
Abstract
Purpose:
Patients who present with urinary tract infections secondary to obstructing stones occasionally fail to improve on treatment based on midstream urine culture (MUSCx). Varying microbiomes between the bladder and the renal pelvis may account for this. In this study, we sought to investigate the utility of obtaining a renal pelvis urine culture (RPUCx) at the time of stenting to guide antibiotic treatment prior to definitive stone operation.
Materials and Methods:
RPUCx was obtained in 257 patients presenting with obstructive ureteral stones undergoing emergent stenting. Concordance rates of RPUCx to MUSCx and blood cultures were examined. Operative time and infectious complication rates after definitive stone management between the two groups were studied. A comparison of those who received an intraoperative RPUCx with those who did not was carried out.
Results and Conclusions:
RPUCx was obtained in patients undergoing emergent stenting from 2018 to –2021; 31% (52/168) of patients had pathogens in the renal pelvis that were absent in the MUSCx. RPUCx had a greater concordance rate with blood culture results compared with MUSCx (95% vs 50%). Drawing RPUCx intraoperatively did not significantly change operative time (15.9 vs 13.6 minutes, p = 0.15). Treatment tailored to RPUCx resulted in lower rates of post-stone management complications (odds ratio 0.26, 95% confidence interval = 0.08–0.83; p = 0.01). RPUCx at the time of stenting can guide treatment and decrease post-treatment complications without additional operative time, confirming utility in the treatment of patients with infection secondary to obstructing stones.
Background
Ureterolithiasis is a common urologic condition, and its incidence has increased over time. 1,2 Obstructing ureteral stones may cause a myriad of symptoms including flank or back pain, hematuria, nausea, or emesis. Obstructing ureteral stones do not always mandate urgent upper tract decompression. However, bilateral ureteral stones, stones in a solitary kidney, and those associated with infectious concerns and refractory pain need urinary drainage. Upper tract drainage is particularly critical when obstructing stones are associated with urinary tract infection (UTI) or sepsis. 3
Urgent retrograde stenting and antibiotic therapy are performed for obstructing stones with UTI or sepsis. The choice of antibiotics is made empirically until midstream urine culture (MUSCx) results are available and antimicrobial therapy is tailored accordingly. Occasionally, these patients fail to improve on apparent appropriate therapy. This may be attributable to discordant pathogens in the bladder and the renal pelvis proximal to the point of obstruction. In 1995, Gault et al. demonstrated a 38% concordance between the bacteria in the stone and MUSCx. 4 This was further corroborated by the work of Mariappan et al. who demonstrated that MUSCx had a sensitivity of 30.2% and a negative predictive value of 62% for predicting renal pelvis urine culture (RPUCx). 5 Other groups have also demonstrated this discordance, but most of these studies compared MUS and stone cultures. 6 However, ureteroscopy or percutaneous nephrolithotomy (PCNL) to retrieve stone fragments is generally contraindicated in patients with obstructing ureterolithiasis with a UTI or sepsis. A urine specimen from the renal pelvis is readily accessible during stenting. In this study we sought to evaluate the value of obtaining RPU specimens at the time of stenting in all patients with obstructive ureterolithiasis, particularly in those stented for infectious reasons, to detect pathogens not found on MUSCx.
