
Abstract
Introduction:
To analyze the influencing factors of ureteral stenosis after ureteroscopic holmium laser lithotripsy.
Methods:
The clinical data of 427 patients treated with ureteroscopic holmium laser lithotripsy were selected, and the patients were divided into two groups based on the presence or absence of ureteral stenosis after the operation. Univariate and multivariate logistic regression were used to analyze the independent risk factors for postoperative ureteral stenosis, and R software and regression coefficients were used to construct a predictive model.
Results:
After a 1-year follow-up of 427 patients, 28 patients (6.56%) developed ureteral stenosis; univariate analysis showed that the occurrence of ureteral stenosis after subureteral holmium laser lithotripsy was related to stone diameter, stone incarceration, degree of hydronephrosis, holmium laser injury of mucosa, and operation time (p < 0.05); further logistic regression analysis showed that a large stone diameter, stone incarceration, and moderate to severe hydronephrosis were independent risk factors for ureteral stenosis after ureteroscopic holmium laser lithotripsy (p < 0.05); According to H-L deviation degree and area under receiver operating characteristic curve test, the results show that the model has high accuracy (χ 2 = 2.475, p = 0.613) and differentiation (0.875 [95% confidence interval or CI: 0.817–0.919]), and the external verification of the nomogram prediction model was carried out by the verification group. The results showed that the prediction probability of the calibration curve was close to the actual probability and had a good consistency (area under the curve: 0.873 [95 CI: 0.822–0.914]).
Conclusion:
The established nomogram model exhibits high accuracy and discriminative ability. It can effectively identify high-risk groups, enabling timely prevention of ureteral stenosis and minimizing the risk of postoperative ureteral stenosis.
Introduction
As a disease secondary to nephrolithiasis, ureteral calculus has an incidence second only to nephrolithiasis. 1 Small ureteral stones can be treated conservatively or removed via drug therapy, whereas those with big diameter, especially obstructive stones, demand surgical intervention as early as possible. 1 –3 Continuous development of medical technology allows widespread clinical use of holmium laser. With small tissue penetration and high lithotripsy efficiency, it can treat ureteral calculi in different sites and with different compositions, which is currently an effective treatment choice for urinary calculi. 4 Nevertheless, at present, ureteral stricture is a common complication after holmium laser lithotripsy, which may lead to nephrectomy or renal failure in severe cases. 5,6 Hence, by investigating the factors influencing ureteral stenosis after ureteroscopic holmium laser lithotripsy and constructing a risk prediction model, it is possible to help clinically assess the occurrence risk of ureteral stenosis and reduce its incidence.
Data and Methods
Data
A total of 427 patients who underwent ureteroscopic holmium laser (Holmium [Ho:YAG] laser therapy machine, raykeen) treatment at The First Affiliated Hospital of Shaoyang University between February 2018 and December 2021 were retrospectively analyzed. This group of patients served as the modeling group for constructing a column chart prediction model for postoperative stenosis. Additionally, 183 patients treated with holmium laser under ureteroscopy in our hospital from December 2021 to December 2022 were collected as the validation group for external validation of the model. Modeling group patients were divided into two groups according to whether ureteral stenosis occurred 1 year after operation. There were 296 males and 131 females; body mass index was 20.45 to 27.52 kg/m2, with an average of (23.78 ± 2.14) kg/m2; aged 22 to 75 years, the patients had an average of (48.67 ± 4.21) years. Information was collected to understand the patient’s stone treatment history, previous medical history, and whether there was fever before operation. Urinary CT, intravenous pyelography, X-ray, and ultrasonography were performed before operation to understand whether the patient was complicated with hydronephrosis and to assess the patients’ urinary anatomy, stone number, size, and position. Routine laboratory tests were performed before operation, including serum creatinine, routine urine analysis, and complete blood count. If the patient’s urine test indicates leukocytosis, mid-segment urine can be collected for culture, and antibiotics can be used for 1 to 3 days as preventive treatment. Subsequently, a reexamination is performed, and the operation can be scheduled if the leukocyte count decreases significantly or returns to normal levels. Inclusion criteria: (1) all patients underwent holmium laser lithotripsy for the first time; (2) the patients have complete relevant information and are informed about the research content; and (3) patients with ureteral calculi who meet the indication of holmium laser lithotripsy have large calculi, distal urinary tract obstruction, and lower calyceal calculi. Exclusion criteria: (1) patients complicated with malignant tumors, liver and kidney dysfunction, and immune system diseases; (2) patients with indwelling ureteral stents; (3) patients complicated with history of ureteral operation, ureteral polyps, kidney stones, and previous history of ureteral stenosis; (4) patients with ureteral strictures as suggested by preoperative examination; and (5) patients with accidental injury during operation. This study protocol was approved by The First Affiliated Hospital of Shaoyang University. The case collection flow chart is shown in Figure 1.

