
Abstract
Background:
Same-session bilateral ureteroscopy may reduce the number of surgeries for stone removal but can lead to higher overall complication rates. We aimed to compare same-session bilateral ureteroscopy with unilateral ureteroscopy in terms of perioperative outcomes.
Methods:
We used the GeRmAn Nationwide inpatient Data (GRAND), provided by the Research Data Center of the Federal Bureau of Statistics (2005–2021). We assessed, through multiple patient-level analyses, severe perioperative complications, mortality, length of hospital stay, hospital revenues, intensive care unit admission, and the evolution of ureteroscopy during the last years in Germany.
Results:
We included 833,609 patients undergoing either same-session bilateral (n = 6914, 0.8%) or unilateral (n = 826,695, 99.2%) ureteroscopy for stone management. Patients undergoing bilateral ureteroscopy presented worse baseline characteristics. After adjusting for these characteristics, same-session bilateral ureteroscopy, compared to unilateral ureteroscopy, was significantly associated with higher odds of postoperative sepsis (odds ratio [OR]: 2.4, 95% confidence interval [CI]: 2–2.8, p < 0.001), myocardial infarction (OR: 2, 95% CI: 1.03–3.5, p = 0.024), acute kidney disease (OR: 2.8, 95% CI: 2.5–3.2, p < 0.001), transfusion (OR: 4.2, 95% CI: 3.6–4.8, p < 0.001), urinary tract infection (OR: 1.6, 95% CI: 1.5–1.7, p < 0.001), intensive care unit admission (OR: 1.9, 95% CI: 1.6–2.3, p < 0.001), and mortality (OR: 3.1, 95% CI: 2.1–4.5, p < 0.001). Similarly, the length of hospital stay was longer, and the in-hospital costs were higher (p < 0.001) after same-session bilateral ureteroscopy. Interestingly, the annual cases of ureteroscopy have undergone about a threefold increase in the last 17 years.
Conclusions:
The present real-world data demonstrate that same-session bilateral ureteroscopy leads to higher rates of perioperative myocardial infarction, acute kidney disease, transfusion, urinary tract infections, sepsis, and intensive care unit admission, as well as to increased length of hospital stay, costs, and inpatient mortality compared to unilateral ureteroscopy.
Introduction
The continuous technological evolutions in semirigid and flexible ureteroscopes, laser sources, suction devices, grasping tools, and access sheaths enable endourologists to safely access and efficiently remove stones from all parts of the upper urinary tract. 1 Despite the similar technological evolutions in percutaneous lithotripsy and extracorporeal shockwave lithotripsy, ureteroscopy is currently recommended as a first-line treatment modality for most ureteric and renal calculi. 2 –4 Given that ureteroscopy is generally safe and well tolerated and considering that up to 25% of all patients diagnosed with urolithiasis present bilateral calculi, some endourologists consider treating bilateral urolithiasis in a single session in well-selected cases. 5,6
It has been postulated that same-session bilateral ureteroscopy may be feasible without increasing the perioperative mortality and morbidity. 7 Even though multiple studies have suggested that same-session bilateral ureteroscopy is safe and effective for the management of urolithiasis, major urological guidelines do not currently recommend in favor of this approach due to the lack of high-quality evidence. 8 Indeed, the recommended approach for the management of bilateral urolithiasis is a staged ureteroscopy. Nevertheless, current guidelines advocate that bilateral ureteroscopy during the same session is feasible resulting in equivalent stone free rates but may lead to higher overall complication rates. 9
Even though these complications are considered, in most cases, minor, a holistic and critical analysis of the effect of same-session bilateral ureteroscopy on perioperative complications is still lacking. 10 In this scope, we aimed to compare same-session bilateral ureteroscopy with unilateral ureteroscopy in terms of perioperative outcomes.
Methods
GeRmAn Nationwide inpatient Data
For the purposes of the present analysis, the inpatient data of all hospitals in Germany from 2005 to 2021 were used. These data include coexisting conditions, surgical procedures, and perioperative outcomes of all hospitalized patients in Germany apart from psychiatric, forensic, and military cases. These data are stored anonymized at the German Office of Statistics (Wiesbaden, Germany) and were provided for analysis upon agreement (LMU—4710–2022). After the implementation in Germany of a diagnosis- and procedure-related remuneration system in 2004 (G-DRG), all hospitals must transfer these inpatient outcomes to the Institute for the Hospital Remuneration System to receive their remuneration. Coexisting conditions and perioperative outcomes are coded based on the International Statistical Classification of Diseases and Related Health Problems, 10th revision, German modification (ICD-10-GM), whereas the surgical procedures are coded based on the German Procedure Classification (OPS). The coding guidelines are provided by the German Institute for Medical Documentation and Information to ensure uniform documentation in Germany.
