
Abstract
Background:
The narrower focal zone (FZ) size of modern lithotripter was considered as one of the factors that resulted in suboptimal treatment result of extracorporeal shockwave lithotripsy (SWL). Therefore, we investigate the efficacy and safety of standard narrow or extended (FZ) sizes in SWL for patients with renal stones.
Materials and Methods:
In this prospective study conducted between April 2018 and October 2022, patients with renal stones were randomized to receive SWL with either standard or extended FZ. Treatment was delivered using a Modulith SLX-F2 lithotripter with a maximum of 3000 shocks at 1.5 Hz. The primary outcome was treatment success 12 weeks after a single SWL session, defined as the absence of a stone or stone fragment <4 mm on computed tomography. Secondary outcomes included the incidence of perinephric hematoma, stone-free rate (SFR), and changes in the urinary levels of acute renal injury markers.
Results:
A total of 320 patients were recruited, and 276 patients were randomized into the two groups. The two groups had similar baseline parameters. The treatment success rate was significantly better for standard FZ (74.3%) than the extended FZ group (59.3%) (p = 0.009). Standard FZ also had a significantly better SFR (Grade-A, 36.8% vs 23.0%, p = 0.013) and less pain after treatment. Both groups had similar perinephric hematoma formation rates, unplanned hospital admission rates, and changes in urinary acute renal injury markers.
Conclusions:
The standard narrow FZ has better treatment efficacy and similar safety compared with the extended FZ during SWL for renal stones. This clinical trial has been registered in the public domain (CCRBCTR) under trial number CUHK_CCRB00510.
Introduction
Extracorporeal shock wave lithotripsy (SWL) was introduced in the early 1980s to manage urolithiasis. With the advantage of being minimally invasive, SWL remains one of the treatment options for renal stones <2 cm in guidelines. 1
In the initial report of the machine HM3, the treatment success rate was ∼90%. 2 However, electrohydraulic shockwave generation would lead to shot-to-shot variation 3 and result in a wider focal zone (FZ) (90 × 15 mm). In addition, there is a need for frequent changes of electrodes because of their short lifespan. Therefore, the latest lithotripters used electromagnetic generators, which relied on the vibration of thin metallic membranes for shockwave production. This is not only more durable (no need to change frequently) but also provides more constant output and a narrower FZ, which may result in less surrounding tissue damage.
Unfortunately, the performance of new lithotripters has never reached that of HM3. There were many potential factors in those new lithotripters that could account for the suboptimal performance, including the use of dry coupling, faster shockwave delivery rate, usage of sedoanalgesia for pain control, and so on. 4 The narrower FZ size was also one of the proposed reasons for this. The potential mechanisms of wider FZ for better treatment results include a better squeezing effect on stones by shockwave in larger FZ 5 and allowance for wider error margin for stone targeting. 6,7 Moreover, the higher peak pressure related to narrower FZ has been shown to cause more intense renal injury in animal models. 8 Therefore, some urologists proposed a shift back to wider FZ generators. 3,5
Modulith SLX-F2 is a lithotripter that tries to incorporate the advantages of HM3 and newer-generation lithotripters. Besides its modular design and dual imaging system, the machine provided two predesigned FZ sizes: a standard (28 × 6 mm, narrower) and an extended (50 × 9 mm, wider) (Table 1) This allows the operator to select the FZ size during SWL. 2 The wider FZ delivers the same energy amount with a lower peak pressure. This unique feature of the machine provides an ideal platform for comparing different FZ sizes in stone fragmentation, as other parameters of lithotripters will be controlled.
Comparison of the Specification of HM3 and Modulith SLX-F2 System
Therefore, a prospective study was performed to evaluate the effect of the two FZ sizes on the treatment outcomes of renal calculi, including both treatment success and related renal injury.
Materials and Methods
Trial design
This randomized parallel-group study assessed and compared the efficacy and safety of two different FZ sizes for treating renal stones after one SWL section. The study complied with the Declaration of Helsinki and ICH-GCP principles.
Participants and eligibility criteria
Patients with renal stones who planned to undergo primary SWL at our center were recruited for this study.
The following inclusion criteria were applied: Patients aged ≥18 years. Solitary radio-opaque renal stone with a maximal diameter of 5–15 mm.