Case collection flow chart.
Methods
The patients had a light diet 1 to 2 days before operation, fasted food and water on the day of operation, maintained adequate sleep, completed routine examinations such as chest X-ray, electrocardiogram, routine urine, blood, and liver and kidney function, and excluded surgical contraindications. The surgeon has more than 10 years of surgical experience, the operation was performed under general anesthesia, the lithotomy position was taken, and the Wolf 8/9.5F ureteral sheath was placed under direct vision of the urethra to find the ureter on the affected side. The ureteroscope (guided by the guidewire) was smoothly advanced into the renal pelvis, with the guidewire left in place in the renal pelvis. Subsequently, the ureteroscope was withdrawn. The 14/12F ureteral sheath (Jiangsu Yikai Medical Device Co., Ltd.) was placed along the guide wire, the guide wire and sheath core were withdrawn, and then the flexible ureteroscope was placed along the channel to search for calculi, and a 200 μm holmium laser fiber was inserted into it to nibble the calculus. For slightly larger stones post-holmium laser lithotripsy, stone fragments were retrieved using a stone basket. Set the laser frequency to 10 to 15 Hz, energy crushing 1.5 to 2.0J, and power 20W. After checking that there is no stone residue in all fields of view, the guide wire can be inserted, the flexible ureteroscope is withdrawn, and the ureter is checked for mucosal perforation, tear or avulsion, and so on 16 F). In the process of lithotripsy, multiple stones or larger stones were clamped out using ureteral stone forceps, and small stones were flushed out using physiologic saline. After the stone fragmentation, the Double-J tube was indwelled for 2 to 3 weeks to link the bladder and kidneys, relieve hydronephrosis, and prevent ureteral stenosis.
Indexes
The clinical information and basic data were collected and compared, including patients’ disease course, weight, gender, age, operation time, holmium laser injury of mucosa, hydronephrosis, stone size, incarceration of stones, stone clearance rate, and incidence of stent-related urinary tract symptoms.
Evaluation criterion
Hydronephrosis status was judged according to urinary CT scan and Color Doppler ultrasonography results. If the kidney has no abnormal shape, with normal renal parenchyma thickness and echo, and the renal collecting system is separated by 2 to 3 cm, it can be judged as mild hydronephrosis; if the renal column is unclearly displayed, the renal parenchyma gets thinner, with kidney increased in volume and pelvis was separated by 3 to 4 cm, showing serious expansion, it can be judged as moderate hydronephrosis; if the renal column has radial echoes, the pelvis was separated by more than 4 cm, the renal parenchyma is obviously thinned, and the regional position is a liquid dark area, showing increased kidney volume and abnormal shape, it can be judged as severe hydronephrosis. The manifestation of incarcerated ureteral calculi is that the contrast agent cannot pass through the obstruction site during X-ray urography, and the area below the obstruction site does not develop normally. The occurrence of incarcerated calculi can be confirmed by ureteroscopy or surgical treatment.
