
Abstract
Pheochromocytoma is a rare disease in children with incidence of reported as 1 in 10 million children. There are few reported series with clinical follow-up published in literature from the Indian subcontinent; none has reported minimally invasive operation for pheochromocytoma and long-term outcome. These children present with symptoms secondary to increased catecholamine secretion from the adrenal pheochromocytes, of which hypertension is the most common and can be life threatening. Although hypertension in children is almost always secondary to a hidden disease, children with pheochromocytoma may be treated for a while before diagnosis is established. Surgical excision of the tumor is the treatment. Preoperative assessment can be challenging as 10% of the cases may be syndromic with bilateral tumors and associated with multiple endocrine neoplasia. The preoperative stabilization of the child with alpha antagonists, fluid replacement, and beta-blockers are the mainstay of preoperative preparation. Intraoperative disasters are well known in the absence of adequate preparation. Conventional procedure has been the standard surgical approach. Minimally invasive surgery (MIS) in children for pheochromocytoma is evolving. We report a series of five children treated over 5 years by the minimally invasive approach with follow-up details for this period. This study confirms the efficacy of MIS approach in treatment of pheochromocytoma and its ability to produce reliable results in the long term.
Introduction
Pheochromocytomas are tumors arising from chromaffin cells of the adrenal medulla first described by Frankel in 1886. 1 The clinical features of the disease result from excessive catecholamines secreted by the pheochromocytes. Pheochromocytoma contributes to about 1% of pediatric hypertensive patients. 2 Incidence of pheochromocytoma is reported as 1 in 10 million children with malignant pheochromocytoma in approximately 2 per 100 million children. 3 It can be sporadic or associated with familial syndromes such as neurofibromatosis type 1 and Von Hippel–Lindau disease. Bilateral tumors have difficult management options ranging between unilateral adrenalectomy, contralateral cortex sparing surgery to bilateral adrenalectomies with their respective disadvantages.
Over the past two decades, there has been a transition from open surgery as the mainstay of surgical management for adrenal surgeries to minimally invasive approaches. 4 Minimal invasive adrenalectomy is now a preferred surgical approach for most adrenal pathologies, particularly lesions smaller than 5–6 cm. 5 In recent years, with the advent of robotic surgeries, there has been a shift to robotic adrenalectomies. 6 There are few studies on this approach in children, without follow-up clinical data. 6,7
This is the first case series on minimally invasive surgery (MIS) for pheochromocytoma using robotic approach with long-term follow-up being reported from Asian continent.
Materials and Methods
This is a case series of five patients found to have pheochromocytoma based on biochemical, imaging, and histopathology reports in our institute from 2018 to 2023. Their files and outpatient records were studied in detail and have been reviewed. The clinical data on the children were analyzed on the basis of age, sex, presentation, preoperative investigations, and treatment. Further preoperative biochemical and radiologic imaging studies were recorded. The operative videos were reviewed for technical details. Postoperative treatment details, including medications administered and clinical recovery till discharge, were collected from the medical records. Follow-up clinical data were recorded from the outpatient records.
Results
There were five children found to have pheochromocytoma included in this study between 2017 and 2023. There were four boys and one girl. Age of the children was between 7 and 13 years. The average height was 138 cm (124–158 cm). The average weight was 28.8 kg (21.6–41 kg) (Table 1).
Age, Gender, Height, and Weight of the Patients
Most common presentation was headache and palpitation, seen in four of the five children. Two children also complained of increased sweating, even at rest, and one child had weight loss (Table 2). Four children were initially evaluated elsewhere with hypertension and were started on oral hypertensive drugs before being referred to our institute (Table 3). Of them, 3 children were treated beyond 6 months (8 months, 1.5 years, and 3 years) before being evaluated and then found to have pheochromocytoma and referred to our institute. One child was incidentally found to have a mass in abdomen after history of fall when she presented in the emergency department.
