
Abstract
Purpose:
We herein describe the superficial preprostatic vein (SPV) anatomy and determine its relationship with the accessory pudendal artery (APA).
Materials and Methods:
We reviewed 500 patients with localized prostate cancer who underwent conventional robot-assisted radical prostatectomy between April 2019 and March 2023 at our institution. SPV was defined as “any vein coming from the space between the puboprostatic ligaments and running within the retropubic adipose tissue anterior to the prostate toward the vesical venous plexus or pelvic side wall.” While APA was defined as “any artery located in the periprostatic region running parallel to the dorsal vascular complex and extending caudal toward the anterior perineum.” The intraoperative anatomy of each SPV and APA was described.
Results:
SPVs had a prevalence rate of 88%. They were preserved in 252 men (58%) and classified as I-, reversed-Y (rY)-, Y-, or H-shaped (64%, 22%, 12%, and 2%, respectively) based on their intraoperative appearance. Overall, 214 APAs were found in 142 of the 252 men with preserved SPV (56%; 165 lateral and 50 apical APAs in 111 and 41 men, respectively). SPVs were pulsatile in 39% men perhaps due to an accompanying tiny artery functioning as a median APA. Pulsations seemed to be initially absent in most SPVs but become apparent late during surgery possibly due to increased arterial and venous blood flow after prostate removal. Pulsations were common in men with ≥1 APA.
Conclusions:
This study, which described the anatomical variations in arteries and veins around the prostrate and their preservation techniques, revealed that preserving this vasculature may help preserve postprostatectomy erection.
ClinicalTrials:
The Clinical Research Registration Number is 230523D.
Introduction
A superficial preprostatic vein (SPV) often runs between the puboprostatic ligaments (PPLs) 1 within the retropubic adipose tissue anterior to the prostate. The anatomical variations of SPVs were first reported by Myers and classified into four types: a single midline superficial vein without bifurcation (60%); a single midline superficial vein with bifurcation to the right or left pelvic sidewall (20%); anomalous superficial vein (10%); and no superficial vein (10%). 2
During radical retropubic prostatectomy (RRP), SPV is usually secured and ligated to maintain hemostasis. However, in robot-assisted radical prostatectomy (RARP), SPV can be preserved because of the delicacy and specificity of the robotic instruments. In the conventional RARP used in our study, SPV and the accessory pudendal artery (APA) are preserved to maintain circulation in the corpus spongiosum (Fig. 1). We found that some SPVs pulsate because of the presence of a tiny artery, considered to be a median APA (Supplementary Fig. S1). SPV facilitates venous drainage of the penis and possibly arterial supply to the corpus spongiosum via the median APA. APA and SPV preservation may prevent postoperative vasculogenic erectile dysfunction in neurovascular bundle (NVB)-sparing cases. 3 –6 Aside from Myers' report, SPV research is scarce. 2 This study aims to reveal SPV anatomy and its relationship with APA through robotic surgery observations. We also report our SPV preservation technique.

Preservation of SPV and APAs. rY-shaped SPV and two lateral APAs
Materials and Methods
Men with localized prostate cancer (n = 500) underwent RARP at the Itabashi Chuo Medical Center (Tokyo, Japan) between April 2019 and March 2023. Six-port transperitoneal conventional RARP was performed using the da Vinci Surgical System (Intuitive Surgical, Inc., Mountain View, CA) (Table 1). We defined SPV as “any vein coming from the space between PPLs and running within the retropubic adipose tissue anterior to the prostate, toward the vesical venous plexus or pelvic side wall,” 2 and APA as “any artery located in the periprostatic region running parallel to the dorsal vascular complex (DVC) and extending caudal toward the anterior perineum.” 7,8
Conventional Robot-Assisted Radical Prostatectomy Procedures Used in This Study
APA = accessory pudendal artery; EPF = endopelvic fascia; NVB = neurovascular bundle; SPV = superficial preprostatic vein.
