
Abstract
Purpose:
This study aimed to assess early outcomes of the single port (SP) robotic low anterior access (LAA) for all upper urinary tract surgeries. In addition, it aimed to explore the impact of clinical factors, notably Body Mass Index (BMI), on post-operative outcomes and length of hospital stay.
Materials and Methods:
Overall, 76 consecutive patients underwent SP robotic surgery with LAA involving all upper urinary tract pathologies, with data collected prospectively. Baseline characteristics, intra- and post-operative outcomes, pain levels, and opioid use were analyzed. Statistical methods, including logistic regression and locally weighted scatterplot smoothing analysis, were used to assess same-day discharge (SDD) predictors and the association between BMI and SDD probability. According to the Institutional Review Board (IRB) protocol, only data recorded in our electronic medical record system was included.
Results:
Ten different procedures were performed with LAA, with no need for conversion to open surgery and complication rates in line with the literature (30 days: 5%, 90 days: 6.6%). Notably, 77.6% of patients were discharged on the same day. A significant association was found between BMI and prolonged hospital stay, particularly in obese patients (BMI ≥30 kg/m2). Post-operative pain was generally low (median VAS: 4), with over 70% discharged without opioid prescriptions.
Conclusions:
The novel LAA is a versatile approach for various upper urinary tract surgeries, including in obese patients. While achieving satisfactory post-operative outcomes, increased BMI correlated with a reduced likelihood of SDD. Further studies, including larger cohorts and multicenter collaborations, are warranted to explore anesthesiologic management and validate these findings.
Introduction
Historically, upper tract urological surgery has been performed through retroperitoneal open approaches. The introduction of robotic surgery with the multi-port (MP) platform has determined a change in favor of transperitoneal approach. This shift was dictated by the MP robot's need for working space. However, the trans-peritoneal approach is associated with non-negligible drawbacks. First, the need to create an induced pneumoperitoneum may lead to a delay in recovery of normal bowel function, resulting in a longer hospital stay. 1
Second, the steep Trendelenburg and the lateral decubitus patient positioning needed for respectively pelvic and upper urinary tract surgery may cause prolonged operative time and may expose patients to underrated anesthesiologic complications. 2,3 Finally, the trans-peritoneal approach can be highly challenging in obese patients, in patients with severe pulmonary conditions, and in patients with previous abdominal surgery. To overcome all these potential limitations, the single port (SP) system has brought back momentum to retroperitoneal access thanks to the possibility of accessing the anatomical target through a direct route.
In particular, SP requires smaller anatomical space to maneuver surgical instruments and, as such, it allows to perform surgical procedures from the lower to upper urinary tract using the same single incision access to the retroperitoneal space and maintaining the patient in supine position. 4 Moreover, recent studies have shown that patients treated with SP extraperitoneal approaches are more likely to be discharged on the same day of the surgery.
Still, it is unknown whether the feasibility and potential advantages of SP surgeries can be negatively influenced by high Body Mass Index (BMI) and can, therefore, be applied in obese patients as well. 5,6 Based on these premises, we aim to assess the feasibility and early outcomes of the Retroperitoneal low anterior access (LAA), previously named SARA (Supine Anterior Retroperitoneal Access) by Pellegrino et al. among different surgical procedures. 4 The secondary aim has been to assess whether clinical factors such as BMI and comorbidities may influence outcomes of these surgeries in terms of intra- and post-operative outcomes.
Patients and Methods
Study population
Overall, we identified 76 consecutive patients who underwent SP robotic surgery for upper urinary tract pathologies, including renal masses, primary upper tract urothelial tumors, uretero-pelvic obstruction syndrome, ureteral strictures, and ureteral calculi. All surgical procedures were performed by the same surgeon, who started performing SP surgery in December 2018. All the patients underwent surgery at the same hospital (UI Health, Chicago, IL).
