
Abstract
Objective:
To evaluate the efficacy of preserving urethral mucosa around verumontanum in all directions and at the prostatic apex on antegrade ejaculation preservation and early postoperative continence in patients undergoing transurethral resection of the prostate (TURP).
Materials and Methods:
A randomized controlled trial was conducted in our tertiary center on patients scheduled for TURP. Patients were randomly allocated into two equal groups. Group A represented the control group who underwent conventional TURP, while Group B represented the ejaculation-sparing TURP. Patients were followed up for 3 months postoperatively to evaluate the voiding parameters and the preservation of antegrade ejaculation.
Results:
A total of 106 patients were evaluated in our study. Both groups were comparable regarding improvement in voiding parameters. Antegrade ejaculation was preserved in 44 patients (83%) of Group B compared with 10 patients (18.9%) in Group A with a highly statistically significant difference (p < 0.001). Early postoperative urge urinary incontinence was lower in group B (5.7%) compared with (20.8%) in group A, with a statistically significant difference (p = 0.02). Other perioperative parameters were compared between both groups.
Conclusion:
The ejaculation-sparing technique adopted in our study showed a promising result for preserving antegrade ejaculation following TURP with a success rate of 83%. Additionally, there was a lower incidence of early postoperative urge urinary incontinence.
Introduction
Benign prostatic hyperplasia (BPH) is a common disease in elderly men, and transurethral resection of the prostate (TURP) is still the gold standard surgical intervention for BPH. However, retrograde ejaculation is a common complication, with a reported incidence of 66% to 86% in sexually active patients. Moreover, early postoperative urge incontinence (UI) may occur in up to 30% to 40% of patients with continence improvement over time, while persistent incontinence occurs in fewer than 1% of cases. These complications are associated with significant disappointment for the patients and unpredictability and uncertainty in the recovery period that cause considerable anxiety to surgeons. 1 –3
Ejaculatory dysfunction results from disrupting the anatomy around the verumontanum, especially the proximal part and the muscular tissue surrounding the verumontanum, rather than bladder neck closure. 4 –6 Early incontinence is usually related to the healing process in the prostatic fossa, urinary tract infections, patient age, or detrusor overactivity caused by long-lasting bladder outlet obstruction. External urethral sphincter damage is the main reason for persistent urine incontinence following prostatectomy, either because of direct injury or because of energy dispersion of the electrocautery. 2,7 –9
Instead of managing these complications, various technologies and surgical techniques were proposed to avoid or minimize the incidence of such complications. Previous studies have evaluated various ejaculation-preserving techniques with promising results. 10 –14
Our study aims to evaluate the efficacy of preserving urethral mucosa around verumontanum in all directions and at the prostatic apex on retrograde ejaculation and postoperative urine continence in patients following TURP.
Materials and Methods
A randomized controlled trial was conducted in our tertiary center between May 2023 and January 2024. After obtaining ethical approval, 106 patients were enrolled in our study from those who attended the outpatient clinic and were scheduled for TURP.
Inclusion criteria were patients with prostate size less than 100 g (as evaluated by pelviabdominal ultrasound) and scheduled for TURP because of refractory retention, recurrent gross hematuria of prostatic origin, failed to respond to medical treatment, recurrent infection, and patients with bladder calculi secondary to bladder outlet obstruction. Patients were required to be sexually active with intact antegrade ejaculation. Patients with neurogenic bladder, detrusor hypocontractility, urethral stricture, prostate cancer, or previous prostatic intervention were excluded from our study.
After patient counseling regarding the surgeries, patients were randomized into two equal groups using a sealed envelope prepared by a separate committee not involved in the study with a 1:1 ratio. Patients, as well as team members involved in the data collection and statistical analysis, were blinded to the type of intervention.
The preoperative evaluation was done on all patients, including careful history taking, general exam, digital rectal exam, prostate size evaluation by pelviabdominal ultrasound, prostate-specific antigen, maximum flow rate (Qmax), post-void residual (PVR), International Prostate Symptom Score (IPSS), and quality of life (QoL) data. All the included patients were sexually active from history, and none of them had a preexisting ED or retrograde ejaculation.
Patients in group A underwent conventional bipolar TURP. 1 Patients in group B underwent ejaculation-preserving TURP; the surgery was as follows: The verumontanum is identified, and with the cutting current, a mark is made on the urethral mucosa 1 cm proximal to the verumontanum in all directions. Standard resection of the middle lobe, lateral lobes, and the apical prostatic tissue is performed sparing the marked urethral mucosa. Apical prostatic tissue was resected lateral to the spared urethral mucosa to ensure proper relief of outlet obstruction. At the end of the surgery, 1 cm urethral mucosa was spared all around the verumontanum, including the prostatic apical urethral mucosa, while having an adequately resected prostate.