Follow-up visit
Patients with ureteral calculi were followed up for 1 year using methods such as telephone inquiry, outpatient follow-up, and medical record inquiry. The occurrence and recurrence of ureteral stenosis were recorded. Color Doppler ultrasonography examination was required on the 1st day, 2nd week, 1 month, 3 months, 6 months, and 12 months after the removal of the Double-J tube. Imaging examinations such as ultrasonography, urological CT, and specialized urological tests (e.g., retrograde urography and intravenous urography) were performed to identify any aggravation of hydronephrosis. These tests helped rule out other potential causes, and if no other cause was found, the aggravation of hydronephrosis was attributed to ureteral stenosis, confirming it as postoperative ureteral stenosis.
Statistical analysis
SPSS 20.0 software was used to analyze the research data. The count data were expressed as (n, %), and the chi-square (χ
2) test or Fisher’s exact test was performed; the measurement data were expressed as mean ± standard deviation (
Results
Incidence of ureteral stenosis
After 1-year follow-up visits, 28 (6.56%) out of 427 patients developed ureteral stenosis, that is, the stricture group. There were 8 cases of upper ureter stenosis (28.57%), 11 cases of middle ureter stenosis (39.29%), and 9 cases of lower ureter stenosis (32.14%). The remaining 399 cases were of the nonstenosis group.
Univariate analysis
Univariate analysis was performed on the two groups. According to the result, the occurrence of ureteral stenosis after ureteroscopic holmium laser lithotripsy is related to stone diameter, calculus incarceration, hydronephrosis degree, holmium laser injury of mucosa, and operation time (p < 0.05), as shown in Table 1.
Univariate Analysis of the Influencing Factors of Ureteral Stenosis after Subureteral Holmium Laser Lithotripsy
Multivariate logistic analysis of factors influencing ureteral stenosis after subureteral holmium laser lithotripsy
According to univariate analysis results, logistic regression analysis was performed using stone diameter, calculus incarceration, hydronephrosis degree, holmium laser injury of mucosa, and operation time as independent variables. It was found that large stone diameter, calculus incarceration, moderate to severe hydronephrosis are independent risk factors influencing ureteral stricture after ureteroscopic holmium laser lithotripsy (p < 0.05). Formula: −0.780 + (1.762 × Stone diameter 1–2 cm/(1.798 × Stone diameter >2 cm) + 2.019 × Stone entrapment + (1.959) × Moderate hydronephrosis/(3.461) × Severe hydronephrosis) as shown in Table 2.