Clinical Presentation of the Children
Blood pressure percentile at time of presentation as per Clinical Practice Guideline for Screening High Blood Pressure in Children and Adolescents
All patients were evaluated with basic investigations of complete blood count and renal and liver functions. Tumor-specific investigations were 24-hour urinary metanephrines, urinary normetanephrines, and urinary vanillylmandelic acid (VMA), which were performed in all patients except one child who had presented as an incidentally detected tumor following trauma (Table 4). She had later undergone an ultrasound (USG) abdomen guided biopsy to establish diagnosis. Further radiodiagnosis with USG abdomen was done in all patients (Fig. 1) followed by either contrast enhanced CT (CECT) or positron emission tomography and CT (PET CT) using fluorodeoxyglucose (FDG) or 68Ga-labeled DOTA(0)-Tyr(3)-octreotide (68Ga-DOTATATE) radioisotopes to establish the origin, size, and extent of lesion, metastasis, and so on (Figs. 2 and 3). One child had been evaluated with USG and CECT abdomen outside, which was suggestive of left-sided pheochromocytoma. But 68Ga-DOTATATE scan picked up tumor activity in the contralateral adrenal gland (Fig. 4).

USG abdomen is the first line of noninvasive radiodiagnosis, which helps in identifying the tumor. USG = ultrasound.

CECT urography showing right suprarenal pheochromocytoma—

CECT abdomen showing left large adrenal tumor with internal hemorrhage following trauma. CECT = contrast enhanced computed tomography.

CT urography
Biochemical Evaluations and Radiodiagnosis Performed in the Patients
VMA = vanillylmandelic acid; USG = ultrasound; CECT = contrast enhanced computed tomography; PET = positron emission tomography.
All patients were reviewed by the pediatric oncologist and pediatric endocrinologists. The children were then admitted 7 days before procedure and started on phenoxybenzamine with fluid resuscitation with crystalloids/fresh frozen plasma. Beta-blocker (propranolol) was started 2 days before operation mainly for stabilizing the heart rate. All children had heart rate below 100 preoperatively with blood pressure control in near normal range on differing doses of alpha blocker, beta-blocker, and fluid replacement. With adequate priming of patients with fluids and beta-blockers, there were no unexpected complications encountered intraoperatively. The child who had a large tumor with intra-tumor rupture had significant volume loss (of approximately 500 mL), for which adequate blood products were transfused on table.
Four patients had robotic adrenalectomy, whereas one child had laparoscopic adrenalectomy. The decision for robotic or laparoscopic adrenalectomy was as per the parents’ decision following detailed counseling of both with pros and cons. All patients had a transperitoneal approach. One child with a relatively large tumor >6 cm had to be converted to open surgery because of extensive adhesion with surrounding viscera.
Robotic surgeries had the standard four port placement, including the camera port, two working ports, and an assistant port, using the da Vinci Xi system (Fig. 5). There were 3 ports in the child who had laparoscopic adrenalectomy. The average time of operation was 230 minutes (ranging from 145 minutes to 315 minutes, depending on the size of tumor). Three patients had right adrenal tumor, one patient had a left adrenal tumor, and one child had bilateral adrenal involvement (Table 5). The child with left malignant pheochromocytoma also underwent left nephrectomy as the tumor was invading into the left kidney and frozen section biopsy was suspicious of tumor extension.