Operative time, hospital stay, catheter removal time, and perioperative complication for both surgeries were documented. Catheter removal was planned for all our patients following 24–48 hours, depending on the presence or absence of hematuria, unless a catheter was indicated for a longer duration, such as capsular perforation or persistent hematuria. Postoperative evaluation at 1 and 3 months was conducted, including voiding and ejaculatory function assessment by ICIQ-SF score for urine incontinence, MSHQ score for ejaculatory function, IPSS score, and QoL. Uroflowmetry and pelviabdominal ultrasound were done at 3 months for prostate size and residual urine evaluation.
Our primary outcome measure was to evaluate postoperative ejaculatory function in both groups. Our secondary outcome measures were to evaluate early postoperative urine continence, perioperative complications, and other voiding parameters.
Statistical analysis
Data were gathered, reviewed, coded, and inputted into IBM SPSS version 27 for analysis. Quantitative data were reported as mean and standard deviations. Qualitative variables were represented as numbers and percentages. Group comparisons for qualitative data utilized the Chi-square test and/or Fisher exact test when the expected count in any cell was less than 5. For two independent groups with quantitative data and a parametric distribution, the independent t-test was employed, while the nonparametric distribution was evaluated using the Mann–Whitney U test. Comparisons between paired groups with quantitative data and a parametric distribution were conducted using the paired t-test, and for nonparametric distribution, the Wilcoxon rank test was applied. The confidence interval was set at 95%, and a margin of error of 5% was accepted. A p < 0.05 was deemed statistically significant.
Results
One hundred and six patients were randomly allocated into two equal groups, as shown in Figure 1, and they were followed up for 3 months postoperative. Preoperative data were similar in both groups, as shown in Table 1 regarding age, IPSS, QoL, Qmax, post-voiding residual urine, and prostate size.
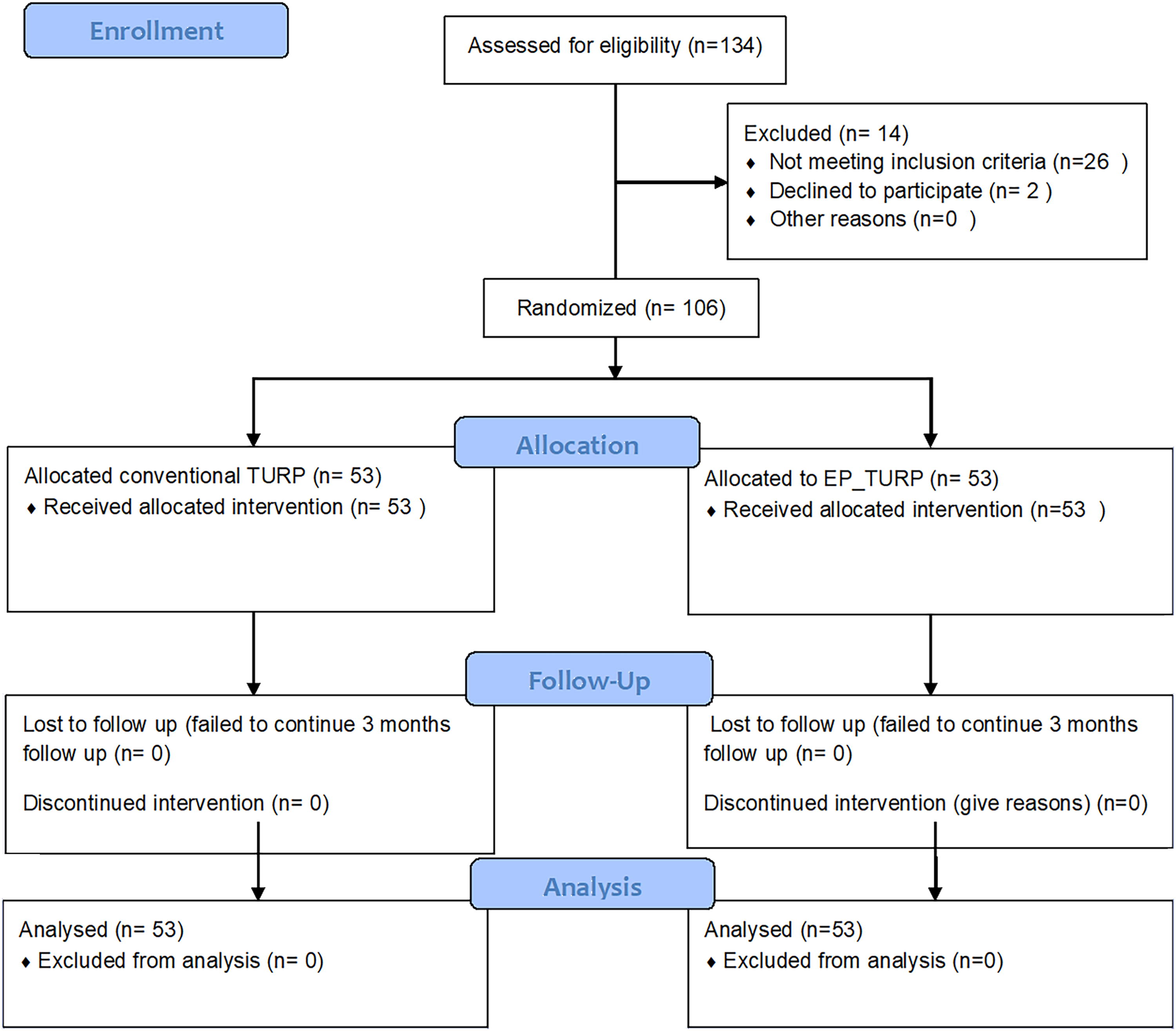
Consort flowchart.