Multivariate Logistic Regression Analysis
CI, confidence interval; OR, odds ratio.
Establishment of nomogram risk prediction model
A nomogram was constructed with stone diameter, calculus incarceration, and hydronephrosis degree as variables, and a model was built using R software, as shown in Figure 2. The score of each risk factor was assessed in light of the nomogram rating scale. The nomogram scale label corresponding to the sum of each score was taken as the risk occurrence index.
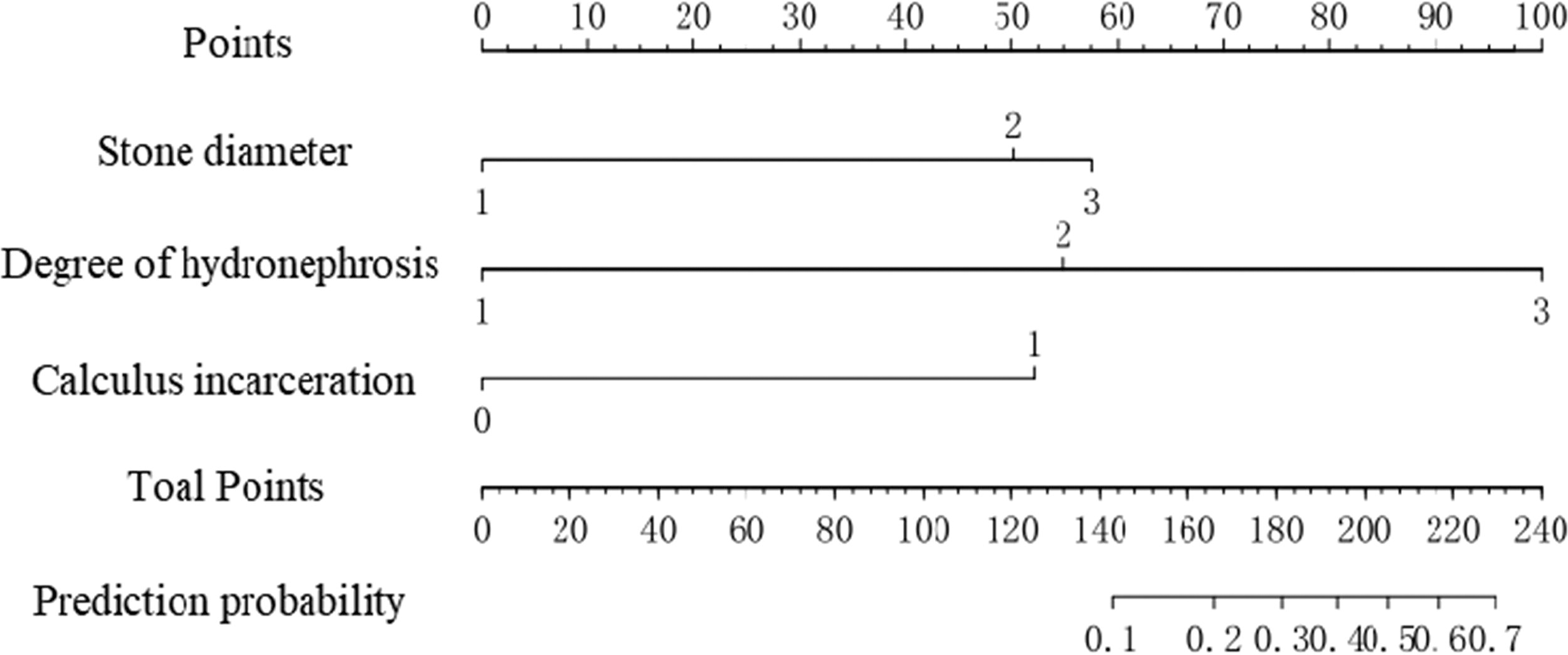
Risk prediction model for ureteral stenosis after ureteroscopic holmium laser lithotripsy.
Example of how to use the nomogram: If a patient has a preoperative stone diameter of 2 cm (50 points), calculus incarceration (52 points), and moderate hydronephrosis (55 points), the sum of the corresponding scores is 157 points, and the corresponding risk index is 0.15.
Internal validation of a risk prediction model for ureteral stenosis after holmium laser lithotripsy under ureteroscopy
Bootstrap method was used to verify the prediction model internally, and the H-L test results were χ2 = 2.475 and p = 0.613. The model had a good calibration degree, and the calibration curve showed a good consistency between the risk predicted by the column chart and the actual risk. The area under ROC curve was 0.875 (95% confidence interval or CI: 0.817–0.919), and the prediction model had good differentiation, as shown in Figure 3.

Internal validation of the nomogram prediction model.
External validation of a risk prediction model for ureteral stenosis after holmium laser lithotripsy under ureteroscopy
Among the 183 cases in the validation group, there were 13 cases of concurrent stenosis and 170 cases of nonconcurrent stenosis. Compared with the nonconcurrent stenosis group, the concurrent group had a higher proportion of stones with a diameter >2, stones with incarceration, and moderate to severe hydronephrosis, as shown in Table 3. The column chart prediction model was externally validated with the validation group population, and the results show that χ2 = 10.041, p = 0.262, the slope of the calibration curve approaches 1, and the predicted probability of the calibration curve is close to the actual probability with good consistency, as shown in Figure 4A. The area under the curve is 0.873 (95% CI: 0.822–0.914), indicating that the prediction model has good discrimination, as shown in Figure 4B.

External validation of the nomogram prediction model.
Comparison of Clinical Data Between the Validation Group and the Nonstenosis Group
Fisher’s exact test.