The following exclusion criteria were also applied:
Patients with multiple renal calculi within the same calix.
Stones associated with any renal or ureteral anatomical abnormality.
Stones previously treated by other management.
Patients with a ureteral stent or nephrostomy tube within 3 months of SWL.
Patients with a history of cystine stones.
Interventions
After informed consent, each patient underwent pretreatment noncontrast computed tomography (NCCT) to confirm the stone location. Patients who met the eligibility criteria were then randomized in a 1:1 ratio to receive treatment with one of the FZ sizes:
Standard group: Treated with narrower FZ—size is 28 × 6 mm, peak pressure 150 MPa.
Extended group: Treated with wider FZ—size is 50 × 9 mm, peak pressure 90 MPa.?
Before SWL, a spot urine sample was collected for the baseline measurement of acute kidney injury (AKI) markers. Patient-controlled analgesia (PCA) system, using intravenous alfentanil was used during SWL. All treatments were delivered at 1.5 Hz. After initial low energy ramping for 100 shocks, treatment was given at energy level 6 for a maximum of 3000 shocks unless the stone could not be localized or the patient could not tolerate the procedure.
After SWL, treatment parameters were recorded. The pain experienced by patients would be assessed at the end of treatment using a verbal analogue scale (0–10 scale). Spot urine samples were again collected for the measurement of urinary markers.
Patients were then reviewed on day 2, 6 and 12 weeks. MRI or NCCT (for patients unsuitable for MRI study) were performed on day 2 to assess any hematoma formation after SWL. Fresh morning spot urine samples were collected for AKI markers during each follow-up. Plain radiography was carried out at 6- and 12-week follow-ups to monitor treatment outcomes. NCCT was performed at 12 weeks to document stone clearance if suggested by plain radiography.
Measurement of urinary markers
The collected spot urine samples were used for the evaluation of acute renal injury markers, including N-acetyl-β-
Main outcome measures
The primary outcome measure was defined as either a stone-free state or the presence of clinically insignificant residual fragments (smaller than 4 mm) as assessed by NCCT performed 12 weeks after a single session of SWL. The secondary outcome measures included the stone-free rate (SFR; Grade-A), the incidence of renal hematoma formation after SWL and unplanned hospital admission, changes in the urinary levels of AKI markers, and so on.
Sample size
In a preliminary study, 50 patients with renal stones 5–15 mm in size were randomized to standard and extended FZ. The treatment success rate at 3 months for standard and extended FZ was 76% and 60%, respectively. The success rate for standard FZ was comparable with our voltage ramping study (74%), which used a similar setting in the control arm. 11 The difference in the success rate of the two FZs was also comparable with a report from the Canadian group, with a 69.2% success rate in standard FZ and 57.1% in extended FZ. 12 Therefore, using our data for the sample size calculation, we estimate that 288 patients would be needed to provide a power of 80% with a two-tailed significance level of 5%. With an additional consideration of ∼10% screen failure and dropout rate, the proposed sample size would be 320.
Randomization, allocation concealment mechanism and implementation
An independent statistical staff generated the randomization list with assistance from a computer program. A permuted block design with random block sizes of 2 and 4 was used. The random allocation sequences were placed in identical preset numbered envelopes. After confirming a subject's eligibility, the on-duty urologist would perform randomization by opening the consecutively numbered, identical preset envelope before starting treatment.
Blinding
A designated team of urologists and radiologists blinded to the treatment assignments were responsible for all follow-up care, including imaging assessments. The laboratory staff members were also blinded to the intervention assignments. Treatment allocation was maintained by only independent statistical staff members who prepared the randomization list and data analysis. These staff were not involved in data collection or patient care.
Statistical methods
The analysis was conducted on an intention-to-treat basis to evaluate the differences between the two FZ groups. Where appropriate, continuous data were compared using Student's t-test or Mann–Whitney U-test. Categorical variables were compared using the chi-square test or Fisher's exact test as appropriate. Logistic regression was used to assess the effects of various predictive factors on treatment success rates. Changes in urine marker levels over time were evaluated using generalized linear mixed models with the log link function. In addition to the trial group, time, and their interaction, the models included age, body mass index, stone size, stone site, and Storz medical lithotripsy index (SMLI) as fixed effects. All data were analyzed using SPSS Statistics, version 28.0 (SPSS, Inc., Chicago, IL). A two-tailed value of p < 0.05 was considered statistically significant.
