
Abstract
Objectives:
The super-pulsed thulium fiber laser (SP TFL) is a new alternative to high-power holmium laser for intracorporeal lithotripsy. The SP TFL has shown advantages in dusting regimes, but benefits in fragmentation regimes are less understood. The second-generation SP TFL introduces an advanced fragmentation pulse (AFP) sequence to maximize SP TFL’s efficiency in fragmentation. This study evaluates safety and efficacy of the SP TFL fragmentation mode in ureteroscopy (URS) and mini percutaneous nephrolithotomy (mini-PCNL).
Materials and Methods:
The study was conducted in two phases. Safety of a new AFP was compared ex vivo to standard SP TFL fragmentation settings by measuring the dimensions of wounds created in porcine kidney after laser exposure for 0.5, 1.0, and 2.0 s. The resulting wounds were evaluated histologically using nitro blue tetrazolium chloride (NBTC) stain. In the clinical phase, the second-generation SP TFL was used to fragment and extract ureteral and renal stones in 40 patients using ureteroscopic and percutaneous approaches. The stone size, volume, density, laser-on-time, and total energy were recorded for each patient. In addition, the chemical composition, ablation rate, and ablation efficiency were assessed for each stone treatment.
Results:
The ex vivo mucosa damage profiles caused by AFP were similar to those caused by regular pulses. In clinical phase, the median volume and density for ureteral stones were 0.4 cm3 and 1029 Hounsfield units (HU), for renal stones 1.3 cm3 and 1113 HU, respectively. Different stone types were crushed into fragments suitable for extraction. The mean AFP energy was 3 J and the average power for ureteral stones was 10.5 W, whereas for renal stones it was 28.5 J and 31 W, respectively. The overall complication rate was low in both groups.
Conclusion:
ST PFL with AFP capability facilitates effective fragmentation of ureteral and renal stones of any composition during URS and mini-PCNL with minimal complication rates.
Introduction
Numerous innovations in the endourological management of urolithiasis have led to complete replacement of shock-wave lithotripsy with modern laser-assisted intracorporeal stone treatment via either ureteroscopic or percutaneous (PERC) approach. 1,2 This paradigm change has been enabled by the introduction into the mainstream clinical practice of the holmium yttrium-aluminum garnet laser (Ho:YAG) and the miniaturization of endo-ureteroscopic instruments.
Almost two decades ago, advent of Ho:YAG laser has shifted the stone-treatment strategy in the stone management from the pure fragmentation to either fragmentation or dusting of the stone. 2 Stone dusting became very popular during the ureteroscopy (URS) saving the cost for baskets and decreasing the morbidity because of the absence of the fragments extractions. 3
The introduction of the new technology, the super-pulsed thulium fiber laser (SP TFL), manifested appearance of a viable alternative to the current gold standard of the Ho:YAG laser. 4 –7 As 2018, numerous preclinical and clinical studies have shown that compared to the Ho:YAG laser, the SP TFL provides 1.5–4 times faster stone ablation and 2–4.5 times lower retropulsion, 4 –12 especially in the dusting regimes of operation. There are also discerning reports, such as e.g., paper by Haas et al. 13 showing that there is no significant difference between the laser time for pulsed-modulated Ho:YAG with Moses 2.0 and SP TFL. It must be noted that the selected optimal modes for the Ho:YAG laser do not coincide with the optimal modes of SP TFL for dusting and fragmentation regimes. SP TFL is becoming very popular, also because of its size and low initial and maintenance costs.
However, the Ho:YAG laser is known for efficient fragmentation of stones into large fragments, and the advantages of the SP TFL are less obvious in this area. The fragmentation regimes are important when performing PERC laser stone treatment for kidney stones (standard PERC and mini-PERC), ureteroscopic management of impacted large ureteral stone burden (URS), and cystolithripsy for bladder stones. Some studies have reported that the TFL stone fragmentation of large stones is either inferior or comparable to the holmium devices in terms of outcomes and operations times. 2,14 To ameliorate this drawback in the TFL-assisted lithotripsy, a novel SP TFL (FiberLase U-MAX, IPG Medical, Marlborough, MA, US and they subsidiary IRE-Polus Ltd., Fryazino, Russia) has been developed. This new laser system has the ability to modulate the laser pulse (Advanced Fragmentation Pulse [AFP]). AFP represents a train (sequence) of sub-pulses. The exact number of sub-pulses as well as amplitudes of individual sub-pulses depend on selected pulse energy. AFP has been optimized for efficient stone fragmentation. Advanced features of this laser system, such as possibility to change the pulse shape and sequence and duration in wide ranges make it possible to introduce an optimized and personalized stone treatment. It refers to the adjustment of the pulse settings after endoscopic stone visualization and observation of the surrounding mucosa.
