
Abstract
Introduction:
Our comprehension of the actual diversity of kidney pyelocaliceal system (PCS) is lacking and many crucial features have been overlooked in the existing literature on this subject. The purpose of this review is to provide a concise summary of the current understanding of the structure of the pelvicalyceal system, considering both anatomical and surgical perspectives, as well as to highlight any limitations or inconsistencies in these approaches.
Material and Methods:
A full review of all the literature on the anatomical and surgical methods used to classify pelvicalyceal system was conducted in several databases in August 2024. This included all the articles that talked about classifications for the whole pelvicalyceal system, minor calyces, and morphometric measurements within the pelvicalyceal system.
Results:
Despite over a century of studying this anatomical zone and numerous approaches, some classifications still rely on pelvic branching or the division site related to the renal sinus. However, no single classification has incorporated both aspects. In addition, despite the consensus regarding the number of minor calyces, there are many approaches to determining their orientation. Finally, researchers have described a sufficient number of morphometric measurements within the pelvicalyceal system, considering their prognostic value before endourological interventions and their correlation with individual patterns of the structure of pelvicalyceal system. However, these measurements often lead to contradictions in interpreting the anatomical favorability of the same pelvicalyceal system using different approaches.
Conclusion:
Despite the numerous approaches to identify pelvicalyceal system from both morphological and surgical perspectives, there are significant gaps in our understanding of the real anatomy of the renal cavity that, even after more than a century, remain unanswered. There needs to be more correlation of anatomy with modern minimally invasive clinical interventions for stone disease.
Introduction
Urologists have a diverse array of minimally-invasive and even extracorporeal interventions at their disposal for treating different upper urinary tract diseases. 1,2 These interventions, made possible by advancements in technology, have largely replaced the need for open surgery. 3 As a result, patients experience significantly less trauma while still benefiting from highly effective treatments. Meanwhile, with the introduction of new tools and equipment, there has been a significant advancement in understanding the variability of the pyelocaliceal system (pelvicalyceal system) anatomy. It is now evident that a thorough knowledge of the anatomy of the kidney cavity is essential for selecting an appropriate surgical approach and improving the likelihood of successful treatment. Different anatomical and surgical classifications of pelvicalyceal system exist. The first encompasses numerous categorizations for delineating certain types of pelvicalyceal system, whereas the latter entails the establishment of distinct threshold values for quantifying the dimensions and angles in different sections of the renal cavity. There are numerous studies that focus on the different approaches to imitating pelvicalyceal system or predicting related events, ranging from the creation of various simulators to conducting experimental research on them, as well as utilizing advanced digital technologies such as artificial intelligence (AI). 4 –6 Nevertheless, while conducting an in-depth analysis of the aforementioned categories of methodologies used in classifying pelvicalyceal system, numerous inconsistencies and contradictions became apparent. This suggests that our comprehension of the actual diversity of this structure is lacking and that many crucial features have been overlooked in the existing literature on this subject. The purpose of this review is to provide a concise summary of the current understanding of the structure of the pelvicalyceal system, considering both anatomical and surgical perspectives, as well as to highlight any limitations or inconsistencies in these approaches.
Material and Methods
Search strategy
In August 2024, comprehensive review of the anatomical and surgical approaches to classify pelvicalyceal system was performed in PubMed, Google Scholar, Embase, and SciELO with the use of Boolean operators and following terms: “kidney,” “renal,” “cavity,” “pelvis,” “pelvicalyceal,” “pyelocaliceal,” “pelvicalyceal system,” “infundibulum,” “calyx,” “anatomy,” “upper,” “middle,” “lower,” “classification,” “types,” “variation,” “visualization,” “CT,” “3D,” “intravenous urography,” “IVU,” “cadaver,” “endocast,” “orientation,” “plane,” “angle,” “length,” “width,” “shape,” “impact,” “outcome,” “measurement,” “PCNL,” “URS,” “Ureteroscopy,” “RIRS,” “endoscopy,” “ESWL,” and “SWL.” To deeply investigate the topic, all references cited by searched articles were thoroughly analyzed, and the snowball technique was also used, as previously described. 7
Inclusion criteria were English-written articles, abstracts of non-English articles but available in English, reviews, original studies and comments, and description of anatomical and/or surgical approaches to classify pelvicalyceal system in normal adult kidneys, without restrictions on the publication date.
Exclusion criteria were abstracts of non-English articles or articles not available in English, studies on anomalous kidneys, and/or nonadult human kidneys.