Results
From April 2018 to October 2022, 320 patients were recruited for the study. Of these, 289 patients fulfilled all inclusion criteria and were randomized into one of the two groups. However, 13 patients' stones could not be localized during treatment, and finally, 276 patients received treatment as planned. Figure 1 presents the CONSORT flow chart of the study.

CONSORT diagram of the study.
The patient's clinical characteristics and stone parameters are listed in Table 2. There were no significant differences between the groups in the baseline parameters. There was also no significant difference in treatment energy and time for the two groups. However, there was a significantly lower end-of-treatment pain score for the standard group compared with those in the extended group, whereas the analgesic consumption during treatment was similar for the two groups (Table 3).
Demographic and Stone Characteristics of the Subjects
BMI = body mass index; IQR = interquartile range; SD = standard deviation.
Treatment Parameters of the Two Groups
SMLI was designed by STORZ MEDICAL for the measurement of the total applied energy during shockwave therapy.
SMLI = Storz Medical Lithotripsy Index.
The overall treatment success and Grade-A SFR were 66.8% and 29.9%, respectively. The corresponding rates were 74.3% and 36.8%, respectively, in the standard group and 59.3% and 23.0%, respectively, in the extended group. The standard (narrower) group has significantly better treatment success and SFR than the extended group. As expected, the standard group (7.4%) also has significantly less secondary intervention than the extended group (16.8%) (p = 0.017) (Table 4).
Treatment Outcome and Complication Rates of the Two Groups
SFR = stone-free rate.
Cross-sectional imaging on day 2 after SWL revealed that 33.6% and 33.1% of patients in the standard group and extended group, respectively, developed perinephric hematoma, a significant difference (p = 0.932). The standard and extended groups had two and four symptomatic hematomas, respectively. All cases were managed conservatively. Both groups had similar unplanned hospital admission rates; most complaints were Clavien Grade 1–2 (Table 4).
A multivariate analysis was performed to assess the factors related to the treatment outcomes of SWL. Here, FZ size and stone size were the only identified predictors of treatment success, with standard FZ size and smaller renal stones associated with a better treatment success rate (Table 5).
Logistic Regression for Treatment Success and Stone Free
SMLI—a measurement of the total energy administrated during lithotripsy.
CI = confidence interval; LC = lower calices.