We routinely removed all retropubic adipose tissue after developing the retropubic (Retzius) space and identified all SPVs and APAs above or under the endopelvic fascia (EPF) or near the pubic ramus. We incised or cut EPF, PPLs, and DVC and examined APAs running below EPF or around the prostatic apical region. SPV was routinely preserved. Some SPVs were torn and could not be preserved completely due to their venous fragility. All grossly visible APAs were preserved.
The clinical anatomy of APAs and SPVs was documented intraoperatively, and digitalized operative videos were reviewed retrospectively to confirm our intraoperative findings. We summarized the anatomy of each SPV, including shape, and APA, including laterality, side, size, and distribution. 9 Furthermore, we investigated the presence of pulsation in SPVs and its correlation with the number of APAs.
Lateral APAs course along the anterolateral aspect of the prostate, either in intimate contact with the anterolateral prostatic surface or closer to EPF, a few millimeters away from the gland. Apical APAs are localized inferior and lateral to PPLs, close to the anterolateral aspect of the prostatic apex, and emerge through the levator ani muscle fibers, approaching the prostatic apex. 8,10 The size of each APA was classified depending on its intraoperative appearance. We were unable to investigate APA origins because this area was not routinely developed during our RARP except in cases with extended pelvic lymph node dissection.
The protocol for this research project was approved by the ethics committee of our institution (approval No. 230523D). Experiments were conducted in accordance with the 2013 revision of the Declaration of Helsinki. Informed consent to participation and publication was obtained from all participants before study commencement.
Binomial and chi-square tests were used to evaluate deviations and differences in categorical and continuous variables. Analyses were performed using R (version 4.0.5) and R studio (version 2022.12.0 + 353). p-Values of <0.05 were considered statistically significant.
Results
Seven men were excluded from the study because of incomplete data. SPVs were present in 432 men (88%; 95% confidence interval [CI] 84–90) and preserved in 252 (58%). These had a median age of 68 (45–81) years and were retrospectively reviewed in this study.
Superficial preprostatic veins
Table 2 summarizes the anatomical variations of SPVs. In our series, SPV origins were located above the anterior wall of DVC. 11 SPV can be completely preserved during the cutting and suturing of DVC (Supplementary Fig. S2). SPV is unlikely to be a superficial branch of DVC but may provide supplemental venous drainage of the corpora cavernosa, which differs from the DVC drainage system. 5,12 –14
Anatomical Variations of Superficial Preprostatic Vein and Accessory Pudendal Artery
rY = reversed-Y.
We identified four types of SPV based on their intraoperative appearance: I-, Y-, reversed-Y (rY)-, and H-shaped (Figs. 2 and 3). The most common type was I-shaped SPVs (64%; 95% CI, 58–70). This is a single midline vein arising from the space between PPLs and entering the vesical venous plexus or pelvic side wall. I-shaped SPVs have no bifurcation anterior to the prostate and give off a small branch to the anterior bladder neck (Fig. 4). The second most common type was rY-shaped SPVs (22%; 95% CI, 18–28). This is an I-shaped SPV with late bifurcation into two branches above the bladder neck. As in I-shaped SPVs, these two branches often give off further tiny branches to the anterior bladder neck and enter the vesical venous plexus or pelvic side wall.