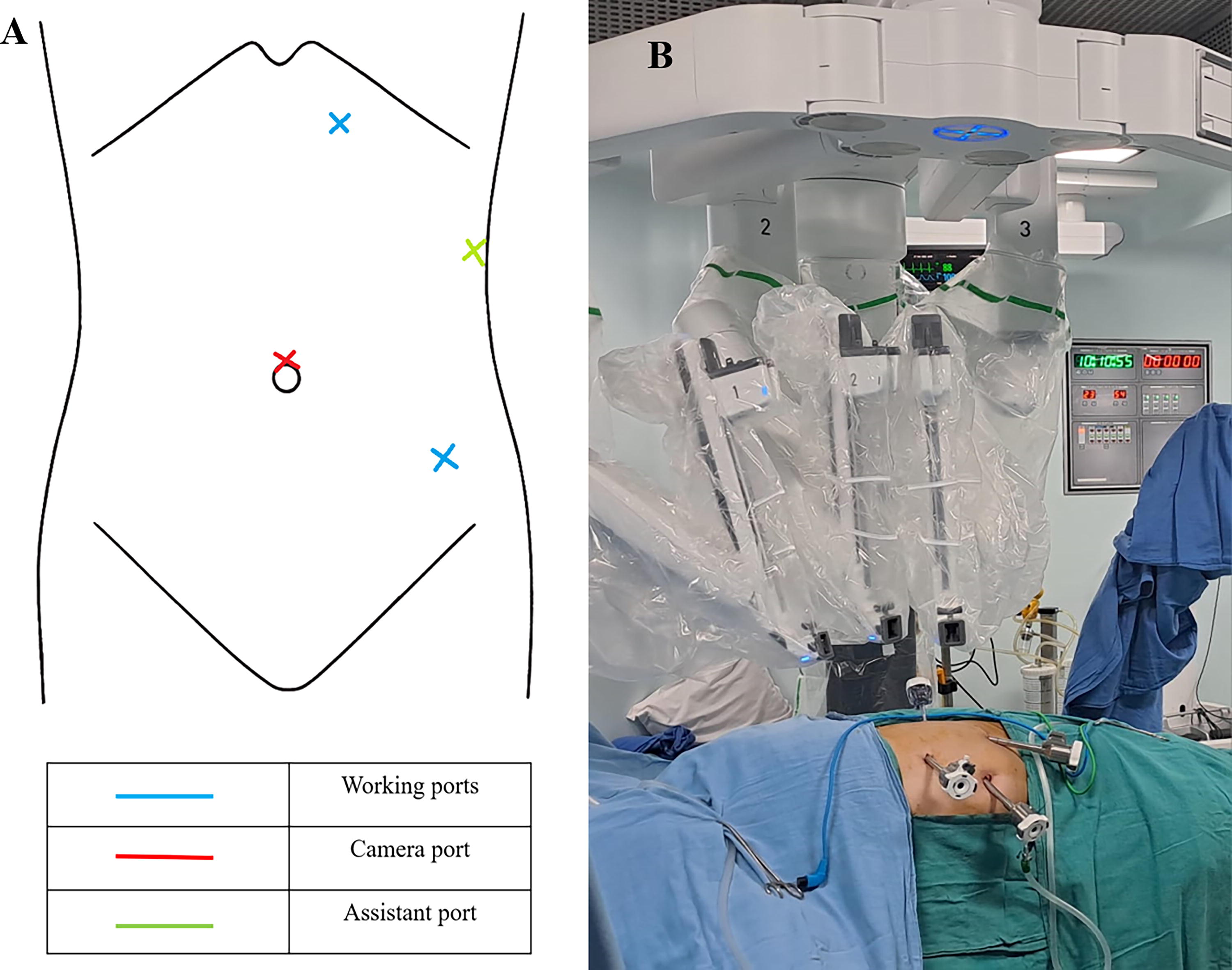
Port placements in robotic adrenalectomy (left side).
Laterality, Size of Tumors as per CT/ PET CT, Intraoperative Duration, Blood Loss, Blood Products Transfused, Postoperative Hospital Stay, and Follow-up of Each Patient
PET = positron emission tomography; CT = computed tomography; PRBC = packed red blood cells; FFP = fresh frozen plasma.
All surgeries were performed by single surgeon, hence eliminating surgeon bias. All the patients were extubated immediately after procedure. In the immediate postoperative period, two children remained normotensive; one child had severe hypotension requiring inotrope support, which was gradually weaned over 3 days and stopped. Two children were having hypertension and were started on antihypertensive drugs orally. Four patients had localized tumor, whereas 1 child with malignant pheochromocytoma had late metastatic disease involving the lungs and spine 9 months after operation. She had complete resection at operation with tumor-free margin. She did not receive any adjuvant therapy as recommended by the established protocol and our pediatric oncologist.
When she presented with weakness in left leg 12 months after procedure, there were FDG-positive lesions on PET CT at the previous surgical bed, contralateral adrenal gland, and spinous involvement. She underwent D9 to L1 laminectomy and decompression of extradural tumor. She finally succumbed to the disease, 3 months later. The other four children had only localized tumors and have been on regular follow-up with no further recurrences and doing well. The child who underwent bilateral adrenalectomy for bilateral pheochromocytoma is on follow-up for 4 years with steroid support.