Materials and Methods
An institutional review board (IRB00079434) application was approved for this study. Using STROBE criteria, we performed a retrospective chart review of collected data of all patients who underwent retrograde ureteral stenting for obstructive ureterolithiasis for acute kidney injury (AKI), intractable pain, or UTI/sepsis from January 2018 to December 2021 at our medical center. Data collected included demographics, results of MUSCx, RPUCx, and blood cultures, urinalysis, stone size, location, and presence of hydronephrosis among other data points. Blood cultures were drawn if the patient met sepsis criteria. 7 All specimens were sent for culture and Gram stain. The location of the largest stone was recorded in patients with multiple ureteral stones. All implanted stents silicone, Double-J stents. Blood agar was used as a culture medium. Preliminary culture results were typically available within 24 hours, and final results with sensitivities were available by 48 hours. Postoperatively, oral antibiotics were continued in the outpatient setting until definitive stone management. RPUCx was not obtained in cases of extreme hemodynamic instability or in cases where hydronephrosis was minimal and no urine could be aspirated from renal pelvis. The complication rate was examined, which was defined as unplanned emergency department or clinic visits and readmissions (including postoperative UTIs and sepsis) within 30 days. Fisher’s exact test and Pearson’s chi-square analysis at the 0.05 significance threshold were used with the Holm–Bonferroni method to reduce false-positive rates. Statistical analysis was performed using R statistical software.
All stents were performed cystoscopically under fluoroscopic guidance. The procedure was carried out using a 22 French rigid cystoscope through which a 6 French ureteral catheter was placed into the ureteral orifice. A flexible wire was then placed through the catheter and advanced to the level of the renal pelvis, which was confirmed using fluoroscopy. The ureteral catheter was then advanced into the renal pelvis and the wire was removed. A syringe was used to aspirate urine from the renal pelvis, and then a low-pressure retrograde pyelogram was performed using minimal contrast. The wire was replaced, and the ureteral catheter was offloaded. Over the wire, an untethered Double-J stent was placed. Proper stent placement was confirmed via both fluoroscopy and endoscopic vision.
Results
From January 2018 to December 2021, a total of 383 patients were urgently stented for ureterolithiasis at our institution. RPUCx was obtained in 67% (257/383) of the patients. For the entire cohort, the median patient age was 56 (41–69) years, the median stone size was 7 (5–9) mm, with a median operative duration of 16 (12–22) minutes and length of stay of 23 (0–72) hours. A summary of the stone location can be found in Table 1. The predominant indication for ureteral stenting was for suspected UTI (55%; 213/383), followed by AKI (25%; 97/383) and intractable pain (20%; 77/383).
Demographic Data for All Patients Undergone Urgent Stenting
Reason for stenting.
Patients stented for infection had fever, leukocytosis >14k, a nitrite or bacteria-positive urinalysis, or sepsis with no other etiology.
Acute kidney injury (AKI) was defined as a creatinine rise of ≥50% from baseline.
Patients were stented for pain or nausea/emesis which was refractory to maximal medical therapy, including PO and IV forms of NSAIDs, narcotics, and two antiemetics.
Ten patients had no data recorded. These patients came with CT scan reads from another facility without definitive measurements and no imaging available to view.
BCx = blood culture; ED = emergency department; IQR = interquartile range; IV = intravenous; PO = per os; NSAIDs = nonsteroidal anti-inflammatory drugs.
Of the 383 patients, 55% (213/383) were urgently stented for suspected UTI or sepsis attributed to obstructing stones. All these patients received a MUSCx preoperatively. An intraoperative RPUCx was obtained in 79% (168/213) of these patients. This subset of patients was our group of interest. In this group of interest, RPUCx was positive in 52.4% (88/168), with the most frequent pathogens being Escherichia coli, Proteus mirabilis, and Candida albicans (Table 2). MUSCx was positive in 42.9% (72/168) of patients in this group with the most frequent pathogens being E. coli, P. mirabilis, and Klebsiella pneumonia. Blood cultures were positive in 31% (52/168) of patients in this group, with the most common pathogens being E. coli, K. pneumonia, and P. mirabilis. Median operative time did not differ significantly between cases in which RPUCx was obtained and cases in which it was omitted, measuring 15.9 vs 13.6 minutes (p = 0.15), respectively. In the group of interest, 25% (42/168) of patients had a positive RPUCx with a negative MUSCx, whereas 12.5% (21/168) of patients had a positive MUSCx and negative RPUCx (Fig. 1). In 19% (32/168) of this subset of patients, both RPUCx and MUSCx were positive. Within this subset, 31.3% (10/32) had discordant pathogens. Ultimately, 31% (52/168) of patients within the group of interest had pathogens in the RPUCx, which were not found in MUSCx.