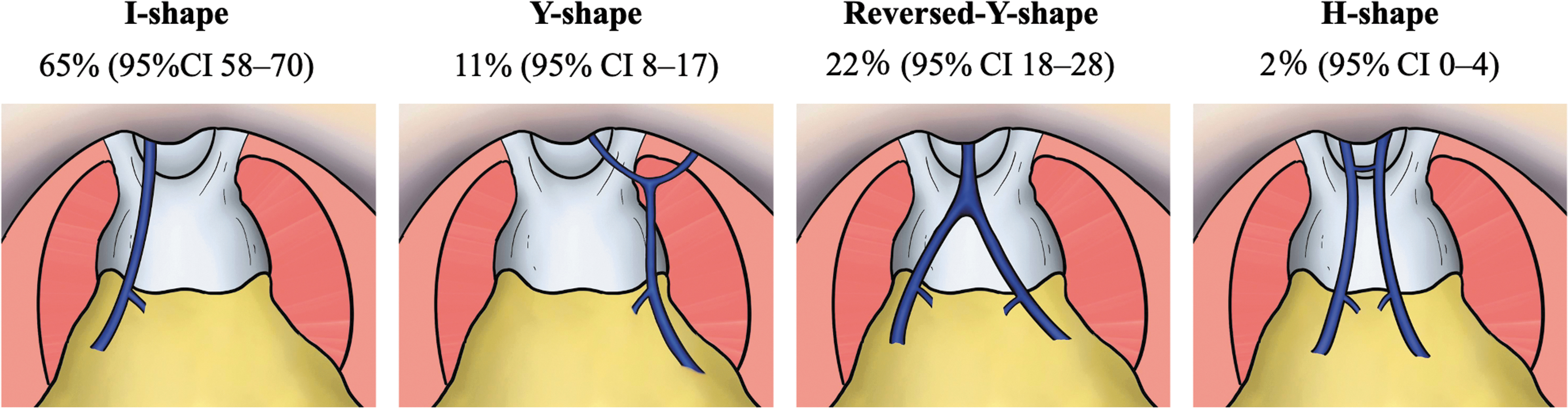
Four types of SPVs, I-, Y-, rY-, and H-shaped, with prevalence rates. CI = confidence interval. Color images are available online.

Four types of SPVs, I-, Y-, rY-, and H-shaped;
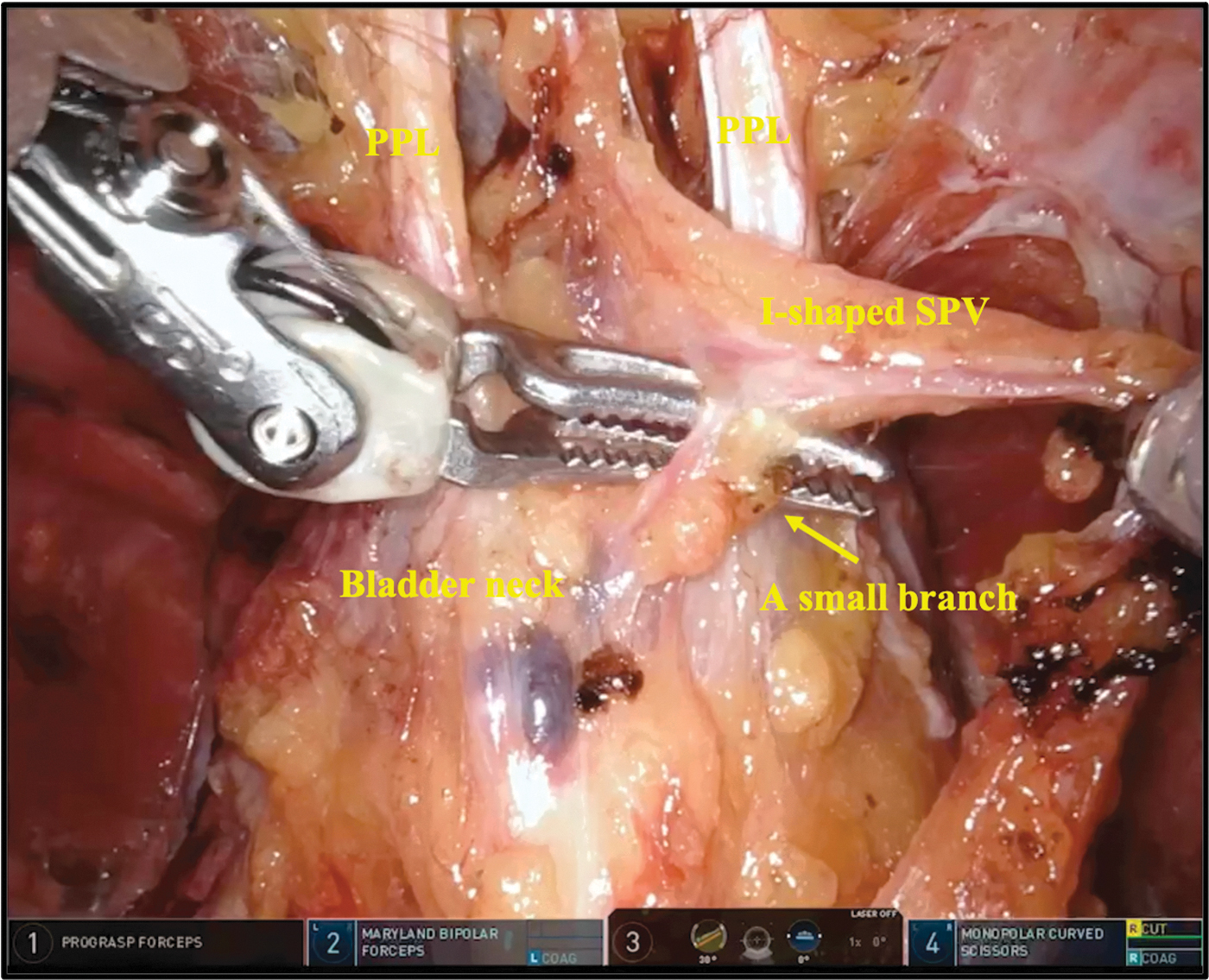
Small branch to the anterior bladder neck from an I-shaped SPV. Color images are available online.
The third most common type was Y-shaped SPVs, with a prevalence of 12% (95% CI, 8–17). The Y-shaped SPV is an I-shaped SPV with early bifurcation. A branch occurs proximal to PPLs to the right or left pelvic side walls. The bifurcation of Y-shaped SPV is more proximal to DVC (early bifurcation) compared with Y-shaped SPV (late bifurcation). One Y-shaped SPV gave off two branches, with one at the anterior prostate in addition to the one at the bladder neck. The H-shaped SPV was the rarest type, found in 4 of 252 men (2%; 95% CI, 0–4). This has the appearance of a pair of I-shaped SPVs running parallel, with a small branch connection proximal to the PPLs. One man had an H-shaped SPV without the connection, appearing as a double I-shaped SPV. This was included in the H-shaped SPV category.
Four men had the “other” variation and were excluded from SPV typing. One of these men had a superficial vein between PPLs that ran along the right pubic ramus to the right pelvic side wall without any SPV branching and was “U-shaped.” In another man, the right and left veins coursing along the pubic ramus joined above the prostatic apex without branching. The other two men in the “other” category had a superficial vein coming from the prostatic apex distal to PPLs, which ran along the right or left pubis ramus and then under the pubis ramus to the left pelvic side wall.
Pulsation of SPV was intraoperatively visualized in 39% (95% CI, 33–45) of men, possibly due to the presence of an accompanying tiny artery (Fig. 5). Although pulsations seemed to be initially absent in most SPVs, they seem to emerge and become more apparent late during surgery, possibly due to the increased arterial and venous blood flow after prostate removal.

Pulsating I-shaped SPV with two lateral APAs after anterior reconstruction. Color images are available online.
The inability to supply arterial flow to the corpus spongiosum via the prostatic artery and return venous flow to the prostate may have increased the arterial supply and venous return through SPV. The pulsation became particularly apparent after posterior reconstruction with Rocco's sutures, which stretched and slightly shrank the SPV. Two of the I-shaped SPVs contained a tiny artery (Supplementary Fig. S1), while one I-shaped SPV had a prostatic APA (Supplementary Fig. S3). These three pulsated at the time of identification.