Data source
For this study, we included all patients undergoing ureteroscopy due to calculi (OPS code: 5–562.4 and 5–562.5). To obtain data on baseline characteristics and perioperative complications, we used further diagnostic and procedural codes based on the ICD-10-GM and OPS system. The primary outcome of the GeRmAn Nationwide inpatient Data (GRAND) study was to assess the effect of single-session bilateral ureteroscopy vs unilateral ureteroscopy for stone removal on severe perioperative complications (sepsis, myocardial infarction, acute kidney disease, transfusion, and urinary infection). Secondary outcomes included the effect of single-session bilateral ureteroscopy vs unilateral ureteroscopy on length of hospital stay, hospital revenues, mortality (defined as death within hospitalization), and intensive care unit admission, as well as the evolution of single-session bilateral ureteroscopy and unilateral ureteroscopy throughout the years in Germany.
Statistical analysis
All analyses were undertaken from the Research Data Center of the German Office of Statistics on our behalf based on R codes developed by our research group (source: Research Data Center of the German Office of Statistics, DRG Statistics 2005–2021, own calculations). Considering that our research group had only access to summary results provided by the Research Data Center of the German Office of Statistics (and not to patient-level data), approval by an ethics committee or patient informed consent were not required according to the German legislation.
The corresponding comparisons between single-session bilateral and unilateral ureteroscopy were performed with the chi-squared for categorical variables and the t-test for continuous variables. All categorical variables were provided as frequencies with proportions, whereas all continuous variables as mean ± standard deviation. We performed a multivariable logistic and linear regression analysis to evaluate the effect of the selected surgical approach (single-session bilateral vs unilateral ureteroscopy) on perioperative outcomes (morbidity, mortality, length of hospital stay, intensive care unit admission, and hospital revenues). All regression models were adjusted for sex, age, obesity, history of chronic kidney disease, diabetes, and prior stenting. Odds ratios (ORs) with 95% confidence intervals (CIs) were estimated for all logistic models and a two-sided p-value lower than 0.05 was considered statistically significant for all analyses.
Results
Baseline characteristics
We included a total of 833,609 patients with a mean age of 53 ± 16 years undergoing either same-session bilateral (n = 6914, 0.8%) or unilateral (n = 826,695, 99.2%) ureteroscopy for stone management. A total of 573,791 (69%) patients were men, while 41,402 (5%) had documented severe obesity, 178,031 (21%) had hypertension and 57,179 (6.9%) diabetes. More than half of all patients had previously received ureteral stenting (n = 448,447, 54%). Patients undergoing bilateral ureteroscopy displayed worse baseline characteristics (Table 1). The number of patients undergoing ureteroscopy substantially increased throughout the last years reaching a maximum number of 68,267 yearly cases in 2019 (from 27,424 cases in 2005) for unilateral ureteroscopy and 670 yearly cases in 2021 (from 180 cases in 2005) for bilateral ureteroscopy. Interestingly, the number of patients undergoing unilateral ureteroscopy decreased during the coronavirus disease 2019 (COVID-19) pandemic, while the number of patients undergoing bilateral ureteroscopy increased (Fig. 1).