Data were reported since the introduction of the LAA approach in October 2022. All patients were included in a prospective maintained database, including baseline characteristics, intra- and post-operative surgical outcomes. Patients lost to follow-up after the procedure were excluded from the study. One case has been temporarily excluded from the series due to pending litigation.
For our analysis, patients were stratified according to same-day discharge (SDD) vs inpatient stay (IS). Each IS was the result of a shared-decision process involving both surgical and anesthesiology teams. This decision was influenced by several factors, including the patient's pre-operative characteristics (such as BMI, Charlson Comorbidity Index (CCI), ASA, and case complexity) as well as intra-operative findings such as estimated blood loss, duration of the procedure, and intra-operative complications.
Surgical technique
All surgical procedures were performed under general anesthesia, with the patient supine (Fig. 1). A single 3 cm incision at approximately McBurney point was made. After separating and dissecting the various layers (anterior fascia, internal and external oblique, and transversalis muscles), retroperitoneal space was exposed and, with a finger, developed. No space maker balloon was needed. AirSeal assistant port (ConMed Corp., Utica, NY) was placed in a “Sidecar” fashion, using the same skin incision as the SP trocar but in a different fascia incision.

Operative room set-up and patient positioning during LAA approach. LAA = lower anterior approach.
For all surgical procedures involving kidney and proximal tract of ureter, an SP robotic camera was inserted at 6-o'clock position, while for procedures involving distal tract of ureter and pelvis, an SP robotic camera was typically inserted at 12-o'clock position. When a peritoneal defect was noted, Veress needle was typically placed at the contralateral side of the incision, along the anterior axillary line and below the costal margin, to vent the peritoneal cavity. Peritoneal defect was subsequently sutured using a 3/O Vycril. The LAA (previously named SARA) was described by Pellegrino et al. in a recent work. 4
Study variables
We considered clinical and demographic characteristics, including age, BMI, gender, (CCI), American Society of Anesthesiologists (ASA) score, previous abdominal surgery, and type of surgical procedure. Intra- and post-operative surgical outcomes included 30-day and 90-day complications according to the Clavien-Dindo classification, 7 intra-operative blood transfusion, readmission rate, estimated blood loss, conversion to transperitoneal approach, conversion to open surgery, peritoneal defect opening, ΔHCT (assessed as changes in hematocrit between baseline and discharge), post-operative pain, post-operative opioid use, and opioid prescription at discharge.
We measured post-operative pain using a visual analogue scale (VAS) to measure post-operative pain, considering the last recorded value on 0 PO Day. We recorded post-operative opioid use as any administration of narcotics during the hospital stay in the post-operative period.
Statistical analysis
Categorical variables are summarized showing frequency and percentages, while continuous variables are presented with mean, median, and interquartile range (IQR). Statistical analysis of baseline characteristics and intra-/post-operative outcomes was conducted, using χ 2 test and test t Student. Subsequently, we compared baseline characteristics according to SDD vs IS using χ 2 test and test t Student.
A multivariable logistic regression model was used to test predictors of SDD, and covariates consisted of BMI, CCI, and type of surgery. Lastly, locally weighted scatterplot smoothing (LOWESS) analysis was used to visually explore the probability of SDD according to BMI. All statistical analyses were performed with R software (version 4.3.2).
Results
Overall, 76 surgical procedures with the novel LAA approach were performed, with 32 (42%) males and 44 (58%) females. As described in Figure 2, 39 patients underwent Single-Port Partial Nephrectomy (SP-RAPN), 16 patients SP Radical Nephrectomy (SP-RARN), and 2 patients SP Nephroureterectomy (SP-RNU) with bladder cuff excision. All baseline characteristics are presented in Table 1.

Surgical procedures performed with LAA approach.
Baseline Characteristics for Overall Population (n = 76)
Median (IQR).
Mean.
ASA = American Society of Anesthesiologist; CCI = Charlson Comorbidity Index.