Discussion
Pediatric pheochromocytomas are rare, with rate of malignancy for adrenal pheochromocytoma ranging from 8.3% to 13.1% and 32% to 42% for extra-adrenal pheochromocytoma. 2 Various germline mutations, such as VHL, SDHB, SDHD, multiple endocrine neoplasia 2, or NF1 genes, have been attributed in pheochromocytoma. 3
Although there are various protocols formulated in the management of pheochromocytoma which include the European Society of Endocrinology, American Association for Clinical Chemistry, and so on, there is no consensus guidelines on the management of pheochromocytoma. 8 Early diagnosis and total excision are the most important aspects of accurate treatment for childhood pheochromocytoma. 2,9
Children with pheochromocytoma present with headache, sweating, flushing, palpitations, gastrointestinal disturbance, weight loss, symptoms of mass effect, or as incidental finding (Table 2). Hypertension is the most consistent sign, which is sustained and without paroxysms in 63%. 3,10 Four patients in our study had hypertension on presentation, with three children already on antihypertensives (Table 3). Despite improved diagnostic techniques, there is an estimated delay of 3 years between initial symptoms and a final diagnosis because of nonspecific symptoms and rarity of the disease. 11
Criteria for malignancy include the invasion of adjacent organs, size of tumor, fixation, contours, heterogeneity, venous invasion, lymphadenopathies, density greater than 20 HU, slow washout (>or <10–15 minutes), and the presence of metastasis. The tumor size is an important factor in establishing malignancy. Tumors with diameters ≥4 cm, ≥6 cm, and ≥8 cm are considered to have a malignant potential of 20%, 65%, and 89%, respectively. Surgery is not always curative in metastatic pheochromocytoma and will need to be combined with chemoembolization, cryoablation, or radiofrequency techniques. 12
The laboratory diagnosis of pheochromocytoma is based on the serum and urinary levels of catecholamines or their metabolites. The combination of urinary metanephrines and VMA has a diagnostic sensitivity of 98% in detecting pheochromocytoma. 2 Other investigations like serum adrenaline and noradrenaline levels and serum chromogranin A also help in diagnosis. 13 –15 In our study, all children had urinary catecholamines assessed.
CT scan is the preferred imaging modality because of its spatial resolution than MRI. 16 Functional imaging provides higher specificity particularly for multifocal or metastatic diseases. Depending on the type of ligand, single photon emission computed tomography isotopes are used, including iodine-123-metaiodobenzylguanidine (123I-MIBG),18F-fluorodeoxyglucose (18F-FDG), 18F-fluorodihydroxyphenylalanine (18F-FDOPA), and 68Ga-DOTATATE. 16,17 In our study, one child had a bilateral pheochromocytoma, which was initially missed in the USG and CT urography which was later picked up in the 68Ga-labeled DOTA scan.
Preoperative blood pressure stabilization ensures intraoperative stability of blood pressures and reduces mortality rate to less than 1% if a team of experienced pediatricians, endocrinologists, anesthesiologist, and skillful surgeons are involved. 11 Phenoxybenzamine was started and continued for 7–14 days following which procedure was planned to ensure cardiovascular stability. Administering crystalloids or plasma along with phenoxybenzamine restores diminished plasma volume and prevent postoperative hypotension. β-Adrenergic receptor blockers are added to control tachycardia and anesthesia-related arrhythmias. 18
Adrenal surgeries have undergone a revolution with the implementation of laparoscopy in 1992 and robotic technology in 1999, 19 although adoption in pediatric world has been later. Laparoscopic adrenalectomy can be considered to be equally safe and effective in pediatric patients as in adults. 20,21 There are three approaches as follows: lateral transperitoneal adrenalectomy, prone retroperitoneal adrenalectomy, and lateral retroperitoneal adrenalectomy. In our study, all the five children had transperitoneal approach as the tumors were well localized with no metastasis.
