
Abstract
Introduction:
Renal colic is frequently treated with opioids; however, narcotic analgesic use can lead to dependence and abuse. We evaluated use trends of opioids and nonsteroidal anti-inflammatory drugs (NSAIDs) for pain management of kidney stones in United States emergency departments (EDs) from 2015 to 2021.
Methods:
Kidney stone encounters were identified using National Hospital Ambulatory Medical Care Survey data. We applied a multistage survey weighting procedure to account for selection probability, nonresponse, and population weights. Medication use trends were estimated through logistic regressions on the timing of the encounter, adjusted for selected demographic and clinical characteristics.
Results:
Between 2015 and 2021, there were an estimated 9,433,291 kidney stone encounters in United States EDs. Opioid use decreased significantly (annual odds ratio [OR]: 0.87, p = 0.003), and there was no significant trend in NSAID use. At discharge, male patients were more likely than females (OR: 1.93, p = 0.001) to receive opioids, and Black patients were less likely than White patients (OR: 0.34, p = 0.010) to receive opioids. Regional variation was also observed, with higher odds of discharge prescriptions in the West (OR: 3.15, p = 0.003) and Midwest (OR: 2.49, p = 0.010), compared with the Northeast. Thirty-five percent of patients received opioids that were stronger than morphine.
Conclusion:
These results suggest improved opioid stewardship from ED physicians in response to the national opioid epidemic. However, regional variation as well as disparities in discharge prescriptions for Black and female patients underscore opportunities for continued efforts.
Introduction
The prevalence of kidney stones in the United States has significantly increased over the past several decades due to a confluence of factors, including an aging population, rising global temperatures, and increasing rates of obesity, diabetes, and other known risk factors. 1 Between 2012 and 2022, the overall estimated prevalence rose from 8.8% and rose to 11.0%. 2 The rising prevalence of kidney stones has resulted in an accompanying increase in emergency department (ED) visits due to renal colic. 3 Annual ED visits for suspected kidney stones have risen from ∼1 million in 2006 to 1.2 million in 2014, with current estimates as high as 2 million ED visits per year. 4,5
Patients with severe pain due to kidney stones are often treated in the ED with opioids due to their rapid onset and potent analgesic properties. 6 While opioids effectively block pain signals, nonsteroidal anti-inflammatory drugs (NSAIDs) may more effectively address the mechanism of renal colic through inhibition of prostaglandin synthesis. 7 Unlike opioids, NSAIDs decrease the release of prostaglandins, which play a significant role in the nociception and inflammation that are integral to the pathophysiology of renal colic. 8 Randomized controlled trials have indicated that patients with renal colic may have improved pain control when managed with NSAIDs, compared with opioids. 9,10
It is also well known that excessive opioid use may lead to dependence or abuse. Despite the relatively short courses of analgesia given after ED visits, opioids prescribed for acute pain in the ED still increase the likelihood of persistent use. 11,12 The risk of opioid misuse is especially salient given the ongoing epidemic in the United States that has been associated with increasing mortality across most demographic groups. 13 The rate of drug overdose deaths involving natural and semisynthetic opioids, which include drugs commonly prescribed for renal colic such as oxycodone and hydrocodone, increased more than four-fold between 1999 (1.0 per 100,000 persons) and 2016 (4.4 per 100,000 person). 6,14 This complex problem requires a multifaceted approach, and one key component is improving opioid stewardship in the ED. We aim to better understand the current trends in opioid and NSAID use for renal colic across the United States, with the ultimate goal of informing health care providers and health systems operators in their continued efforts to provide safe and effective pain management for kidney stone patients.
Methods
Data source
This study used National Hospital Ambulatory Medical Care Survey (NHAMCS) Emergency Department Public Use Data from 2015 to 2021. These data contain nationally representative samples of randomly selected ED visits from nonfederal hospitals in all 50 states and the District of Columbia. The number of hospitals participating in the survey annually ranged from 234 to 337 during the study period. 15
Encounters for kidney and upper tract stones were identified using ICD-9-CM codes 592.x and 788.0, and ICD-10-CM codes N20.x, N22.x, and N23.x. Opioids were identified using Multum therapeutic category codes 60 and 191, excluding buprenorphine, and NSAIDs were identified through codes 61 and 278. All data are deidentified and the Columbia University Institutional Review Board reviewed and approved the research design, methodology, and data handling procedures (protocol AAAQ4259).