Discussion
Holmium laser represents a new technology extensively used in clinical treatment of ureteral calculus. Boasting excellent lithotripsy ability, it can pass the generated energy through optical fiber, transmit the vaporized energy to the stone, and then vaporize the stone into particles, which can efficiently crush stone of various compositions. 7,8 At present, ureteral stenosis is one severe complication after ureteroscopic holmium laser lithotripsy. If the risk of ureteral stenosis can be accurately predicted, the curative effect can be significantly improved, thus reducing patients’ economic burden and cutting medical expenses. 9 –13 Hence, this study investigates the risk factors in occurrence of ureteral stricture after ureteroscopic holmium laser lithotripsy, constructs a risk prediction model to provide a basis for the early clinical identification and timely intervention of high-risk cases.
After 1-year follow-up visits, it was found that 28 (6.56%) out of 427 patients developed ureteral stricture, higher than 1.50% in Darwish et al., 14 which may be related to the selection of sample size. This study is a single center study, and some results may deviate from big data results. Univariate and multivariate analysis of the included patients showed that stone diameter, stone impactivity, and degree of hydronephrosis were the influencing factors of ureteral stricture after ureteroscopic holmium laser lithotripsy, consistent with the research results of Darwish et al. and Shen et al. 15 The possible reason is that patients with calculus incarceration are prone to ureteral mucosal edema, so safety guide wire easily penetrates the mucosa, resulting in mucosal bleeding, infection, scarring, and loss, which in turn triggers ureteral stenosis. In addition, the ureteral wall in patients with calculus incarceration may have accompanying urothelial hyperplasia, edema, and interstitial fibrosis, which aggravates calculus incarceration, restricts stone movement, thereby increasing the lithotripsy difficulty and the risk of wall loss. The long-term incarceration of large-diameter stones in the ureter can stimulate mucosal edema and congestion, leading to fibrous tissue hyperplasia and inflammatory polyps. The above pathological changes will deteriorate under ureteroscopy, thereby contributing to ureteral stenosis. 9,16
The nomogram can transform the complex regression equation into a visual graph, make the prediction model simple and clear, and facilitate the risk assessment. 17 A nomogram model was established based on the influencing factors screened by multivariate analysis. Later, ROC curve and H–L goodness-of-fit test were performed to test the nomogram built herein. The verification results show that the predicted value is basically consistent with the measured value (Fig. 3), finding that stone diameter, calculus incarceration, and hydronephrosis degree have high reliability and validity as predictor variables. In practice, the sum of risk factor scores can be used to assess the occurrence risk of ureteral stricture after ureteroscopic holmium laser lithotripsy. This model can help patients undergoing ureteroscopic holmium laser lithotripsy to effectively prevent the risk of ureteral stricture and reduce its incidence.
In conclusion, the stone diameter, calculus incarceration, and hydronephrosis degree are independent risk factors for ureteral stenosis after ureteroscopic holmium laser lithotripsy. The nomogram model established based on these results has high accuracy and differentiation, allowing for the effective identification of high-risk groups, provision of timely prevention, and minimizing the risk of postoperative ureteral stenosis. Nevertheless, the sample size included in this study is small, so the incidence of ureteral stenosis may be different from some cognition. Additionally, this study did not analyze factors such as multiple ureteral calculi, renal function, calculus composition, and hydronephrosis complications. Therefore, long-term research is needed to further study these influencing factors and provide more reliable results.
Footnotes
Authors’ Contributions
P.L.: Data collection and article writing. K.W.: Data collection and article writing. L.L.: Data collection. Q.X.: Data collection. Y.W.: Data analysis. Q.L.: Project development, data collection, data analysis, and article editing.
Consent for Publication
All authors give consent for publication.
Ethical Approval
This retrospective study involving human participants was in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by The First Affiliated Hospital of Shaoyang University’s ethics review board (2020055).
Data Availability Statement
The datasets used to support the findings of this study are included within the article.
Author Disclosure Statement
All authors have no conflict of interest.
Funding Information
This work has been supported by