Notably, the mean BMI was 31.7 kg/m2, with 50% of patients considered obese (BMI ≥30). Intra- and post-operative outcomes are described in Table 2. Moreover, 24 patients (32%) underwent previous abdominal surgery, including colectomy, prior partial nephrectomy. There was no need to convert to open surgery and no need to switch to a standard surgical approach. Peritoneal defect was noted in 10 (13.2%) patients.
Intra-Operative and Post-Operative Outcomes for Overall Population
median (IQR)
ΔHCT = changes in Hematocrit between baseline and discharge; VAS = Visual Analogue Scale.
All peritoneal defects were repaired as previously specified, and no case required conversion to the transperitoneal approach. Of the 76 patients, 59 were discharged the same day (77.6%, Table 3). The 30-day post-operative complications rate was 5%, with no Clavien-Dindo ≥3 complications recorded, while the 90-day post-operative complications rate was 6.6%. Supplementary Table S1 summarizes post-operative complications. The 30-day and 90-day readmission rates were 6.6% and 7.9%, respectively.
Clinical and Post-Operative Characteristics Among Patients Discharged the Same Day vs Not Same-Day Discharged
Median (IQR).
Mean.
Post-operative pain was moderate-low (median VAS 4, IQR 3–5) and post-operative opioid use rate, assessed as any administration of narcotics after surgery, was 40%. In comparison, 60% of patients did not need any opioid as an analgesic. No differences were found in terms of post-operative pain (mean 3.6 (0.26) vs 4.1 (0.68) p 0.5, for SDD vs IS, respectively) and opioid use between SDD group vs IS (n = 22 vs 8, p 0.6, for SDD vs IS, respectively).
Overall, at discharge, 72.4% of patients did not need a narcotic prescription. When stratifying according to SDD group vs IS, we noted a significant statistical difference with BMI (mean 31.7 (SD 0.98), 30.4 (0.97) vs 36.2 (2.58) p 0.04, for overall, SDD vs IS, respectively). When exploring the correlation between BMI and probability of SDD after adjusting for covariates in multivariable logistic regression models, increased BMI was statistically associated with a lower likelihood of SDD (OR, 0.92, 95% CI: 0.86–0.98, p = 0.01) (Table 4).
Multivariable Logistic Regression Model Predicting Same-Day Discharge