Statistical analyses
We reported descriptive statistics for demographic characteristics, including sex, age, race, ethnicity, geographic region, and insurance status, as well as for clinical characteristics, including visit year, common comorbidities, and other hospital admission characteristics. Race, ethnicity, and region categories correspond to those reported in the U.S. Census. Descriptive statistics regarding opioid use were also calculated and stratified by place of administration (ordered in the ED vs prescribed at discharge), opioid type, and opioid strength (weaker than morphine, morphine-equivalent, or stronger than morphine) Supplementary Table S1. 16 Continuous variables were reported using medians and interquartile ranges (IQRs), and categorical variables were reported using counts and percentages.
We estimated the annual odds ratios (ORs) for medication use through logistic regression on the timing of the encounter, measured in years. All other ORs for medication use were derived from logistic regression coefficients of categorical demographic and clinical variables. Opioid use and NSAID use trends were evaluated in independent logistic regression models.
Both the descriptive statistics and medication use trends reflect national estimates and incorporated a multistage survey weighting procedure that accounted for selection probability, nonresponse, and population weights. Results were considered statistically significant with two-sided p-values <0.01, as suggested by NHAMCS to reduce the possibility of type I error when interpreting weighted survey results. 15 All analyses were conducted using RStudio (R version 4.2.2).
Results
Patient characteristics
There were an estimated 9,433,291 encounters for kidney stones in the United States between 2015 and 2021 (Table 1). The median age of patients during these encounters was 46 years (IQR: 33–59 years), with the majority between 25 and 64 years of age. The majority of patients were male (55%) and White (74%). Private insurance was the most common insurance type (42%), followed by Medicaid (19%) and Medicare (18%). While all U.S. census regions were well represented, the South had the highest number of visits (38%), followed by the West (23%). Approximately 9% of the patients were hospitalized after their ED visits, and 5% had been seen in the same ED within the previous 72 hours.
National Hospital Ambulatory Medical Care Survey Patients with Kidney Stones (2015–2021)
ED = emergency department.
Opioid and NSAID use trends
The percentage of patients who received opioids during ED encounters for kidney stones was 77% in 2015 and declined to 67% in 2021 (Fig. 1). Multivariable logistic regression adjusting for sex, age, race, ethnicity, geographic region, and insurance status demonstrated a significant decrease in the odds of opioid use over time (annual OR: 0.87, 99% confidence interval [CI] 0.76–0.98, p = 0.003).

Proportion of kidney stone encounters with opioids and NSAIDs given in NHAMCS reporting emergency departments from 2015 to 2021.
The percentage of patients who received NSAIDs during these encounters was 55% in 2015 and 62% in 2020. There was no statistically significant change over time in the adjusted odds of NSAID use (annual OR: 1.04, 99% CI 0.91–1.18, p = 0.450). Although there are conditions that may influence the use of opioids or NSAIDs for renal colic such as chronic kidney disease or gastrointestinal ulcers, hemorrhage, or esophagitis, the rates of these comorbidities are low in the NHAMCS population (3% and 0.4%, respectively) (Table 1). Furthermore, a sensitivity analysis considering chronic kidney disease as a covariate for predicting the odds of opioid and NSAID use was not significant in either model (Supplementary Table S2).
Factors associated with opioid use at discharge
The odds of opioids given at discharge also declined significantly during the study period (annual OR: 0.86, 99% CI 0.74–0.99, p = 0.005). Furthermore, there was variation in the odds of receiving opioids at discharge by sex, race, and region, which was not observed when considering opioids given at any point during the encounter. At discharge, male patients were more likely than females to leave the ED with opioids (OR: 1.93, 99% CI 1.15–3.22, p = 0.001), and Black patients were less likely than White patients to receive opioids (OR: 0.34, 99% CI 0.12–0.99, p = 0.010). Additionally, patients in the West and Midwest had higher odds of receiving opioids at discharge than in the Northeast (OR: 3.15, 99% CI 1.18–8.38, p = 0.003 and OR: 2.49, 99% CI 1.01–6.13, p = 0.010, respectively) (Table 2).