Preoperative Data
IPSS = International Prostate Symptom Score; Qmax = maximum flow rate; QoL = quality of life.
Perioperative parameters are demonstrated in Table 2. Both groups had a comparable improvement in the voiding parameters, with statistically significant differences in the IPSS, QoL, Qmax, post-voiding residual urine, and prostate size reduction. Operative time, hospital stay, and catheter removal time were similar in both groups. Preserved antegrade ejaculation was seen in 44 patients (83%) of Group B compared with 10 patients (18.9%) in Group A with a highly statistically significant difference (p < 0.001).
Perioperative Parameters
IPSS = International Prostate Symptom Score; Qmax = maximum flow rate; QoL = quality of life.
Perioperative complications were reported in Table 3. We did not record any case of a failed trial of micturition following both procedures, and there was no recurrence of urine retention during our follow-up period. Early postoperative urge urinary incontinence was seen less in group B in only 3 patients (5.7%) compared with 11 patients (20.8%) with a statistically significant difference (p = 0.2) which was improved during follow-up in both groups and failed to show any significant difference at 3 months postoperative. Apart from ejaculatory dysfunction and early urine incontinence, other perioperative complications were comparable between both groups.
Perioperative Complications
Discussion
Ejaculation plays an important role in the overall quality of sexual life, and the absence of antegrade ejaculation is considered one of the drawbacks of TURP. Therefore, sexually active patients may delay or avoid the TURP procedure or seek other less effective ejaculation-sparing s such as water vapor thermal therapy, prostatic artery embolization, or prostatic urethral lift to preserve their ejaculation. 15 –18
Vernet et al. explained the mechanism of ejaculation, using endorectal ultrasound during ejaculation. Antegrade ejaculation takes place by the caudal shift of the verumontanum to contact with the adjacent urethral wall rather than bladder neck closure, then the semen emitted from the ejaculatory ducts is forced in antegrade direction by proximal closure of the verumontanum and surrounding tissue with the coordination of rhythmic muscle contractions between the bulbospongiosus muscle and the external urethral sphincter. 19 From this consensus, sparing the tissues around the verumontanum, named the ejaculatory high-pressure area, contributes to preserving ejaculation post-TURP rather than bladder neck sparing. 6,15
There is no agreement regarding the optimum ejaculation-sparing technique. We planned our TURP procedure to spare 1 cm of urethral mucosa all around the verumontanum, including the prostatic apical urethral mucosa, to evaluate its impact on the preservation of post-TURP antegrade ejaculation and early UI.
Different trials have proposed various ejaculation-sparing techniques. Lebdai et al presented a consensus statement of 15 experts to define the areas to be resected or preserved to achieve both relief of obstruction and ejaculation preservation. They propose sparing 2 cm mucosa along with the posterior part of the prostatic urethra proximal to the verumontanum to achieve this goal. Based on this consensus, the authors have proposed the PARTURP study, a prospective randomized study with a 3-year follow-up, comparing partial to complete TURP. 14
Alloussi et al. adopted a technique that included sparing the paracollicular tissue and 1 cm proximal to the verumontanum or just bladder neck resection in those with bladder neck obstruction. 11 Zhang et al. evaluated the sparing of the tissues between 5 and 7 o’clock from the bladder neck to the verumontanum. 12 Ben Rhouma et al. proposed the preservation of 1 cm urethral mucosa around the supramontanal prostatic tissue. 20 Ronzoni et al. evaluated the preservation of the supramontanal prostate and the area of the prostatic urethra for >1 cm from the verumontanum. 21
In our study, 106 were randomized into two equal groups and evaluated at 1 and 3 months postoperative. Both groups were similar in the preoperative parameters. The improvement in postoperative voiding parameters, including IPSS, Qmax, and PVRU, was equivalent in both groups, as shown in Table 2 with a significant improvement compared with the preoperative parameters. Postoperative prostate size, hospital stay, blood loss, and catheter removal time were similar in both groups.