There are few case reports and series on robot-assisted adrenalectomies in pediatric population till date (Table 6). 6,7 Robotic access ameliorates many limitations of laparoscopic procedure, including two-dimensional vision, loss of depth perception, rigid instruments, and only four degrees of freedom. Although robotic surgeries have extra time involved in docking the robot, this can be overlooked given the advantages of robotic approach over laparoscopic approach. 22 In addition, large tumors (greater than 6 cm), enlarged veins, and densely adherent tumors which are considered difficult to excise by laparoscopic techniques can be accessed with robotic surgeries. 22,23
Comparison with Other Robotic and Robot-Assisted Laparoscopic Adrenalectomy
This study included robotic adrenalectomies in nonendocrine tumors.
A meta-analysis done by Zawadzka K and associates compared outcomes in patients who underwent total bilateral adrenalectomy and partial adrenalectomy in bilateral tumors. 24 They reported that all patients undergoing bilateral adrenalectomy were steroid dependent, whereas approximately two-thirds did not require steroid supplementation after partial adrenalectomy. Despite adrenal-sparing techniques, some part of the adrenal cortex loses the ability to endogenously synthesize adrenal hormones. Preservation of residual cortical function to avoid adrenal insufficiency has to be weighed against the risk of local recurrence, which is higher after partial adrenalectomy. However, there is no significant difference in metastasis or mortality rate between the two groups. 24 In our study, we had one child with bilateral pheochromocytoma for whom bilateral adrenalectomy was performed. Now at 5 years follow-up, child is doing well with no further tumor recurrence.
According to a study by Mitra and colleagues, there is significant heterogenicity in operative times based on surgical approach between laparoscopic (77–256 minutes), posterior retroperitoneoscopic (51–214 minutes), and open (85–180 minutes) procedures. 6 The surgeons’ experience, first assistant training level, and tumor size are independent factors associated with mean operative time and estimated blood loss. 19
In our study, the median time of operation was 235 minutes (including induction of anesthesia, intubation, positioning, port placements, docking and doffing of the robot, and wound closure to extubation). The size of the tumor was a major factor in determining the duration of procedure. Larger tumors required more dissection and hemostasis from the feeding vessels. The average postoperative stay was 8 days.
Aliyev and associates in their study demonstrated that the robotic and laparoscopic groups were similar regarding postoperative narcotic and nonsteroidal anti-inflammatory drug use. 22 It is well established now that laparoscopic approach is as safe as open adrenalectomies even in pediatric populations. 25 But cost is a concern for the use of the robot in general surgical procedures. 22 In comparing the robotic and laparoscopic approach, robotic adrenalectomy remains highly debated because of the cost and duration of operation. 6,26 The risk of tumor recurrence in the remnant adrenal gland is 10%; metachronous tumor development in the contralateral adrenal gland is 30% in patients with hereditary forms of pheochromocytoma. All patients should be followed up annually for at least 10 years after procedure. 11 In our study, one child was tumor free at 6 months follow-up (screened with USG and PET CT). But at 12-month follow-up, she had new lesions on the contralateral adrenal and ipsilateral tumor bed with bony metastasis. This child later succumbed to the disease. The follow-up period for the remaining children ranges from 5 years to 6 months (Table 6). All children have been doing well.
Conclusion
Pheochromocytoma is a rare and life-threatening disease in children, presenting with uncontrolled hypertension. Initial stabilization of blood pressures and adequate hydration preoperatively minimize perioperative hemodynamic risk. Robotic operation as a minimally invasive approach for tumors less than 6 cm is a safe, effective, and reliable option. Lifelong follow-up is recommended.
Footnotes
Authors’ Contributions
C.C.: Methodology, formal analysis, data curation, and writing—original draft; A.P.: Methodology, data curation, and formal analysis; D.K.K.: Methodology, data curation, and interpretation of data; P.Y.: Methodology, data curation, and formal analysis; A.M.: Methodology, data curation, and formal analysis; S.K.C.: Conception, design of work, analysis, interpretation of data, reviewing, writing—original draft, and reviewing and editing.
All authors are in agreement for the accountability of all aspects of work regarding accuracy and integrity.
Author Disclosure Statement
There are no financial or personal relationships that may inappropriately influence the publication of the article or integrity of the research reported.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.