Accessory pudendal arteries
Anatomical variations of APAs and the association between SPVs and APAs are summarized in Tables 1 and 3. All APAs were preserved except for one right small lateral APA. A total of 214 APAs were found in 142 of 252 men with SPV preservation (56%; 95% CI, 50–62), 165 lateral APAs in 111 men (44%; 95% CI, 38–50), and 50 apical APAs in 41 men (16%; 95% CI, 12–21). Thus, more lateral APAs were identified (44% vs 16%; p < 0.01).
Types of Accessory Pudendal Artery
The prevalence of APAs in cases where SPV was I-, Y-, rY-, and H-shaped was 54% (95% CI, 46–61), 67% (95% CI, 49–81), 57% (95% CI, 44–69), and 75% (95% CI, 29–96), respectively. We found significant pulsation in SPVs when one or more APAs were present (32% vs 45%; p < 0.04).
SPV preservation
With the assistance of a bed surgeon, SPV preservation is not difficult (Fig. 6). It is easiest in cases with a smaller prostate gland. In cases with large prostate glands, we ligated SPV early on as mobilization of a large prostate makes SPV preservation extremely difficult.

Preservation of an rY-shaped SPV with the assistance of a bedside surgeon;
After developing the Retzius space, SPV, when present, is visible through the adipose tissue at the prostatic apex. However, in patients with obesity, SPV often cannot be seen due to the amount of fat present. In such instances, we needed to remove the excess fat before we could secure SPV. After SPV identification, we released SPV from the surrounding adipose tissue by cutting sharply along both outer edges of SPV using the tip of monopolar curved scissors as thin layers of fascia cover the surface of the adipose tissue and SPV. Blunt retraction of SPV with laparoscopic suction or other laparoscopic instruments facilitates neat dissection. In cases with rY- or Y-shaped SPVs, the same procedure was performed with the bifurcating branch as the main trunk.
Before dissection of the bladder neck, a tiny branch to the anterior bladder neck should be ligated with a vascular clip or via coagulation using bipolar forceps (da Vinci Surgical System; Intuitive Surgical, Inc.) (Fig. 4). SPV is then sufficiently mobilized to be pushed to one side, according to its running course, by the bedside surgeon's manipulation. The bedside surgeon controls SPV location at all times, keeping it out of the operating field with laparoscopic instruments. For rY-shaped SPVs, either the two branches are brought to one side together or each branch is brought separately to the closest pelvic side wall.
Since rY-shaped SPVs are the most difficult to preserve, either branch may be cut off and preserved to leave an I-shaped SPV. Y-shaped SPV can easily be preserved in a “U” shape by ligating the main trunk. This “U-” shaped vein can be kept below the pubic bone not to obstruct the operating field.
Complete bladder neck dissection increases the mobility of prostate, bladder, and SPV; SPV can be pushed more laterally to the pelvic side wall. However, SPV is easily broken off when the prostate gland is mobilized too extensively. During mobilization of the prostate with a fourth arm (ProGrasp forceps) for dissection of Denonvilliers' fascia or NVBs, the console and bedside surgeon should pay attention to SPV location. If the SPV course and NVB-sparing side coincide, SPVs can be more easily preserved by grouping them with NVB.
During DVC suturing, 15 anterior reconstruction, or vesicourethral anastomosis, bleeding must be sufficiently controlled for clear SPV visualization to avoid entrapping SPV with the stitch (Supplementary Fig. S2). Having the bedside surgeon push SPV laterally out of the operative field helps prevent this. We recommend that the console and bedside surgeons secure SPV together, so that the console surgeon can complete the prostatectomy unimpeded.
Discussion
In 1991, Myers reported the anatomy of SPV in 160 men who underwent RRP. 2 We investigated this in detail in the robotic surgery era. Our I-shaped SPVs correspond to Myers single midline superficial vein without bifurcation, rY-shaped to SPV with bifurcation, and double I-and Y-shaped to other variations of the anomalous superficial vein. In addition, Myers proportions of each SPV type are consistent with our findings.