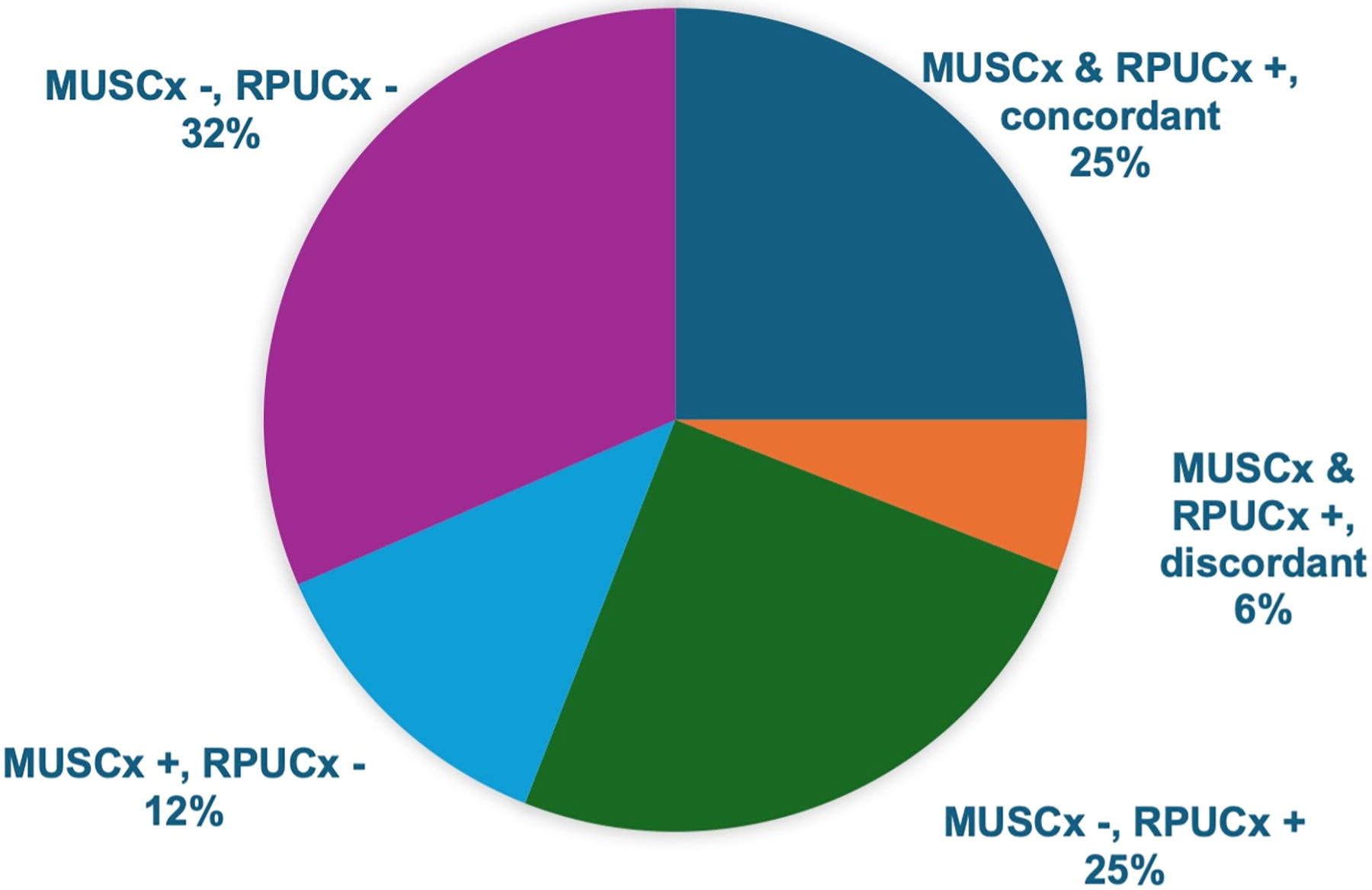
Concordance of positive RPUCx and MUSCx in the study population. MUSCx = midstream urine culture; RPUCx = renal pelvis urine culture.
