement in the 24F scope arm. The generalizability of these results may be limited using PM holmium laser technology, our institutional experience with ambulatory HoLEP, and the primary surgeon's level of experience. Subjective surgeon scope gradings, TOV, and discharge decisions may have been subject to bias as they were performed with knowledge of the scope utilized for each patient. Furthermore, our follow-up protocol lacked a routine assessment of postoperative uroflow. Despite these limitations, this was a well-executed single-blind randomized controlled trial from a high-volume HoLEP center with equal preoperative patient demographics between groups and a low number of patients lost to follow-up (n = 8, 5.3%).
de Figueiredo et al. recently described their surgical technique with their proof-of-concept video article highlighting their anecdotal LEP experience with a 22F and 18.5F laser resectoscope. 10 Further retrospective and prospective studies are required to determine if further miniaturization of laser resectoscopes <24F will improve rates of temporary postoperative incontinence and rates of urethral stricture and BNC, without sacrificing enucleation and morcellation efficiency or success of ambulatory LEP pathways.
Conclusions
We found that HoLEP can be performed safely and effectively with both the 24F and 28F laser scopes. Surgeon satisfaction ratings were higher with the 28F scope, but there were no differences in procedural duration or operative efficiencies. The 28F scope is associated with higher rates of effective SDTOV and shorter LOS. Excellent postoperative safety and functional outcomes were achieved after ambulatory PM HoLEP irrespective of scope size. Hence, the 24F scope should be considered a viable tool for experienced surgeons and can be safely utilized in situations that call for a smaller scope diameter. A secondary analysis with longer follow-up will be required to determine if rates of BNC or urethral stricture are improved with the utilization of the smaller scope size.
Footnotes
Authors' Contributions
All listed authors made contributions to the completion of this study. N.S.D.: Patient consent, data extraction, data analysis, article writing, and submission. M.S.L.: Project funding, project design, IRB application, and article editing. M.A.A.: Project design and IRB application. J.G.: Article writing and article review. P.X.: Article review. A.M. and A.F.-A.: Patient consent and database entry. J.H.: Project design, IRB application, and consents. A.E.K.: Project design and article editing.
Author Disclosure Statement
A.E.K. is a consultant for Boston Scientific, Wolf, Storz, and Virtuoso Surgical. She is a data safety monitoring board member of Sonomotion and Uriprene. M.S.L. is a consultant for Lumenis.
Funding Information
Richard Wolf Medical Instruments Corporation: FP-SP0072330.