Odds of Opioids Given for Kidney Stone Encounters in the Emergency Department
CI = confidence interval; OR = odds ratio.
Factors associated with NSAID use
The odds of NSAIDs given for kidney stones were not associated with sex, race, ethnicity, region, or insurance status. Patients, 75 years of age and older were less likely to be given NSAIDs compared with the 18- to 24-year-old reference group (OR: 0.15, 99% CI 0.03–0.77, p = 0.003) (Table 3).
Odds of Nonsteroidal Anti-Inflammatory Drugs Given for Kidney Stone Encounters in the Emergency Department
Opioid characteristics
Patients with kidney stones received opioids during 68% of encounters. Among those who were discharged following their ED visit, 47% received an opioid prescription. Overall, opioids stronger than morphine were provided in 35% of encounters, morphine-equivalent strength opioids were provided in 43% of encounters, and opioids weaker than morphine were provided in only 7% of encounters (some patients received multiple types of opioids). In the ED, morphine was the most frequently used opioid (23%) followed by hydromorphone (18%) and hydrocodone (9%). At discharge, hydrocodone was the most prescribed opioid (24%), followed by oxycodone (16%) and tramadol (4%) (Table 4).
Proportion of Opioids Given by Type and Time of Dispensing for Kidney Stone Encounters in the Emergency Department
Regarding the strength of opioids given during the study period, the use of strong opioids decreased from 48% to 28% of encounters. This appeared to be partially offset by an increasing rate of intermediate-strength opioids, which rose from 22% to 37%. The proportion of patients who received weak opioids only declined slightly from 7% to 2%. The decline in strong opioid use was statistically significant and the annual OR per year mirrored the decline in overall opioid use (annual OR: 0.85, 99% CI 0.75–0.96, p = 0.001). However, the trends for intermediate-strength and weak opioids were not significant when evaluated in independent logistic regressions adjusted for sex, age, race, ethnicity, geographic region, and insurance status (Fig. 2).
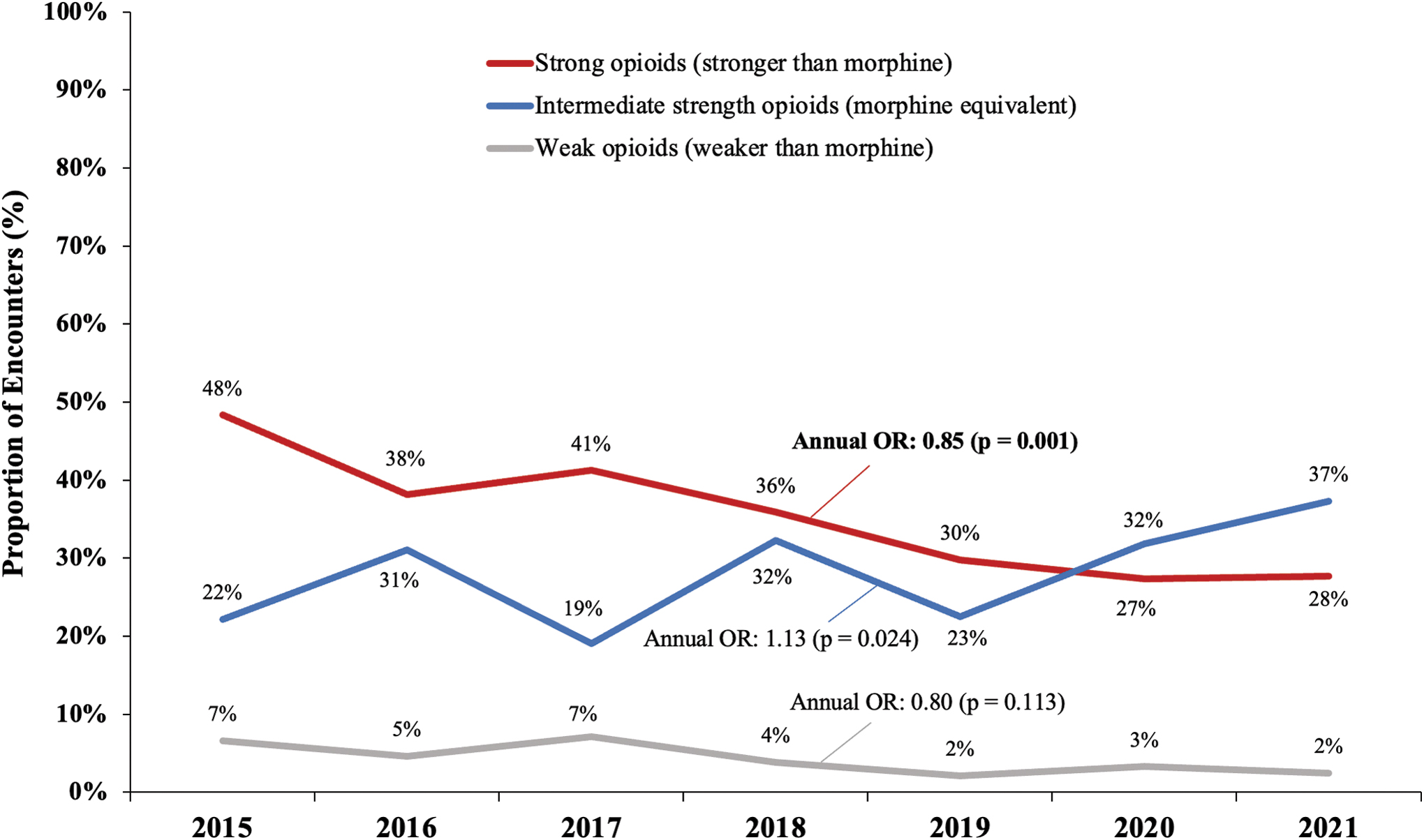
Proportion of kidney stone encounters with opioids given in NHAMCS reporting emergency departments (by strength).
Discussion