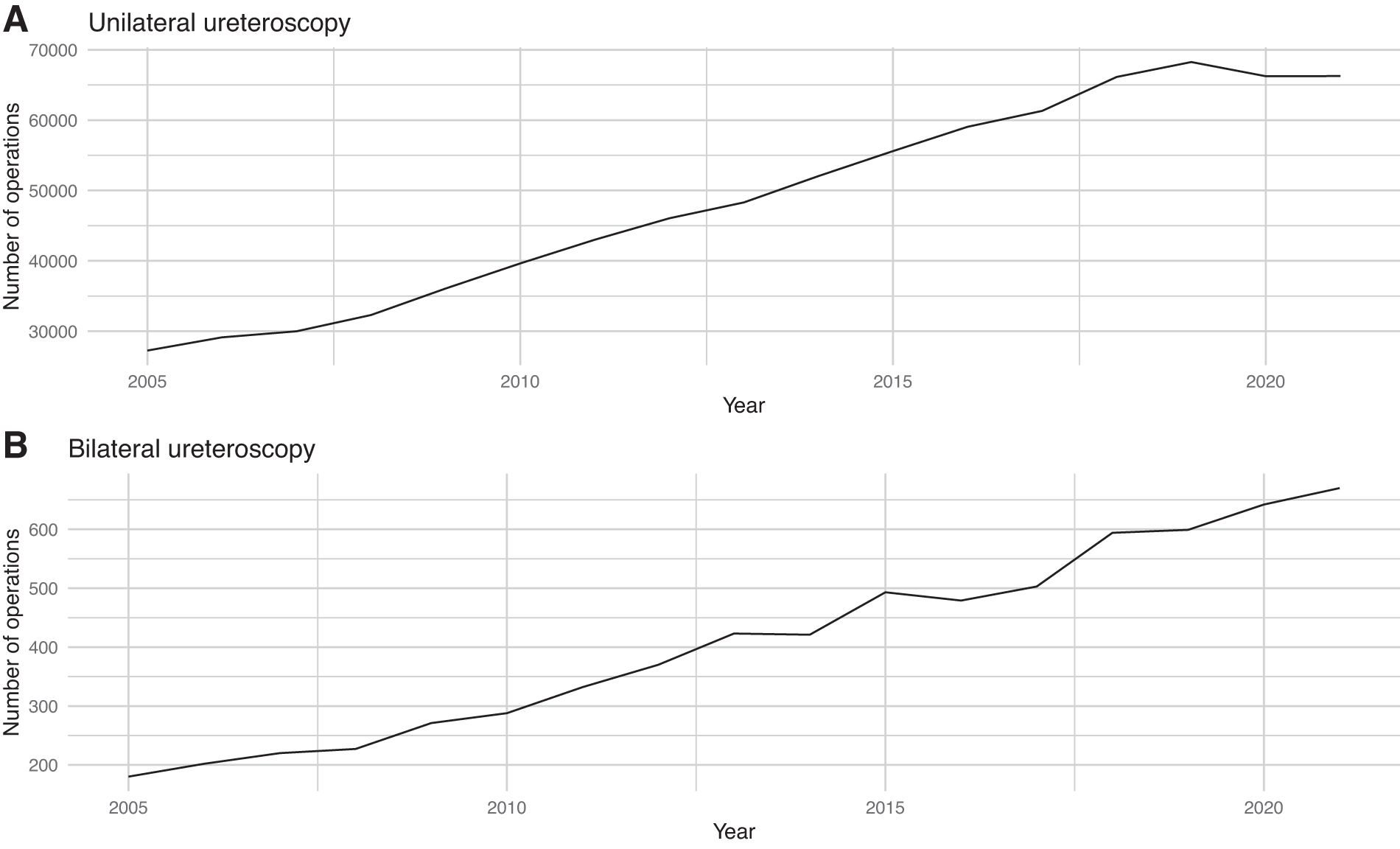
The annual number of cases of unilateral and bilateral ureteroscopy.
Baseline Characteristics of the Included Patients Based on Surgical Approach for Stone Management
Variables are presented as mean ± SD or frequencies with proportions. The t-test was performed for comparisons between continuous variables and the chi-squared test for comparisons between categorical variables. The bold cells indicate statistically significant p-values.
SD = standard deviation.
Perioperative morbidity
Even though the total number of perioperative complications was relatively low in the whole study cohort, these complications were more frequent after same-session bilateral ureteroscopy than with unilateral ureteroscopy. Overall, same-session bilateral ureteroscopy, compared to unilateral ureteroscopy, was significantly associated with higher odds of sepsis (2.2% vs 0.7%; OR: 2.4, 95% CI: 2–2.8, p < 0.001), myocardial infarction (0.2% vs <0.1%; OR: 2, 95% CI: 1.03–3.5, p = 0.024), acute kidney disease (3.9% vs 1.1%; OR: 2.8, 95% CI: 2.5–3.2, p < 0.001), transfusion (3.1% vs 0.5%; OR: 4.2, 95% CI: 3.6–4.8, p < 0.001), and urinary tract infection (14% vs 8.1%; OR: 1.6, 95% CI: 1.5–1.7, p < 0.001). Therefore, in the multivariate analysis after adjusting for sex, age, obesity, history of chronic kidney disease, diabetes, and prior stenting, same-session bilateral ureteroscopy was associated with 140% higher odds for sepsis, 100% higher odds for myocardial infarction, 180% higher odds for acute kidney disease, 320% higher odds for transfusion, and 60% higher odds for urinary tract infection (Table 2).
Multivariable Logistic Regression Analysis for the Effect of the Surgical Approach for Stone Management on Sepsis, Myocardial Infarction, Acute Kidney Disease, Transfusion, and Urinary Infection
All models are adjusted for sex, age, obesity, history of chronic kidney disease, diabetes, and prior stenting. The bold cells indicate statistically significant p-values.