The aim of this study was to evaluate the novel pulse-shaping modes of the SP TFL in terms of feasibility, efficacy and safety in fragmentation of ureteral and renal stones during ureteroscopic and PERC intracorporeal lithotripsy.
Materials and Methods
Ex vivo safety testing
Freshly excised porcine kidney samples were cut into 20 × 25 × 8 mm blocks. The blocks were placed in water bath at 37°C. SP TFL exposures were performed using the settings summarized in Table 1. For all settings, the average laser power was maintained at ∼10 W for 365 µm fiber (ureteral stones, semi-rigid scope) and ∼30 W for 550 µm fiber (kidney stones, percutaneous nephrolithotomy [PCNL] scope). Exposures were performed in quasi-contact (∼0.5 mm) mode with the fiber oriented normally to tissue surface, simulating worst-case scenario of accidental exposure of mucosal wall during lithotripsy. Exposure times were 0.5, 1, and 2 seconds 15 for all samples. All experiments were done in triplicate. Immediately after exposure, the tissue was cut, using cryotome (3550 Technical, Genelabotech, China) and stained with nitro blue tetrazolium chloride (NBTC) stain (Sigma-Aldrich, USA). Histology slides were evaluated using lab microscope (ADF D 450, Dmicro, Russia).
The Super-Pulsed Thulium Fiber Laser Settings Used in Ex Vivo Phase
Study population and procedures
A prospective single center trial has been conducted for 46 patients between June 2022 and January 2023. We excluded six patients who had multiple calculi, upper tract anomalies, active urinary tract infection, or to whom endourological operation was contraindicated or the extraction alone had been sufficient. Only patients for whom laser lithotripsy was recommended per clinical guidelines were included. Thus, 40 patients were undergoing either ureteroscopic (URS) or PERC (mini-PCNL) management with laser lithotripsy (SP TFL FiberLase U-MAX IPG Medical, Marlborogh, MA, US and their subsidiary IRE-Polus Ltd., Fryazino, Russia). The study protocol has been approved by the local Ethics Committee. During the recruitment, we collected the following patient data: age, sex, and stone parameters (size, side, location, density) obtained from low-dose non-contrast CT scan in bone window 354–1800 HU. Stone volume was estimated using the formula of an ellipsoid (4/3 × π × radius length × radius width × radius depth) and stone density was measured in Hounsfield units (HU). The inclusion criteria were single stone, signed informed consent, ability, and willingness to present for 1-month follow-up evaluation.
All cases were carried out under general anesthesia. The procedures were performed using a standardized technique as previously described. 9 Therefore, with the exception of the laser modality, all other steps were the same. For ureteral calculi, when the stone was reached with semi-rigid ureteroscope (8F Karl Storz®, Germany), laser lithotripsy was performed if the stone was considered too large for direct extraction with a grasper. At the end of the procedure, URS JJ-stent has been placed for 1 month because of the mucosal changes at the location of the stone. Urethral catheters have been removed in 1–2 days postoperatively.
Minipercs were done under general anesthesia, in supine position and the puncture was done by the standard technique under fluoroscopy guidance. MIP L Miniperc instrument (19.5 F, Karl Storz®) was used and the tract was dilated with the single-shot 23/24 F dilation system. The stone was fragmented with SP TFL.
Fragments were evacuated by vacuum cleaner effect or (infrequently) with a grasper. At the end of the procedure, a thorough visual inspection by the nephroscope was performed of all the calyces to confirm residual fragments. Fluoroscopy was done to further confirm the absence of residual fragments. At the end of the procedure, we placed a nephrostomy tube for 1–2 days routinely. Ureteral and urethral catheter have been removed on the following day after intervention.
For irrigation purposes constant 0.9% saline irrigation pressure (40 cm H2O) at ambient temperature and a manual pump (Traxerflow Dual Port®, Rocamed®, Monaco) have been used. All the interventions were done by an experienced endourologist, who had previous experience in laser lithotripsy for at least 5 years. Lithotripsy was performed by the SP TFL, using laser fibers of 550 μm for renal stones and of 365 μm for ureteral stones. The tip of the laser fiber was cut off (not stripped), to eliminate the distal transparent part, at the beginning of every procedure.