Both groups exhibited significant increases in all the urinary AKI markers. However, no intergroup differences were observed in any urinary marker level (Table 6 and Fig. 2). The levels of all markers returned to the baseline at 6 weeks after SWL.
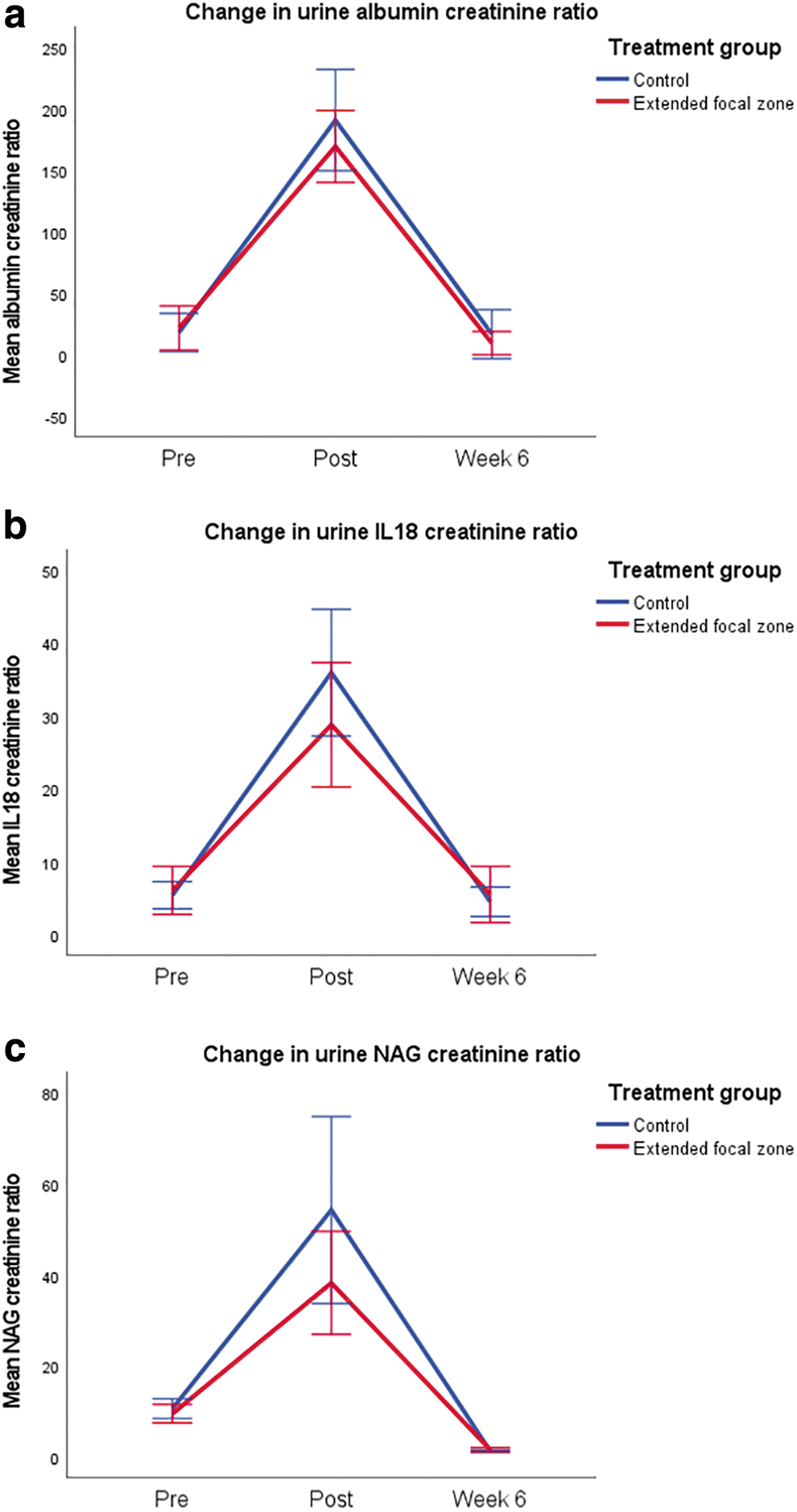
The change in urine marker levels over time
Changes in Urine Marker Levels in Patients
Mean changes were estimated from generalized linear mixed models with the log link function. In addition to the trial group, time, and their interaction, the models included age, BMI, stone size, stone site, and SMLI as fixed effects.
FZ = focal zone; IL = interleukin; NAG = N-acetyl-β-
Discussion
In this study, we evaluated the effect of different FZ sizes on the outcomes of SWL for renal stones. Our results indicate that patients treated with a standard (smaller) FZ have better treatment success rates than those treated with an extended one. It also causes less pain at the end of treatment, with no difference in complication rate or renal injury compared with the extended one. These results reassured us that the current trend of using smaller FZ sizes for SWL is both effective and safe for our patients.
As discussed previously, narrow FZ size was one of the suspected reasons for the lower efficacy of newer lithotripters compared with the HM3 machine. In a previous study comparing the treatment outcome of modified HM3 and Modulith SLX-F2, using the extended FZ, there was no difference in SFR for renal stones, which suggests that extended FZ could help to improve the treatment outcomes. 13 However, there are other technical differences in machine parameters between the two lithotripters, such as the coupling and localization systems, which would also affect the treatment efficacy. As a result, we could not simply conclude that the comparable treatment success rates of Modulith SLX-F2 and modified HM3 supported the benefit of extended FZ.
The unique feature of having dual FZ sizes of Modulith SLX-F2 machine could provide an ideal platform for comparison of different FZ sizes in stone fragmentation, as other parameters of lithotripters (such as coupling system, energy output per shock) were controlled. A previous report from Canadian urologists (in the abstract) compared the outcomes of two different FZs. 12 Surprisingly, the preliminary result was similar to our study: extended FZ had poorer SFR at 3 months (57.1%, compared with standard FZ, 69.2%; p = 0.042). Therefore, our study confirmed the standard (smaller) FZ has better treatment outcomes for renal stones than the extended FZ, with no increase in complication rate.