OR = odds ratio.
Hospital stay, costs, mortality, and intensive care unit admission
The mean length of hospital stay was 3.9 ± 4.2 days, and the in-hospital costs were 2634 ± 2216 Euros per patient for the whole study cohort. Nevertheless, after adjusting for major baseline characteristics, the length of hospital stay was longer by 1.3 (95% CI: 1.2–1.4, p < 0.001) days and the inpatient costs were higher by 614 (95% CI: 557–671, p < 0.001) Euros after same-session bilateral ureteroscopy compared to unilateral ureteroscopy. Accordingly, 101 (1.5%) patients required postoperative intensive care unit admission after same-session bilateral ureteroscopy compared to 5293 (0.6%) patients after unilateral ureteroscopy (OR: 1.9, 95% CI: 1.6–2.3, p < 0.001). Similarly, 29 (0.4%) deaths occurred after same-session bilateral ureteroscopy compared to 683 (<0.1%) deaths after unilateral ureteroscopy (OR: 3.1, 95% CI: 2.1–4.5, p < 0.001). Therefore, in the multivariate analysis after adjusting for major baseline characteristics, same-session bilateral ureteroscopy was associated with 90% higher odds for postoperative intensive care unit admission and 210% higher odds for postoperative mortality (Table 3).
Multivariable Logistic and Linear Regression Analysis for the Effect of the Surgical Approach for Stone Management on Perioperative Length of Hospital Stay, Costs, Intensive Care Unit Admission, and Mortality
All models are adjusted for sex, age, obesity, history of chronic kidney disease, diabetes, and prior stenting. The bold cells indicate statistically significant p-values.
ICU = intensive care unit.
Discussion
The present high-volume study indicates that same-session bilateral ureteroscopy is associated with worse perioperative outcomes compared to unilateral ureteroscopy. Patients undergoing same-session bilateral ureteroscopy displayed worse baseline characteristics compared to those undergoing unilateral ureteroscopy. Nevertheless, after adjusting for these characteristics, we demonstrated that same-session bilateral ureteroscopy leads to higher rates of perioperative myocardial infarction, acute kidney disease, transfusion, urinary tract infections, sepsis, and intensive care unit admission. Accordingly, the German nationwide data from 2005 to 2021 suggest that same-session bilateral ureteroscopy increases length of hospital stay, costs, and inpatient mortality. Interestingly, the annual cases of ureteroscopy have undergone about a threefold increase in the last few years.
It seems that same-session bilateral ureteroscopy is an endourological procedure with a relatively higher complication incidence. A recent meta-analysis suggests that even though same-session bilateral ureteroscopy achieves an overall stone-free rate of 82% after surgery and 91% on the short-term follow-up, it is associated with an overall complication rate of 17%. Postoperative fever occurs in 4% of all cases, postoperative pain in 20%, gross hematuria in 4%, and other complications such as urosepsis, urinary tract infection, small mucosal laceration, stone migration, and ureteral perforation in 6% of all patients undergoing same-session bilateral ureteroscopy. 11 On the contrary, unilateral ureteroscopy is associated with an overall complication rate of about 7% and a major complication rate (Clavien–Dindo ≥ III) of about 2%. 12 Severe ureteral injury, urosepsis, and transfusion can occur in up to 2% of all cases, whereas cerebrovascular events in about 1% of all cases. 13 In the present analysis, we detected an overall mortality rate <0.1%, which is in accordance with relevant studies on the field. 14 Still, a significant increase in deaths after same-session bilateral ureteroscopy was observed with a mortality rate of 0.4% in this subset of patients. It should be highlighted that the latter is alarming for an endoscopic procedure for a benign disease. 15
In the CROES URS Global Study, 2153 patients with multiple stones underwent either unilateral (n = 1880) or same-session bilateral ureteroscopy (n = 273). Moreover, 8626 patients underwent unilateral ureteroscopy for single stones. Same-session bilateral ureteroscopy was more likely to be performed in high-volume centers, in fit patients, as well as in patients with fewer prior stone treatments. The authors demonstrated that patients undergoing same-session bilateral ureteroscopy present lower stone-free rates, higher retreatment rates, longer operating times, and prolonged hospital stay compared to patients with unilateral ureteroscopy. On the contrary, patients with single stones present the best perioperative outcomes followed by patients with multiple stones undergoing unilateral ureteroscopy. Nevertheless, the authors suggested that there is no difference in complication rates among same-session bilateral ureteroscopy, unilateral ureteroscopy, and single stone ureteroscopy, which is in antithesis with the findings of this study. 16 Accordingly, patients undergoing same-session bilateral ureteroscopy displayed in our analysis worse baseline characteristics compared to those undergoing unilateral ureteroscopy. The latter might be explained by the fact that, in-patients with multiple comorbidities, a same-session bilateral ureteroscopy can be performed in an attempt to remove all stones and to reduce the additional risks of further operations and needs for anesthesia. 17,18