Data extraction and analysis
We did not conduct a quantitative and systematic review of the research, instead focusing on a multidimensional investigation of approaches to pelvicalyceal system categorization from both anatomical and surgical perspectives. Rather, we conducted a thorough analysis of existing data without strict exclusion criteria to identify true evolution in our understanding of structural variants of the pelvicalyceal system, identification of characteristic patterns, and approaches to measuring individual compartments of the kidney cavity as predictors of surgical outcomes. Based on the obtained data, a primary review structure (A.T.) was developed, which was revised by three experts (B.K.S., B.M.Z.H., and P.J.). It should be noted that because of the use of different terms to describe pelvicalyceal system by authors (pelvicalyceal, pelvicaliceal, pyelocalyceal, pyelocaliceal), all these terms were used when searching for information, but in the text of our review, we used the “pyelocaliceal” term.
Results
As a result of consensus, the presented review is structured as follows: 1) pelvicalyceal system classifications; 2) calyces—general number, shape, and orientation; 3) focus on specific calyceal level—upper, middle, and lower calix.
PCS classifications
Publications from the previous century have discussed the concept of categorizing pelvicalyceal system based on the variety of its anatomical structures (Table 1). Although there is a lack of reliable and detailed methods for observing instruments and directly examining cadaveric kidneys and endocasts, the trends at that time align with more recent suggestions. The metanephros influences the branching of the ureteral bud during the embryonic period, which forms the basis of these trends. This branching determines the initial formation of the pelvis, the number of infundibula, and consequently, the drainage pattern of the small calyces. In 1891, Legueu provided a description of the partition of the pyelus, which refers to the kidney cavity from the papillar region to the ureteropelvic junction (UPJ), into two types: ampullary and dendritic. 8 In 1901, Brödel maintained the same idea by categorizing the renal pelvis into two distinct types: true and divided. 9 Subsequent study of the anatomy of the pelvicalyceal system in the first half of the 20th century led to both attempts at anatomical measurements and the formation of classifications with a large number of variants, which were positioned as intermediate between those previously mentioned. Graves 10 classified them as Type A (the classical Y type), Type B (the inverted T), Type C (the balloon), and Type D (the inverted bagpipes). The work of Lofgren in 1957 is significant in terms of the independence of different portions of the pyelus based on pyramidal pairs rather than the establishment of the classification of pelvicalyceal system. Lofgren advocated separating the pyelus into three components: pars cranialis, corresponding to pyramid pairs 1–3; pars intermedia, corresponding to pyramid pairs 4–5; and pars caudalis, corresponding to pyramid pairs 6–7. 20
Pyelocaliceal System Classifications Based on the Pelvic Division to the Infundibulum
A significant advancement in contemporary comprehension of the anatomy of the pelvicalyceal system is the research conducted by Sykes in 1964. 11 The author analyzed calyceal casts in a study on 300 deceased adult kidneys. These casts were created by injecting vinolyte resin into the ureter. Two types of pelvicalyceal system were mentioned: 1) “double caliceal” type, when cast is divided into two major calyces. The upper major calix was long and slim compared with the lower one and contained the major calix at the extremity. The lower minor calyces drained into the lower and larger major calix, whereas the hilar calyces drained either entirely into the lower major calix or into both major calyces; 2) “pelvic” type of caliceal arrangement, when pelvicalyceal system did not divide into major calyces with direct drainage of minor calyces into an extended pelvis.
A study of equivalent significance was published 2 years later by Fine and Keen, in which they examined endocasts from African, European, and Indian individuals. 12 Out of the 107 casts that were examined, 40 of them displayed distinct upper and lower major calyces together with their corresponding minor calyces. In addition, 35 of the casts exhibited upper and lower major calyces, as well as middle minor calyces that originated from either the upper or lower major calix, or both. Twenty-eight middle calyces were observed, originating either from a third major calix or straight from the pelvis. It was unclear whether these calyces belonged to the upper or lower major calix. Among the four specimens, specifically two pairs of kidneys, the pelvis did not exhibit any division into major calyces. Instead, all the minor calyces originated directly from the pelvis. Also from the branching point of view, but being more specific on the length of the pelvis, Didio described two variations of the pelvis in 1970: long and branchy. 13 In 1957, Mebel was among the first to recognize the pelvis’s position in relation to the renal sinus and proposed the following variations: type I (intrarenal pelvis), type II (extrarenal pelvis), type III (extrarenal pelvis with open posterior surface), type IV (mixed), and type V (no pelvis). 21 Covantsev et al. 21 investigated the macroscopic dissection of 90 kidneys and found the following proportions: 50%, 10%, 20%, 17.78%, and 2.22%, respectively. Bruce et al. 22 classified the pelvis as intrarenal, extrarenal, or borderline. The intrarenal form is located exclusively within the renal sinus, whereas the extrarenal type is situated fully outside of it. The borderline type is characterized by its position, which is partially within and partially outside the renal sinus (Table 2).