TFL: Operative settings and lasering technique
During the URS procedure for all ureteral stones, the novel AFP laser mode with an average power of 10.5 W and the pulse total energy of 3 J were used. At the Miniperc for all renal stones, the novel AFP laser mode with an average power of 31 W and the pulse energy of 28.5 J were used. Stone fragmentation was considered to be the splitting of the stone into fragments, which was determined by the access used. So for ureteral stones, the size of the fragments did not exceed 4 mm, and for kidney stones it was no more than 7 mm. For achieving fragmentation we used the following technique: We kept the distance between the laser fiber and the stone at 0.5 mm continuously and sent to one point of the stone from 1 to 3 modulated laser pulses and then moved the fiber by 0.5–1 .0 mm laterally. Thus, we achieved a complete split of the stone into fragments. Also, we maintained a safe distance between the tip of the laser fiber and the endoscope within 3–5 mm.
Outcomes measurements
For laser lithotripsy efficacy, we estimated the efficiency (in mm3/J) by dividing the pre-operatively estimated stone volume by the total amount of energy delivered by the SP TFL. The ablation rate was calculated as the stone volume divided by the laser-on time (LOT). LOT, which was automatically recorded by the laser system, was the total time that the laser was emitting energy. The chemical composition of the stone fragment was determined in the CMD laboratory (Moscow, Russia), using infrared spectroscopy. Complications were classified according to the Clavien–Dindo classification. 16
Results
Ex vivo tests
NBTC-stained cross-sections of the wounds produced ex vivo by SP TFL operating in AFP and regular modes are shown in Figure 1A, B. The corresponding measurements of the cut depth and coagulative margins are presented in Figure 1C, D. Table 2 shows p values between the AFP and the regular modes across different laser settings for a given exposure time and fiber diameter.
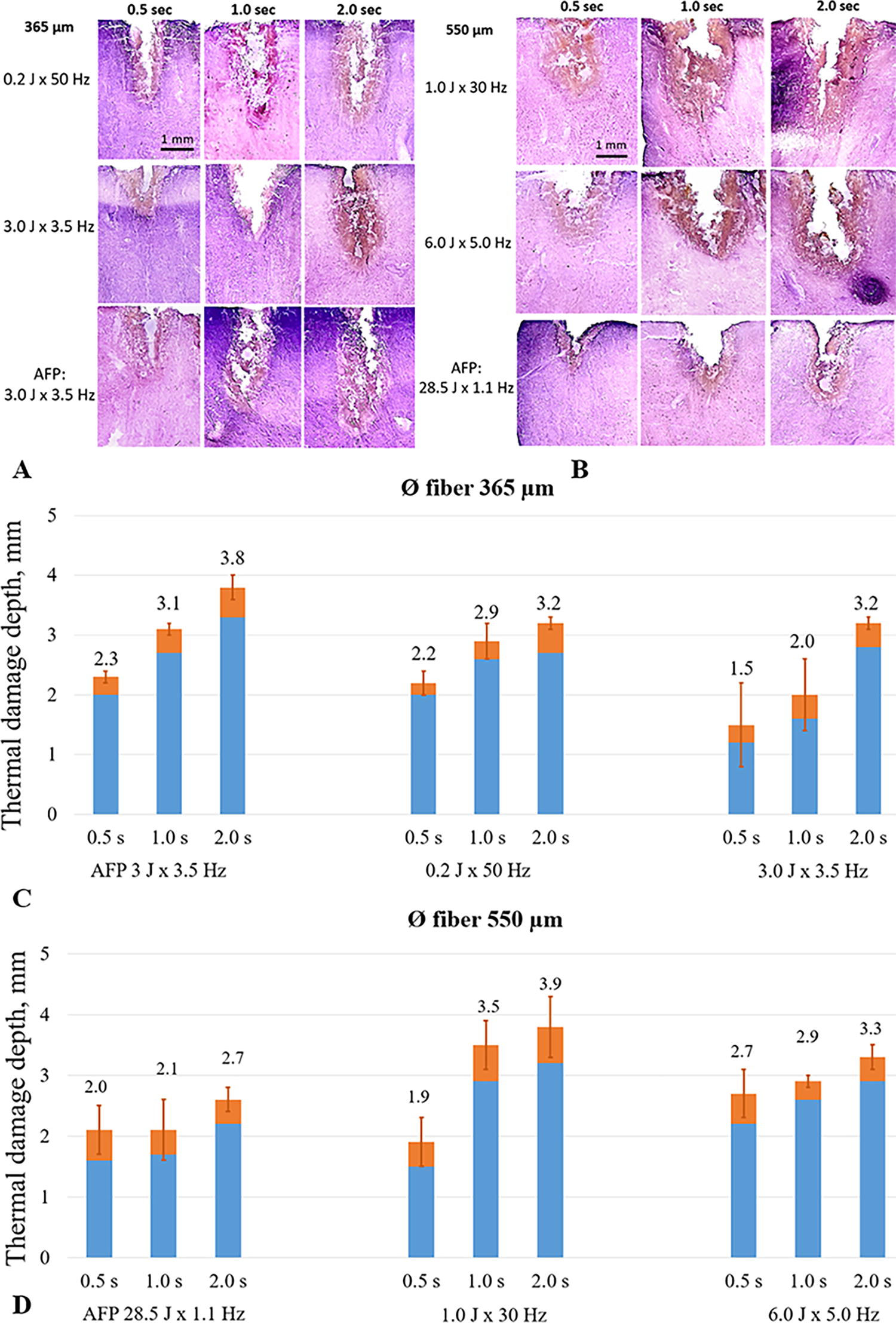
Ex vivo safety testing.