BMI = body mass index; OR = odds ratio.
After that, at LOWESS analysis, which graphically represented the correlation between BMI and SDD, we observed a steady decrease in SDD with increasing BMI up to 30 kg/m2, after which a plateau was observed (Fig. 3).
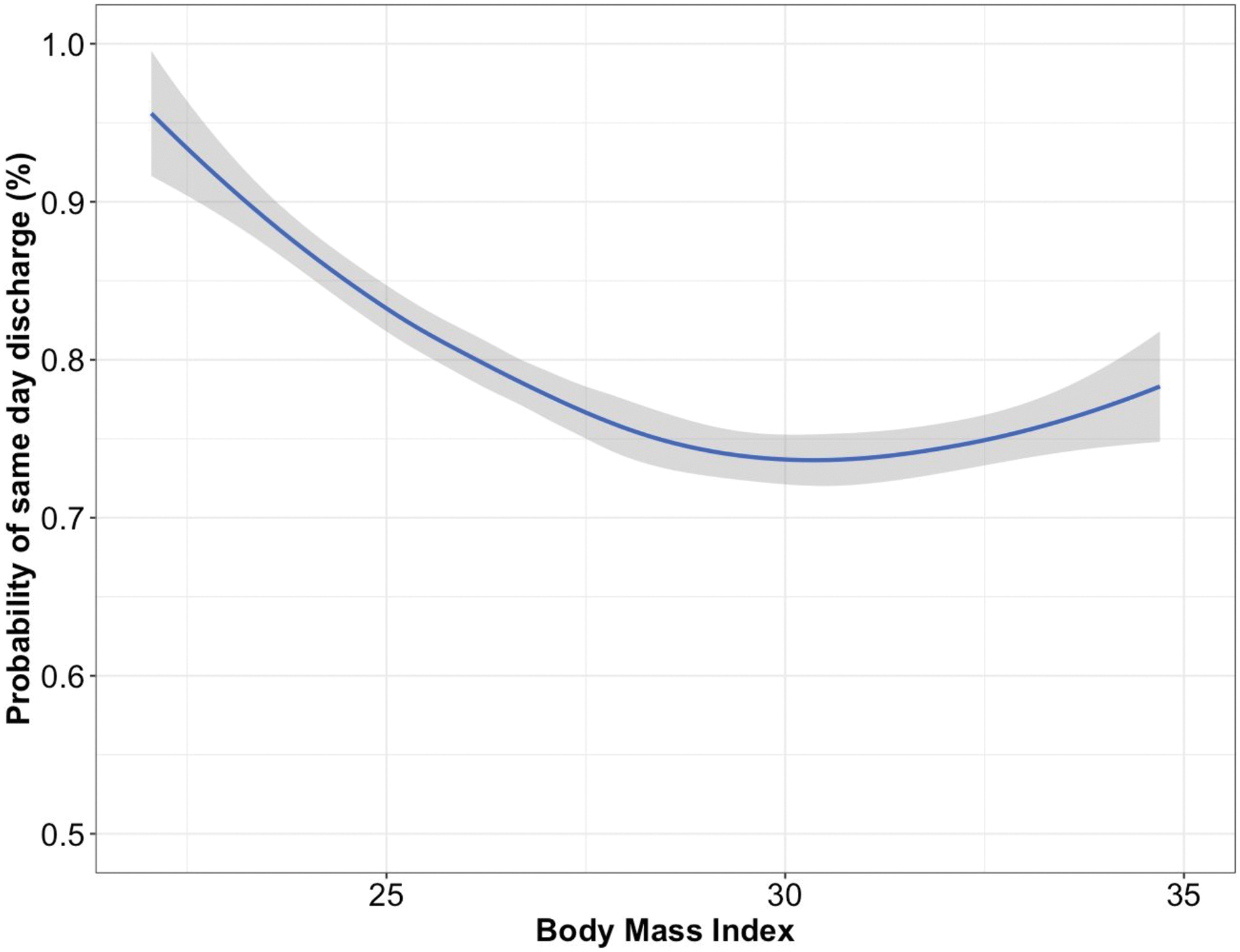
LOWESS analysis reporting probability of SDD according to BMI. BMI = body mass index; SDD = same-day discharge.
Discussion
To the best of our knowledge, this is the first study showing early outcomes of this approach among different surgical procedures and exploring the role of clinical factors and of BMI on the risk of prolonged hospital stay for patients treated with SP system. One of the main features of the SP system is its versatility. Surgical instruments do not require ample working space but can be manipulated with ease and accuracy even in a narrow space. 8
Using this flexibility, the SP system has facilitated access to the retroperitoneum, overcoming the issues encountered with MP, such as handling the instruments in a confined environment that can more easily cause external clashing of the instruments. The innovative feature of this novel surgical access is the possibility to perform different surgical procedures of the upper urinary tract with the same incision at the McBurney point, maintaining supine position and avoiding all anesthesiologic and post-operative complications related with lateral decubitus and or steep Trendelenburg.
Noting the uniqueness of our patient cohort, with half of them having a BMI ≥30, we explored the feasibility of this access in obese patients analyzing whether BMI may negatively influence post-operative surgical outcomes and risk of prolonged stay across different surgical procedures of the upper urinary tract. This said, several of our findings are worth highlighting.
First, our results demonstrated that LAA is highly versatile. Of the 76 surgeries, 80% were for oncological indications, involving 10 different procedures (Fig. 1). Versatility of this approach can be particularly appreciated performing nephroureterectomy with bladder cuff excision: in these cases, with a single incision, it is possible to reach both the upper and lower urinary tract, strengthening the concept of “multi-quadrant surgery.”