This study demonstrated a significantly decreasing trend in the annual rate of opioids used for pain management of kidney stones in U.S. emergency departments, with an absolute decline of 10% between 2015 and 2021. The rate of opioids used was lowest in 2019 (54% of encounters) and this rate rose to 67% in 2021. The observed uptick in opioid use in EDs during the COVID-19 pandemic has a variety of potential explanations, including reduced ED staff, physician burnout, and the desire for patients to pass stones at home with more potent analgesia. 17 Although there was an absolute increase in the rate of NSAID use of 7% over the same period, this trend was not statistically significant. This declining use of opioids in EDs may have been expected given the heightened focus on the opioid epidemic in recent years, however, our study does not provide evidence that NSAID use has directly offset this decrease.
These findings align with prior studies that demonstrated a decrease in opioid use for kidney stones at both the national and single-institution levels. 6,18 One of the most plausible reasons behind the recent decline in opioid use in EDs is heightened public awareness of the mortality and other harms associated with opioid misuse. 19 Opioid overdoses have claimed over 650,000 lives since 1999, starting a determined movement to curb opioid prescriptions and promote alternative pain management strategies. 20,21 Interventions such as prescription drug monitoring programs (PDMPs) and education initiatives have proliferated significantly, aimed at directly influencing prescriber behavior while concomitantly increasing providers' awareness of the issue. As of 2023, 49 states have state-wide prescription monitoring databases (with the exception of Missouri), and 45 mandate that prescribers consult PDMPs in practice. 22 Although the effectiveness of such programs is varied, one recent evaluation of Pennsylvania's PDMP on 15 EDs reported a 17.7% relative reduction in opioid prescribing rates. 23
It is difficult to directly attribute national trends to individual initiatives due to the heterogeneity of populations, health systems, and opioid policies; however, it has been shown that health care providers have been more cautious when prescribing opioids in a variety of states and clinical settings. 24
Our study also evaluated potential disparities in opioid use for renal colic based on race, sex, and other demographic characteristics. It has been established that significant disparities exist for pain management in a variety of health care settings. 25 It has been hypothesized that disparities in receiving opioids would be more pronounced at discharge than in the ED, given the higher level of trust required by physicians to send patients home with potentially addictive treatment and risk of overdosage. 26 Our study supports this hypothesis in the setting of renal colic, as female and Black patients were less likely to be prescribed opioids at discharge, compared with male and White patients.