Most Common Isolated Pathogens and Stratified by Source
MUSCx = midstream urine culture; RPUCx = renal pelvis urine culture.
Thirty-four patients not only had data regarding MUSCx and RPUCx but also had blood culture data. In this group, 58.8% (20/34) of patients had a positive RPUCx, and 50% (17/34) had a positive MUSCx (Fig. 2). The RPUCx–blood culture pathogen concordance rates were significantly higher when compared with the MUSCx (95% vs 50%, p < 0.01). Analyzing records from patients who received a stent for AKI or pain and had appropriate cultures drawn, MUSCx was positive in 22/144 (15.2%) patients and RPUCx was positive in 26/90 (28.8%) of the patients. Antibiotic susceptibility results were available for 94 patients. The empirically prescribed perioperative antibiotics were inappropriate relative to the RPUCx results in 30% (28/94) of the patients. The most administered preoperative antibiotics were ceftriaxone, cefazolin, and piperacillin/tazobactam. In instances where perioperative empiric antibiotic treatment was insufficient, the most common culprits were cefazolin (76%) and ceftriaxone (23%). Complication rates after stent placement did not differ significantly between those who had appropriate perioperative antibiotics to RPUCx and those who did not, but the total complication rates after definitive stone management were lower in patients who received appropriate RPUCx-guided antibiotics (20% vs 50%, p = 0.03) (Table 3). Sepsis rates after definitive stone management were lower in the group receiving RPUCx target antibiotics than those with empiric antibiotic therapy (5.8% vs 35%, p = 0.03).
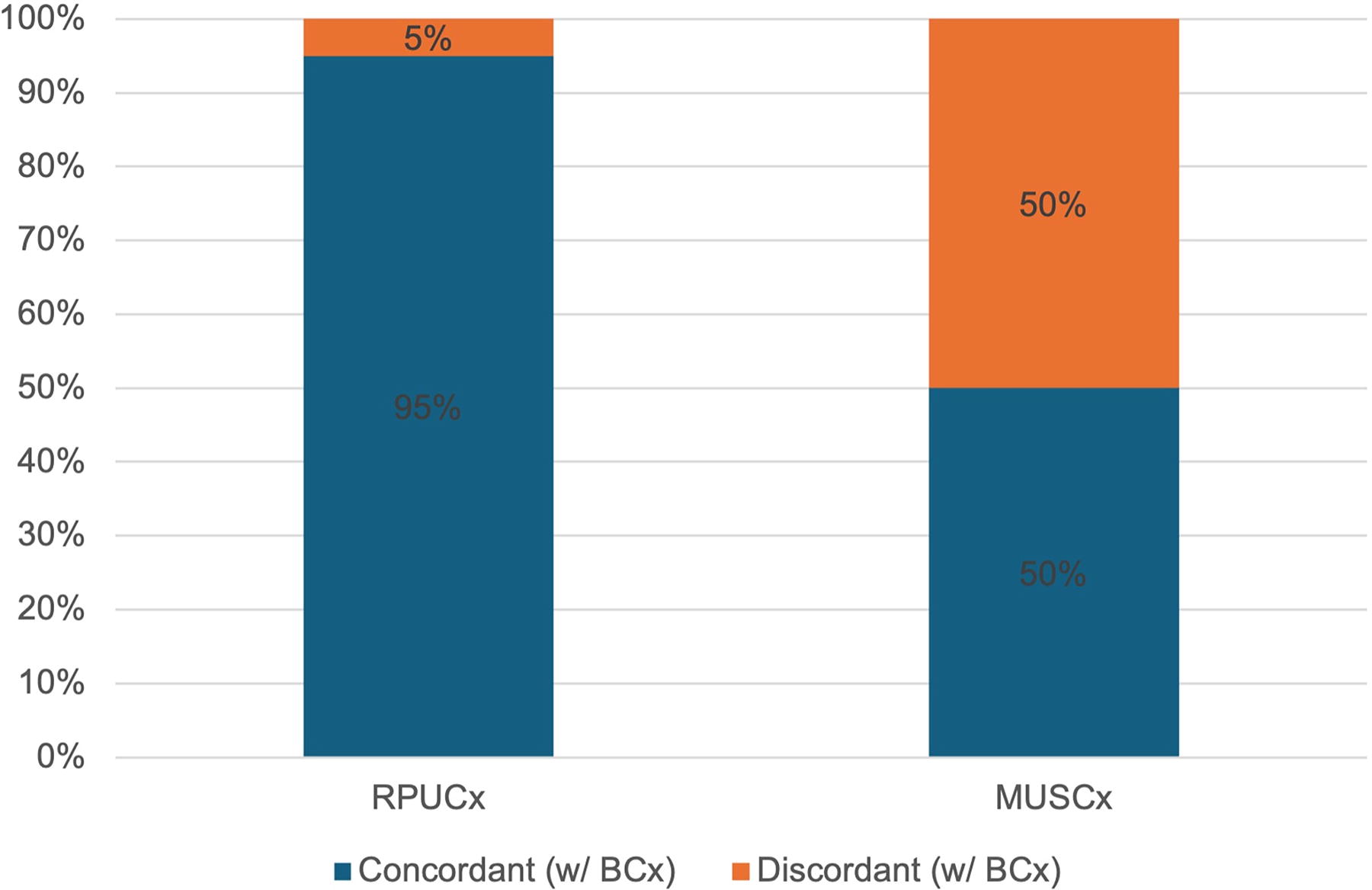
Concordance of RPUCx and MUSCx in patients with positive blood culture (BCx). Column “RPUCx” demonstrates a 95% concordance of blood and renal pelvis urine cultures. Column “MUSCx” demonstrates a 50% concordance of blood and midstream urine cultures.