Overall, there was no need for conversion to open surgery and there was no need to switch to a standard approach. We demonstrated that LAA intra-operative and post-operative complication rates align with the literature, 9 even considering studies including partial nephrectomy only. 10 Moreover, our data showed that discharging the patient on the same day is feasible, thus confirming that LAA is a one-stop solution for any feasible procedure involving the upper urinary tract.
Second, a significant statistical difference between SDD and IS was recorded regarding BMI. Of note, half of our patient cohort was considered obese using the definition of BMI ≥30 kg/m2. When exploring the correlation between the probability of SDD and BMI, we observed a decrease in SDD until reaching a plateau at BMI ≥30, thus confirming the reliability of the definition of obesity in this clinical scenario.
This could be explained because of anesthesiologic-related reasons. It is not unusual for anesthesiologists to prefer to monitor more frail patients for 24 h post-operatively. On the other hand, no differences were found in terms of post-operative complications. Taken together, although we confirmed the feasibility of LAA even in highly obese patients, this aspect should be considered before surgical planning to inform overweight patients of the possibility of prolonged post-operative stay properly.
Finally, significant results were also noted regarding post-operative pain levels and the need for opioid administration, which deserve emphasis. Specifically, overall post-operative pain was low, with a median VAS score of 4 (IQR 2–5), with a high rate of early discharges (77.6%), confirming what we know from the literature about the SP system and confirming that avoiding peritoneum access is associated to a lower post-operative pain. 11 –13
Notably, 60% of patients did not require any opioid administration and more than 70% were discharged without any opioid prescription. This could be partially attributed not only to the absence of anesthesiologic issues related to patient positioning but also to the avoidance of irritation of the peritoneum, mandatory for the transperitoneal approach, sensitive to increased intra-abdominal pressure due to the pneumoperitoneum, causing oxidative stress. 14
This study aimed to explore the feasibility of this novel LAA among different surgical procedures, showing satisfactory early post-operative outcomes and demonstrating that it is safe even in morbidly obese patients, although a longer length of stay may be needed. The strength of our work lies in the including of all patients treated with LAA consecutively at a tertiary referral center for minimally invasive surgery, and all data have been standardized.
Conversely, this study is not devoid of limitations: First, its retrospective nature unavoidably introduces selection biases. Second, given our intent to explore the flexibility of SP among different upper urinary tract procedures, we did not perform a stratification according to the type of surgery for our analyses. Thus, residual heterogeneity needs to be considered when interpreting the results.
Moreover, the small number of patients included, the lack of a comparison group and the lack of long-term follow-up are two other aspects to note. This said, further studies are needed to better investigate anesthesiologic management, especially for morbidly obese patients, and to increase the patients' cohort also through a multicenter collaboration.
Conclusions
Using the SP system, LAA is a purely retroperitoneal, extremely versatile approach. When technically feasible, surgical procedures involving all upper urinary tract can be performed with promising surgical outcomes, even in obese patients, demonstrating a rate of post-operative complications in line with the literature. BMI must be considered for outpatient vs inpatient surgery: We have shown that the probability of SDD decreases as BMI increases, reaching a plateau at BMI ≥30 kg/m2. In addition, post-operative pain was substantially low, with more than half of the patients not requiring opioid analgesics after surgery.
Authors' Contribution
D.C., G.P., and S.C.: Protocol/project development; R.C.S., G.P., J.A.T., and L.M.: Data collection or management; D.C., E.M.: Data analysis; D.C., S.C.: Manuscript writing/editing; E.M., L.M., A.A.P., G.P., A.A., F.M., and A.B.: Critical revision of the manuscript.
Footnotes
Disclosure Statement
Dr. Crivellaro is a consultant for Intuitive Surgical. The remaining authors have nothing to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.