P-Value Between the AFP and the Regular Modes Across Different Laser Settings for a Given Exposure Time and Fiber Diameter
AFP, advanced fragmentation pulse.
Clinical phase
For the clinical phase, patient demographics and stone data are shown in Table 3. Median (interquartile range [IQR]) age for patients with ureteral stones was 53 (19–82) years and for patients with renal stones was 51 (23–74) years. Most patients had age-related Charlson comorbidity index score grade 1 or 2. Median (IQR) stone volume for ureteral stones was 0.4 (0.1–1.8) сm3, and for renal stones, it was 1.3 (0.2–5.1) сm3. Median (IQR) stone density for ureteral and renal stones was 1029 (354–1800) HU and 1113 (390–1700) HU, respectively. The chemical composition of stones in ureter and kidney was of a mixed composition, so the stone was classified as the type that was dominant, that is, its percentage was more than 50. Therefore, all stones were calcium oxalate 20 cases, carbapatite 14 cases, uric acid 5 cases, and brushite −1 case. Case examples for laser settings in ureteral and kidney stones are shown in Figures 2 and 3, respectively. SP TFL study outcomes and postsurgery complications are summarized in Table 4.
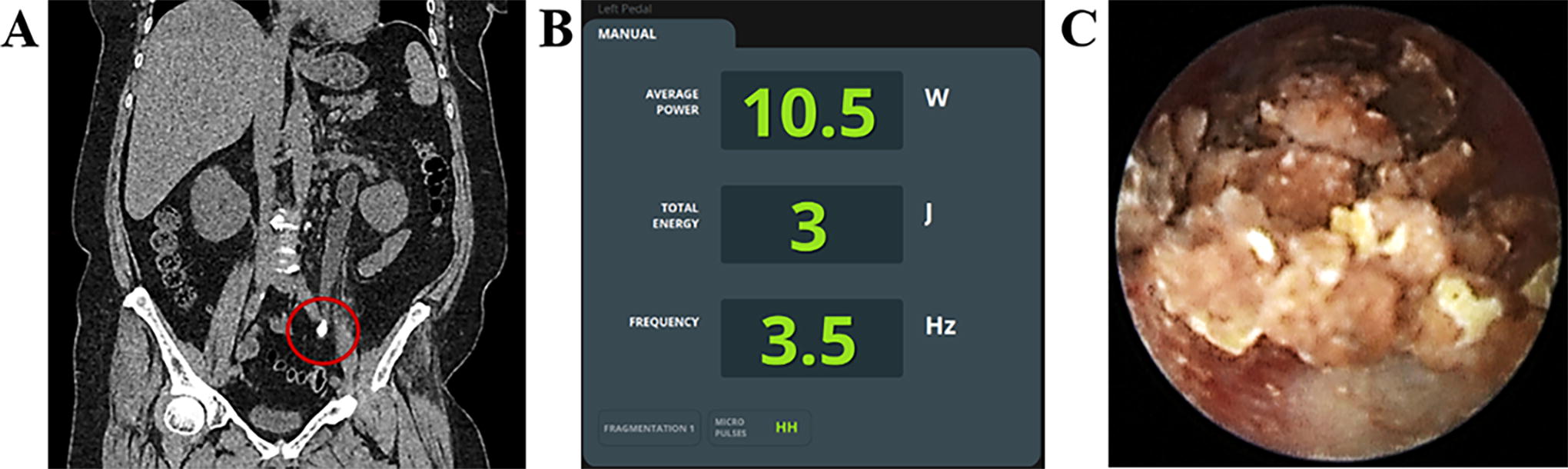
Ureteral stone laser settings example.