In our study, ejaculation preservation was evaluated at 1 and 3 months. Preservation of antegrade ejaculation in the intervention group B was 83% (44 patients out of 53) compared with 18.8% (10 patients out of 53) in the control group A. The ejaculatory function was evaluated in both groups with MCHQ score until 3 months postoperatively, with a highly statistically significant difference between both groups (p < 0.001).
Our results were comparable to those of Alloussi et al., who reported the preservation of ejaculation in their study over 60 months in 90% of their patients. 11 Ben Rhouma et al.’s study showed 65.7% ejaculation preservation in the intervention group compared with 28.6% in the conventional TURP group after 3 months of follow-up. 20
El Shazly et al. evaluated ejaculation preservation by performing a bladder neck and supramontanal sparing of 5 mm paracollicular tissue in a randomized controlled trial vs conventional TURP. Preservation of ejaculation was 80% in the intervention group compared with 27% in the control group. 22 Manasa et al. reported ejaculation preservation of 88.89% in the bladder neck and supramontanal sparing TURP compared with 22.22% in the conventional TURP. 13
Regarding post-TURP urinary continence, Zinner et al. demonstrated the role of urethral mucosa in the continence mechanism. Compared with conventional prostatic resection, urethral mucosa preservation at the prostatic apex increases the length of the urethral mucosa and the number of mucosal folds near the external urethral sphincter. This coaptation acts as a sealing pad, which reenforces the external urethral sphincter, increases the urethral closure pressure, and leads to better urinary continence. 23
In our study, only 5.7% of patients in the ejaculation-sparing group developed urge urinary incontinence in the first month following catheter removal compared with 20.8% in the standard TURP group, a statistically significant difference (p = 0.02). Continence rates improved over 3 months to 1.9% and 5.7% in the ejaculation-sparing and control groups, respectively, with no statistically significant difference.
Liang et al. evaluated transurethral prostatic resection with the sparing of urethral mucosa at the prostatic apex. Less postoperative urine incontinence was encountered following catheter removal in the sparing of urethral mucosa at the prostatic apex with a statistically significant difference. 24 Liu et al. reported a reduction of postoperative urinary incontinence to nil with the urethral mucosal preservation at the prostatic apex compared with 22.5% in the convention TURP. 25
Our study recorded no significant differences between the two groups regarding prostate size reduction, operative time, hospital stay, catheter removal time, and other perioperative complications.
The ejaculation-sparing TURP technique adopted in our study showed a success rate of 83% in preserving antegrade ejaculation following TURP, with an additional lower incidence of early postoperative urge urinary incontinence.
As the instruments and energy sources used in the TURP procedure have evolved. The resection technique has also evolved to cope with the demands and patients’ expectations without compromising the safety or efficacy of the procedure. This modification in the resection technique is a reasonable option for those patients who desire to preserve their ejaculation following TURP.
This study is not devoid of limitations as it was a single-site study with a relatively small sample size. A short-term follow-up was done to evaluate the efficacy of ejaculation sparing. However, a longer follow-up is needed to assess the durability of the procedure in improving patients’ voiding and to detect the impact on the retreatment rate.
Footnotes
Authors’ Contributions
A.M.T. and A.H. contributed to the study design and protocol application and processing. In addition to article writing mainly in the discussion section and literature search. A.M.I. and A.R. contributed to data collection and analysis and writing the results and discussion section with the final outline of the article. M.E. and K.O.E. made the final revision of the article and critical appraisal of it. All authors read and approved the final version of the article. All authors contributed equally to the article and read and approved the final version of the article. Our article has not been published previously or is under consideration for publication elsewhere.
Ethical Consideration
Ethical committee approval was obtained before commencing the study from the faculty of medicine, Ain Shams University, with approval number: MS 319/2023. Patients were counseled before enrollment and consented to the treatment options. The trial was registered at clinicaltrial.gov. clinical trial registration number: NCT06263049.
Consent for Participation
Written consent was obtained from all patients’ parents or legal guardians before participation.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the article.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.