Our study also contributes to the current understanding of regional variation in opioid use patterns for kidney stones in EDs. We found significantly greater odds of opioids prescribed at discharge in the West and Midwest regions, compared with the Northeast. The result aligns broadly with the literature that describes historically high rates of opioid prescribing in the West, South, and rural areas in general. 27 Additionally, our regional results build upon a study from Zhu and colleagues that used prior NHAMCS data and reported significantly higher rates of opioid use for kidney stones in the Midwest only. 18 Our more current data may suggest a need to refocus efforts to curb opioid prescribing in the Western United States as well as the Midwest.
Improved access to urology services and rapid primary intervention may be other viable methods to reduce reliance on narcotic pain medications for ED patients with symptomatic urolithiasis. A recent study from Abrams and colleagues found that acute renal colic patients who elected ureteroscopy as initial treatment were less likely to require narcotic prescriptions than those who attempted a trial of stone passage with or without expulsive therapy. 28 Additionally, an acute care urology service could be helpful for renal colic patients by reducing the time to consult and intervention, and by improving postoperative outcomes. 29 By accelerating definitive intervention, the need for prolonged analgesics can be reduced and improve the quality of life of stone formers.
Our study has several limitations. First, as with any retrospective cohort study, there may be unobserved variables that influence a patient's likelihood of receiving opioids or NSAIDs. For example, NHAMCS did not collect medical or surgical history, such as prior kidney stones, recent stone removal procedures, or substance use disorders. Another limitation of NHAMCS's cross-sectional nature was that we were unable to evaluate the long-term efficacy of pain medication or readmission. Additionally, NHAMCS data collection practices may vary from year to year. The COVID-19 pandemic posed unique challenges in 2020 such as delays in data collection and a reduced response rate. 30 Also, patients could have up to 3 additional diagnosis codes associated with a particular ED visit. Although renal colic from stones is generally considered to be one of the most painful presenting conditions, NHAMCS does not explicitly indicate which specific diagnosis is associated with pain medication. Finally, this study relied on reported ICD codes and Multum drug codes; any errors in data collection would diminish the reliability of the results.
Conclusions
The decreased use of opioids, and strong opioids in particular, for kidney stone patients presenting to the ED from 2015 to 2021 displays improved opioid stewardship from ED physicians. These results align with ongoing national efforts to curb opioid prescribing in the United States in response to the epidemic. However, regional variation, as well as disparities in prescriptions at discharge for Black patients and female patients underscore opportunities for continued efforts.
Footnotes
Acknowledgments
An earlier version of our abstract with data from 2015 through 2020 was published in: Abstracts of the 40th World Congress of Endourology: WCE 2023. Journal of Endourology 2023;37(S1):A1–A422; doi: 10.1089/end.2023.36001.abstracts.
Authors' Contributions
R.B.B.: Methodology, data curation, statistical analysis, and writing (original draft). J.V.: Methodology, data validation, and writing (original draft). E.J.M.: Conceptualization, methodology, data validation, and writing (reviewing and editing). A.B. and J.L.: Data validation and writing (reviewing and editing). O.S.: Conceptualization and writing (reviewing and editing).
Author Disclosure Statement
There are no conflicts of interest relevant to this study. O.S. is a member of the advisory boards for Ambu, Boston Scientific, and Coloplast. He is also a lecturer for Coloplast. A.B. is a consultant for Johnson & Johnson.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Tables S1
Supplementary Tables S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.