Our APA prevalence rate was higher than that reported in a 2017 meta-analysis, 9 possibly due to different APA identification methods. The meta-analysis included 23 studies, of which 4 found APAs during laparoscopic radical prostatectomy or RARP. 7,10,16,17 The other studies were cadaveric, radiographic, or RRP series, and likely missed small APAs visible only with an intraoperative microscope. 18 –21 Using a robot-assisted system, more APAs can be identified because of using highly magnified three-dimensional imaging and a drier surgical field with pneumoperitoneum. 22 Unlike the studies included in the meta-analysis, 9 we were able to identify a higher distribution rate of lateral than apical APAs (44% vs 16%; p < 0.01) due to our removal of all retropubic adipose tissue.
Although some apical APAs can be difficult to identify intraoperatively and the detection rate can vary depending on how the prostatic apex and DVC are dissected, 50 apical APAs were found in 41 of 252 men (16%; 95% CI, 12–21). Our apical APA prevalence was within the 8% to 22% reported by previous intraoperative studies with laparoscopy, 7,8,10 supporting our higher detection rate of lateral APAs.
Furthermore, we investigated the relationship between SPVs and APAs, hypothesizing that a tiny artery runs along pulsating SPVs as a median APA. Penile arterial supply of men with APAs is dominated by APAs rather than internal pudendal arteries (IPAs) 9 and tends to include the tiny median APA of SPV in addition to lateral APAs (32% vs 45%; p < 0.04). We posit that, compared with APA preservation only, preserving SPVs and APAs can better maintain blood circulation in the corpus spongiosum and contribute to shorter postprostatectomy potency recovery in NVB-sparing cases.
The descriptions of vasculature around the prostate in this study have clearly defined and classified SPV and APA depending on the anatomy, enabling future studies with standardized definitions for discussion. A classification standard is crucial as SPV anatomy often differs based on local geographic features such as APAs. 9
In conventional RARP, sufficient knowledge on the clinical anatomy of SPVs and APAs may preserve potency. At present, however, the role of APAs in potency remains controversial, 3,7,8,10,16 –19,23 and the function of SPVs with or without a median APA is unknown. The samples in this study were obtained from a single institution; therefore, generalizability of our results is limited. We could not compare the effect of SPV preservation on potency recovery as there were few cases where SPV was not preserved. Moreover, the surgical and clinical outcomes of RARP with preservation of the vasculature around the prostate, including the operative time, blood loss, complication rate, positive surgical margin rate, continence, and potency recovery, were not investigated. Thus, future research, assessing the role of APAs and SPVs and the impact of their preservation on surgical and clinical outcomes, is warranted.
Conclusion
The current study summarized the anatomical variations between SPVs and APAs. Notably, the SPV emerges from the space between the PPLs and runs within the retropubic adipose tissue anterior to the prostate toward the vesical venous plexus or pelvic side wall, whereas the APA courses through the periprostatic region running parallel to the DVC and extends caudally toward the anterior perineum. With a prevalence rate of 88% (95% CI, 84%–90%), SPVs were classified as I-, rY-, Y-, or H-shaped (64%, 22%, 12%, and 2%, respectively). In addition, we presented a technique for preserving each SPV type used during conventional RARP and recommend preserving arterial and venous vasculature around the prostate to preserve postprostatectomy potency.
Footnotes
Acknowledgment
The authors would like to thank Enago (
Authors' Contributions
Y. Ozawa: conceptualization (lead); data curation; formal analysis; investigation; methodology; project administration; resources, software; visualization; writing—original draft (lead); and writing—review and editing (lead). K.A.: data curation; investigation; visualization; and writing—review and editing (equal). S.K.: data curation; investigation; and writing—review and editing (equal). M.Y.: data curation and writing—review and editing (equal). Y. Odagaki: data curation; investigation; and writing—review and editing (equal). H.S.: data curation; investigation; and writing—review and editing (equal). K.Y.: conceptualization (supporting); investigation; writing—original draft (supporting); writing—review and editing (equal); and supervision.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.