Complications and Unplanned Emergency Department (ED) or Clinic Visits After Definitive Stone Management
Note: Bold values indicate statistically significant values determined by p < 0.05.
AKI = acute kidney injury; UTI = urinary tract infection.
Discussion
Obstructive ureterolithiasis is considered a urologic emergency particularly when associated with UTI, AKI, solitary kidney, or if presenting bilaterally. Retrograde stenting is typically the treatment of choice for those with infectious concerns. The postoperative course in patients stented for infected stones revolves around antibiotic therapy tailored toward MUS culture. However, in those with high-grade obstruction, the urinary biome may differ between the bladder and the urine proximal to the stone. MUSCx may be misleading in these patients, and negative culture results may not correlate to the patient’s clinical picture. Prior studies have demonstrated a discordance between MUSCx and stone cultures during PCNL. This is of paramount importance as the risk of post-PCNL systemic inflammatory response (SIRS) increases 10-fold in patients with positive stone culture. 8 As most patients exhibit a SIRS response in the first 24–48 hours after operation, intraoperative urine and stone cultures may not provide timely information to prevent urosepsis. As a result, intraoperative urine Gram stain during PCNL was studied to detect the presence of infection given its expedient nature. However, the results of its ability to predict postoperative SIRS have been conflicting. 9,10 Based on the findings that a positive MUSCx was significantly associated with urosepsis after ureteroscopy despite adequate preoperative antibiotic course, it can be postulated that stagnant urine behind a stone may harbor pathogens not detected in MUSCx. 11,12 In this context, collecting RPUCx may have utility in decreasing morbidity in those stented for obstructing, infected stones.