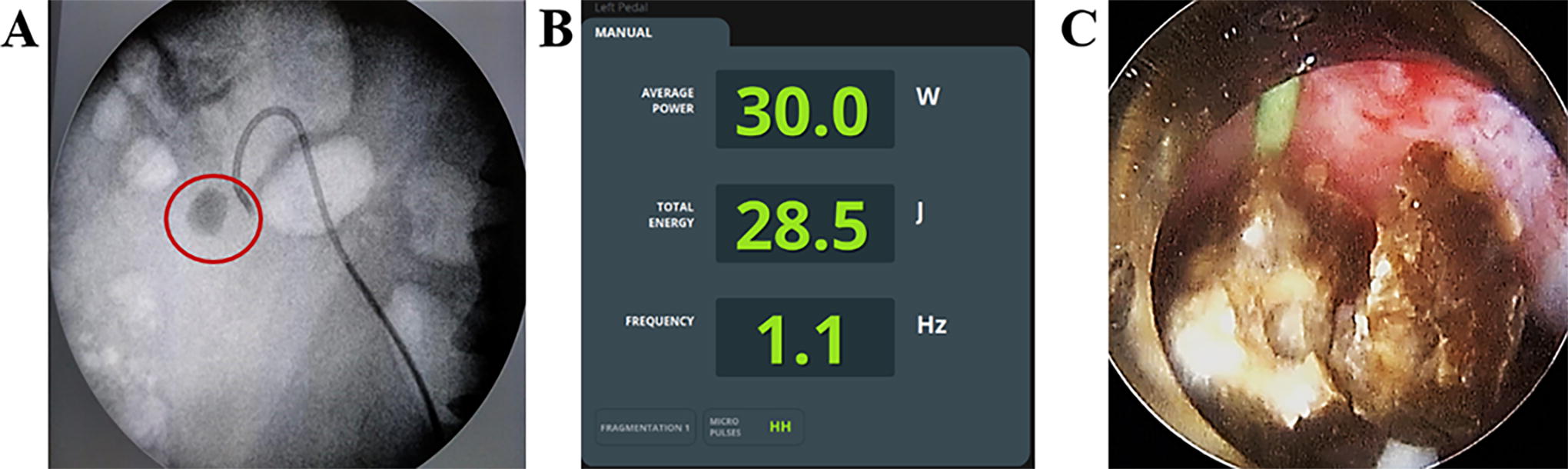
Kidney stone laser settings example.
Demographics of the Study Population and Stone Characteristics
CCI, Charlson comorbidity index; IQR, interquartile range.
Clinical Phase Outcomes
IQR, interquartile range.
Fragmentation to fragments suitable for extraction was achieved in all cases. Median (IQR) LOT for ureteral stones was 2.4 (0.1–8.2) minutes and for renal stones was 4.5 (0.2–19.4) minutes. The median (IQR) amount of total energy for ureteral and renal stones was 1.6 (0.1–5.2) kJ and 8.2 (0.4–35.8) kJ, respectively. Median (IQR) ablation efficiency was 0.5 (0.1–2.5) mm3/J for ureteral stones and 0.3 (0.1–0.8) for renal stones. Median (IQR) ablation rate was 5.6 (1.1–28.8) mm3/s for ureteral stones and 8.0 (1.3–28.3) for renal stones. The differences in the ablation efficiencies and ablation rates between ureteral and renal stones most likely are explained by the differences in hardness (median 1029 vs median 1113, respectively; see Table 2) and chemical composition of the stones between the two locations. Complications analyzed by the Clavien–Dindo classification system were similar and relatively low in both groups. In one URS case, there was a need for JJ-stent change because of its abnormal function after operation and fever. In the second group, there were 4 cases of prolonged fever, which have been conservatively managed. In one case, after mini-PNL we have placed JJ-stent after removal of nephrostomy tube. In the second group, there were no hemoglobin drop after mini-PCNL. There were no either inadvertent urinary wall perforation or fragment migration in either group.