Pyelocaliceal System Classifications Based on the Pelvic Position Related to Renal Sinus
During the following 20 years, the medical field dedicated its efforts to comprehending established categorizations and typically concurred with prior authors. However, the identification of novel distinct patterns in the structure of the pelvicalyceal system resulted in the development of the Sampaio and Mandarim-De-Lacerda classification in 1988, which is today the most often used. 14 They classified pelvic arrangements into four types within two groups. Group A is presented by two main calyceal groups (superior and inferior), dividing primarily the renal pelvis, with the middle zone draining on these two major calyceal groups. It consists of two types (AI and AII), depending on the presence of middle zone drainage by two crossed calyces. Group B is presented by pelvicalyceal system with independent middle zone drainage and also consists of two types, whether the latter is drained by a major calyceal group (BI) or by minor calyces directly to the pelvis (BII). As indicated by the authors themselves, the proposed classification is similar to some of those proposed previously, such as by Fine and Keen. 12 However, it is added with a focus on crossing calyces in the kidney mid zone or the consequent formation of the inter-pyelocaliceal space. This classification has been tested by other authors both for the assessment of endocasts and for predicting endourological interventions. So, Marroig et al. 24 obtained 170 resin endocasts from 85 adult cadavers and found 33.53% endocasts of group A1, 13.53% of group A2, 34.71% of group B1, and 18.23% of group B2, whereas type B1 prevailed on A2 in the original study. 14 According to Anjara et al., 23 the frequency of various pyelocaliceal patterns was A1 = 38%, A2 = 12%, B1 = 29%, and B2 = 20%. This proportion differs from the original study by the prevalence of B2 over the A2 rate. Out of the 100 kidneys, one specimen presented with extrarenal calyces with an absent pelvis, and the ureter was found to arise directly from the calyces, which could not be classified. Recently, it was shown that B1 type prevailed on the left, whereas A1 was more common on the right side. 25
In the late 20th century, Szkodziak et al. 15 conducted an analysis of the structure of pelvicalyceal system among subjects from the Lublin region of Poland. This study, which was overlooked by many other studies, is significant for understanding the temporal and regional trends in the classification of the kidney cavity. According to the authors, the latter is represented by the following types: branching (with two subtypes: two- and three-branching), transitional, and ampullar, with the first type being the most common, regardless of gender.
The main work of the first decade of the 21st century regarding anatomical classification is the work by Ningthoujam et al., 16 who proposed the next types when classifying the pelvicalyceal system patterns: multicalyceal (radiate), tricalyceal (triangular), and bicalyceal types (Y-shape). Noteworthy is the fact that in 16% of cases, the anatomy did not correspond to any of the mentioned options. In the already-mentioned study by Anjara et al., 23 the percentages of specimens belonging to each group in this classification were: multicalyceal (23%), tricalyceal (27%), bicalyceal (35%), and unclassified (15%). It is noteworthy that bicalyceal (35%) and A1 (38%) variants are almost identical in frequency, which emphasizes the similarity of approaches in Ningthoujam et al. 16 and Sampaio and Mandarim-De-Lacerda. 14 In contrast to this work, the study by Mishra et al. should be mentioned, 26 in which the tricaliceal type prevailed (50%), whereas unclassified anatomy was presented in 4% of cases. It was also recently stated that bicalyceal and tricalyceal anatomy were found to be more on the left side and multicalyceal anatomy on the right side. 25 Confusing results were published by Krishnaveni et al., 27 who examined 44 adult kidneys that had been preserved with formalin and then injected with a sulfate solution. Radiography was performed on these kidneys. Out of the 23 kidneys examined, multiple calyces were found in all of them, with more than four calyces observed. Among them, 12 kidneys had two major calyces, whereas only 9 kidneys had three major calyces. An arrangement in the shape of a Y was observed in 3 out of 12 cases, whereas a multiple arrangement was observed in 3 out of 23 cases. However, no specific information was provided regarding the differences between the suggested and original nomenclature. Recent investigations have revitalized the classification of the renal pelvis in relation to the renal hilum. Anjara et al. 23 defined the next proportions as 79%, 5%, and 13% for intrarenal, extrarenal, and borderline patterns, respectively. Moreover, the authors proposed to include an additional category of absent pelvis, which was presented in 3%, the extrarenal (5%) and absent renal pelvis (3%). Gandhi and Chavan 28 found that these patterns were present in 48.5%, 21.9%, and 20.9%, respectively, and the absent pelvis was found in 8.7%.