Besides treatment outcomes, the effect of FZ size on kidney injury is also controversial. During the earlier development of SWL, there were concerns about the wide FZ of HM3, which might lead to more kidney injury. For example, in a study comparing the effect of SWL by HM3 and Lithostar plus (a machine with a narrower FZ), there was a significantly higher urinary level of AKI markers in patients treated with HM3. 14 On the contrary, in another in vivo study, a narrower FZ machine (Modulith SLX, an earlier model of Modulith SLX-F2) produced more severe tissue damage than HM3. Histologically, porcine kidneys treated by HM3 only had a diffuse interstitial hemorrhage. But for those kidneys treated by Modulith SLX, there was also near-complete tissue disruption devoid of histologically recognizable kidney structure. 8 In another ex vivo study using Modulith SLX-F2 to treat porcine kidneys, vascular and parenchymal tissue injuries were again observed in the focused areas, 15 although less severe than in the previous article. Nevertheless, no difference in the size of vascular lesions was noticed between kidneys treated by standard or extended FZ. 15
Although it would be difficult to have a histological assessment of our subjects after SWL, we have a comprehensive renal injury assessment, including post-treatment cross-sectional imaging, serial urinary AKI markers, and clinical evaluation for adverse complications. Our results showed that a smaller FZ did not increase perinephric hematoma formation and AKI markers. In addition, the unplanned hospital admission rate of the two groups was comparable. The observed hematoma incident was comparable with the literature and our previous report and was mainly related to using more sensitive cross-sectional imaging for the assessment. 11,16 Fortunately, only six patients (two from standard FZ and four from extended FZ) had symptoms necessitating admission, and all were managed conservatively.
In a recent study with a similar study design, comparing the treatment outcome of narrow and broader FZ in a piezoelectric lithotripter, the result showed both narrow and wider FZ had similar treatment results. 17 However, the overall SFR was assessed after three sessions of treatment. If we based on the SFR after the first treatment session, the narrow FZ has a numerically better result (79.2%) than the wider FZ (69.1%). Therefore, this also suggested that a narrow FZ might have better treatment results, as in our study. However, besides the higher peak pressure, there may be other possible mechanisms resulting in better treatment outcomes for the narrower FZ, which will need further investigation in future.
We also observed that the end-of-treatment pain score was statistically higher in the extended FZ group (Table 3). We initially postulated this might be owing to more tissue being affected during treatment by the wider FZ and, hence, more pain experienced. However, in the above-mentioned study by Noureldin et al., patients experienced less pain when treated by the extended FZ. 17 We did not understand the difference, and further studies might be needed to assess this outcome.
One main limitation of our study was that stone analysis results were unavailable in our patients, as many did not collect their stone fragments for analysis. However, as the total sample size comprised >270 cases, we assumed the distribution of stone composition should be balanced in the two groups. The overall SFR of our studies seems to be lower than the literature. 17 However, we used NCCT for treatment assessment, and only those with no stone fragment seen were considered stone free, this might explain the lower SFR of our study. However, our treatment success rate, which included stone-free and residual fragments <4 mm in size, was comparable with the other studies. 12,17 The study period was long (4 years) because of the COVID pandemic effect. However, the team managing the patients remained the same, and the assessment and management were consistent throughout the study period.
Conclusion
In this randomized study of SWL for treating renal stones by Modulith SLX-F2 lithotripter, we observed that a narrow FZ could provide better stone treatment results than the extended FZ, with no increase in complication rate.
Footnotes
Acknowledgments
The authors thank the nursing and radiographers at Lithotripsy and Uro-investigation Centre, Prince of Wales Hospital, Shatin, Hong Kong, China, for supporting this study.
Authors' Contributions
The article have been read and approved by all the authors, and all the authors have made a substantial contribution to the article's information. Concept and supervision: C.-F.N. Protocol development: C.-F.N. and S.C.H.L. Data collection: C.F.N., C.H.Y., J.Y.C.T., P.K.F.C., A.W.Y.K., B.S.Y.L., W.K.T., and W.C.W.C. Data analysis: C.F.N., S.C.H.L., A.W.Y.K., and B.S.Y.L. Article drafting: C.-F.N., S.C.H.L., and A.W.Y.K. Article review: all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by the Hong Kong RGC Research Matching Grant Scheme 8601454 and 8601526.