It seems that the use of ureteroscopy has increased dramatically over the last years. The latter might be predominantly attributed to the fact that, in Germany, a dramatic shift from extracorporeal shockwave therapy to ureteroscopy is observed. This shift is related to the enormous technological advances of the endoscopic armamentarium. 3 Based on the previous notion, ureteroscopy is also more often preferred for middle-size renal stones compared to percutaneous lithotripsy. 19 Administrative data from the United States indicate that total ureteroscopy cases increase annually by 15%, while total extracorporeal shockwave therapy cases decline annually by about 2%. 20 The increase of annual ureteroscopy cases may be also attributed to the increase in the prevalence of urolithiasis over the last years. 21 Indeed, nationwide data from the United States suggest a 2.5-fold increase in the prevalence of urolithiasis, while for some areas, this increase might be even higher. 22
It should be highlighted that the COVID-19 pandemic negatively affected the annual ureteroscopy cases. Considering the increasing implementation of ureteroscopy for stone management, an increase in the annual ureteroscopy cases would have been expected. Still, during the COVID-19 pandemic, patients presented lower hospital admission rates, higher rates of selection of medical expulsive therapy, and lower rates of unilateral ureteroscopy. 23 Indeed, after the outbreak of COVID-19 pandemic, the Guidelines Office of the EAU published recommendations on the management of urological conditions. 24 The treatment of stones was considered an elective surgery which had to be postponed, whenever possible. Of note, in cases of infection or obstruction due to urolithiasis, placement of a stent or nephrostomy tube under local anesthesia was recommended in an attempt to prioritize the management of oncological and other emergency cases. 25 Interestingly, the annual cases of single-session bilateral ureteroscopy increased slightly during the COVID-19 pandemic, suggesting that endourologists might have attempted to treat bilateral urolithiasis in a single session to avoid unnecessary overloading of the health care system, as well as to reduce the additional risks of further operations and needs for anesthesia.
Although we performed, to our knowledge, the largest study on the field, it should be highlighted that our findings are not devoid of some important limitations that need to be underlined. The present analyses are based on retrospective, billing data, and, therefore, are prone to coding errors and misclassification. Even though these administrative data present a high degree of accuracy since they are regularly controlled by independent physician task forces, some important baseline and perioperative information are not available. Data on preoperative stone burden, stone location, urine cultures, laboratory findings, operative time, as well as short- and long-term stone free rates are not included in the GRAND database. Similarly, information on mortality and morbidity after hospital discharge, readmission and reoperation rates, effect of bilateral surgery on quality of life, and further follow-up data are also not provided in the GRAND database. Moreover, the total number of procedures and the timing between them for each patient are also lacking. Due to the lack of this information, single-session bilateral ureteroscopy could not be compared to staged bilateral ureteroscopy for stone management. Importantly, our data are restricted to Germany and, therefore, they cannot be extrapolated to other health care systems. Finally, it should be noted that the relentless improvement of instrumentation and techniques in ureteroscopy since 2005 might have affected the perioperative outcomes. Still, to overcome these limitations, our holistic approach through multiple analyses based on high-volume data may lead to solid conclusions about the negative perioperative outcomes of same-session bilateral ureteroscopy.
Conclusion
The present large-scale, real-world data demonstrate that same-session bilateral ureteroscopy increases perioperative mortality and morbidity, prolongs hospital stay, and is associated with additional perioperative costs and intensive care unit admissions compared to unilateral ureteroscopy. Interestingly, the proportion of patients undergoing same-session bilateral ureteroscopy in Germany is relatively low. Overall, the GRAND study showcases the potential harms of same-session bilateral ureteroscopy for stone management. Nevertheless, this study should be only considered hypothesis-generating due to its retrospective design and its important limitations. Therefore, further trials are needed to corroborate our findings, and clinical decision of performing same-session bilateral ureteroscopy is left to individual clinical judgment.
Footnotes
Authors' Contributions
All authors participated in the drafting, writing, and editing of the manuscript.
Ethics Statement
Written informed consent from the participants, as well as ethical approval, was not required for this study in accordance with the national legislation and institutional requirements. All data used in this work are stored anonymized at the German Federal Statistical Office.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.