Initially described by Mariappan and colleagues, MUSCx is a poor predictor of upper tract infection in patients with obstructing stones. 5 This led to a few studies investigating the role of RPUCx during PCNL to predict postoperative SIRS and urosepsis. However, obtaining RPUCx at the time of PCNL may be too delayed to prevent sepsis in this patient population. In our study, 52.4% of patients had a positive RPUCx, whereas 42.9% of patients had a positive MUSCx. Pathogen discordance was observed in 31.3% of patients. Thus, RPUCx was able to provide unique pathogen information for 31% of all patients in the study group. A similar pathogen discordance rate of 29.4% has been reported during PCNL for these two parameters. 13,14 Though discordance in our study was only in 10 patients, it underscores the importance of obtaining both MUSCx and RPUCx for adequate treatment of UTIs in the setting of planned surgical stone management. It also underscores the differential microbiome in the bladder and upper tracts, particularly in the setting of ureteral obstruction. We have demonstrated a higher concordance of RPUCx with blood cultures compared with MUSCx, 95% vs 50%, which is critical in guiding antibiotic therapy in patients with bacteremia. 13 Furthermore, Yoshida et al. described that a positive intraoperative RPUCx at the time of ureteroscopy was associated with postoperative SIRS response despite an adequate antibiotic regimen. 15 We have demonstrated that obtaining an RPUCx at the time of urgent stenting and providing an appropriate antibiotic regimen significantly reduces the risk of complication after definitive stone management. We have also demonstrated that RPUCx is positive in close to one-third of patients undergoing stenting for AKI or intractable pain and thus is a valuable piece of information regardless of the reason for urgent stenting.
Anesthesia-related complications in patients with sepsis must be considered, and for these patients, rapid stenting is indicated to decrease anesthesia-related complications. Obtaining a renal pelvis urine specimen would certainly be expected to prolong time under anesthesia as it adds an extra procedural step. In this study, operative time was 2.19 minutes longer for patients in whom RPUCx was obtained. It is important to note, that this difference is not statistically and likely not clinically significant and therefore should not impact the decision to obtain RPUCxs.
Based on this study, RPUCx at the time of stenting for infected stones provides critical information to guide antibiotic therapy and to decrease complications after definitive stone management. However, this study is not without limitations. First, the retrospective nature of data collection prevented standardized specimen collection and analysis including timing and type of antibiotic administration. Second, this study did not include those patients undergoing PCNL tube placement for pelvicalyceal decompression and focused on retrograde stenting alone. The inclusion of these patients may further clarify the disparities in the culture results. Third, many patients were transferred to our institution from other centers and already had received one or more doses of antibiotics before transfer. Given that urine cultures may be rapidly sterilized, the results presented herein may represent an underestimation of patients with significant growth from RPUCx, MUSCx, or both. Finally, formal fungal cultures were not routinely obtained. However, several patients did demonstrate funguria, particularly from the RPUCx, in regular urine culture media. Regardless, the data presented herein have demonstrated that antibiotic therapy tailored to RPUCx decreases morbidity, complications, and sepsis after definitive stone management.
Conclusions
RPUCx during the time of stenting provides critical information in the management of acutely ill patients with infected, obstructing stones and decreases complication rates after definitive stone management with no significant increase in operative duration or morbidity. Thus, RPUCx should be obtained in every patient undergoing urgent stenting for obstructing stones, regardless of the reason for stenting, as a standard of practice.
Footnotes
Authors’ Contributions
M.M.: Project conceptualization and supervision and article writing (review and editing). R.X.: Data curation, formal analysis of data, and article writing (review and editing). C.O’C.: Data curation. P.U.T.: Data curation, formal analysis of data, and article writing (review and editing).
Author Disclosure Statement
The authors have no conflicts to disclose.
Funding Information
No funding was received for this article.