Discussion
To investigate and mitigate safety risk introduced by the novel AFP with high energy settings sequence, an ex vivo study was conducted on a fresh porcine kidney to assess the depth of ablation and of the thermo-damage zone for the new fragmentation modes (see Table 2 and Fig. 1). It should be noted that this test was performed for the most dangerous case, when the fiber is in quasi-contact and at a normal incidence angle to the tissue. The results show that for 550 µm fiber no significant differences were found between the AFP and “the worst” regular pulses of the same average power (p > 0.05) at exposure time 0.5 second, but the difference was significant for exposure times up to 1 and 2 seconds (p < 0.05). At the same time, for 365 µm fiber no significant differences were found between the AFP and “the worst” regular pulses of the same average power (p > 0.05) at exposure time up to 1 second, but significant differences were observed at exposure time 2 seconds (p < 0.05). Based on the literature data, 17,18 the typical wall thickness of the ureter and renal pelvis is 4.0 and 2.9 mm, respectively. Thus, with exposures at relevant laser settings up to ∼2 seconds (even in the case when the depth of thermal-damage zone for AFP exceeds the depth of regular pulse) for both 365 µm and 550 µm fibers, there should be no perforation of the wall of either ureter or renal pelvis, respectively. Hence, these optimized regimes appear to be safe for fragmentation of ureteral and renal stones. We have also observed the absence of upper urinary tract perforations during the clinical study. Further clinical trials with the new pulse sequences are necessary to confirm the preliminary results obtained in this initial experience.
During many years, Ho:YAG laser lithotripsy has been the gold standard of the intracorporeal lithotripsy. The main reason for its dominance was its ability to effectively fragment and dust all stones types by means of small core diameter laser fiber. 19 This enabled the rise of the role of the endourology in the management of urolithiasis.
Majority of the studies show SP TFL is twice superior in dusting mode for urinary stones when compared to the best Ho:YAG laser. However, the Ho:YAG laser is known 20 for an efficient fragmentation of stones into large fragments (overwhelming majority of Ho fragments are <4 mm for all compositions). Until now, the benefits of SP TFL in the fragmentation mode were questionable. Fragmentation mode is important when performing either the PERC treatment for the kidney stones or during URS for impacted ureteral stones or cystolithoripsy for bladder stones. To ameliorate this aspect of TFL technology, a new SP TFL capable of emitting optimized AFP has been developed. This clinical study demonstrates that the efficacy and safety of the new fragmentation modes of SP TFL are comparable or better than the respective indicators of Ho:YAG laser, obtained from the analysis of published literature. 17
The main limitation of our study is that it contains two clinically different groups. Therefore, we avoided to provide direct statistical comparison between the two groups. The obtained results clearly showed the feasibility to provide pure and fast large size fragmentation in different stone types during either URS or PERC stone management. The possibility of laser pulse modulation led to the high efficacy in terms of ablation speed for all stone types.
In all cases, large fragments were removed or evacuated with fluid stream and underwent subsequent analysis.
There were also no cases of laser induced retrograde migration during the ureteroscopic fragmentation. In the second group, SP TFL fragmentation mode did not cause either ureteral or calyceal migration.
Conclusion
The novel SP TFL makes it possible to successfully fragment ureteral and renal stones of any chemical composition during endourological stone management with minimal complication rate. Optimized fragmentation laser pulse shape and sequences with high energy setting make this laser a promising alternative to the Ho:YAG laser for fragmentation. Further clinical trials with the new pulse sequences are necessary to confirm the preliminary results obtained in this initial experience in comparison with Ho:YAG laser.
Ethical Statement
Informed consent was obtained from all individual participants involved in the study. This article describes study involving human participants that was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Footnotes
Authors’ Contributions
A.M.: Protocol development, data collection and management, article writing—editing. M.A.: Data collection and management. A.A.: Data collection and management. G.A.: Protocol development, data analysis, article writing—editing. I.Y.: Protocol development, data analysis, article writing—editing. A.K.: Protocol development, data analysis, data collection, article writing—editing. V.A.: Protocol development, data analysis, article writing—editing. O.B.: Data collection and management. O.T.: Protocol development, data analysis, article writing—editing.
Author Disclosure Statement
The authors declare that they have no conflict of interest; however, O.T. consults for Karl Storz, Coloplast, IPG photonics, Ambu, Quanta System, and Rocamed. G.A., I.Y., and A.K. are employees of IPG Medical. V.A. and O.B. are employees of NTO “IRE-Polus.”
Funding Information
Provided by NTO “IRE-Polus,” Fryazino, Russia.