Most recent attempts to classify pelvicalyceal system have focused not only on the patterns of the pelvis and infundibulae but also on the minor calyces. Thus, in 2018, Takazawa et al. 17 categorized each minor calix into five levels: top, upper, middle, lower, and bottom. The upper, middle, and lower calyces were typically found in pairs: anterior and posterior, whereas the top and bottom levels were presented by compound calyces. Consequently, the pelvis was classified into Type I: single pelvis (58%) and Type II: divided pelvis (42%). Type I was subclassified into three types: Type Ia (43%), the standard type with a pelvis/UPJ width ratio near 3; Type Ib (4%), a wide type with a pelvis/UPJ width ratio of 5–10; and Type Ic (11%), a narrow one with a pelvis/UPJ width ratio near 1–2. In Type II, the renal pelvis is always bifurcated into the upper branch (comprising the top and upper calyces) and lower branch (comprising the middle, lower, and bottom calyces). The bifurcation point was always between the upper and middle calyceal groups. If the branch point was inside the straight line between the top and bottom, the pelvis was considered to be Type II. Analyzing reproducibility, the authors revealed that the most common area of disagreement was between Type Ia and Type Ic.
The next step forward was taken by Zhu et al. in 2021. 18 The authors conducted measurements of the attributes of the renal pelvicalyceal system and put up the modified Takazawa anatomical classification. Initially, the cut-off values for the pelvis/UPJ width ratio were adjusted specifically for the A group. A1 (22%), A2 (27%), and A3 (13%) represent pelvicalyceal system with ratios less than 4, between 4 and 16, and greater than 16, respectively. These pelvicalyceal system are referred to as slimline, funnel-shaped, and box-shaped, respectively. Group B was further categorized based on three measurements: type B1 (pelvis/UPJ width ratio <4, infundibulopelvic angle [IPA] > 30° according to Elbahnasy’s approach, and infundibular length [IL] < 3 cm) and type B2 [at least two requirements were not present]).
Finally, last year, Qi et al. 19 published a study on posteriorly oriented minor calyces, and from this point of view, they classified the kidney cavity into three different types: 1) pot-belly type: the renal pelvis is shaped like a pot-belly and is directly associated with cup-shaped minor calyces in the absence of a distinct renal major calix; 2) classical branched type: in this type of posterior group of renal calyces, ≥2 renal major calyces branch to form the renal pelvis; 3) elongated branched type: major renal calyces were branched, with at least 1 major calyceal axis of ≥0.9 cm length and ≤0.3 cm neck width. The morphological typing showed that the percentage of occurrence of these types was 8.06%, 73.13%, and 18.81% among 2642 kidneys, respectively.
Calyces—general number, shape, orientation
Obviously, studying the morphology of the pelvicalyceal system is more accessible and clearer when focused on its “macro” compartments, such as the pelvis, infundibulum, and major calyces, as evidenced by the many different classifications listed earlier. However, the upper urinary tract starts with parts that are directly in touch with the renal papilla, also known as minor calyces. This is why a full study of the pelvicalyceal system’s shape and variation should also include this “micro” area. The direct mention of minor calyces in the classification of pelvicalyceal system is available only in recently published proposals. 17,18 However, authors have been describing attempts to analyze the architecture of small calyces for more than a century, so this is not a new task (Table 3).
Approaches to Classify Minor Calyces
IVU = intravenous urography.
Number and shapes of minor calyces
When studying small calyces, the question of their number causes the least discrepancy. the studied samples typically have a minimum number of 4–5, 11,28 –30 and a maximum number of 11–14, 11,28,30 although there are also examples of 16 small calyces. 29 There is even more consensus when determining the average number of calyces: from 6 to 9 per kidney. 11,17,21,28 –31 The default assumption regarding the shape of the small calyces is that in the absence of significant pyelocalicoectasia, they present as cup-shaped. The number of drained papilla determines whether they are simple or compound. 32 However, a very insightful article was published by Asakawa in 1988, 29 who investigated 100 adult kidney endocasts. According to the neck part of minor calyces, the following types were proposed: 1) neck type: having a tubular portion of funnel-shaped minor calyces or a transitional canal to major calyces, irrespective of its length; 2) half-neck type: having a neck part partially; 3) non-neck type: having no neck part, and the fornix is opening directly in the pelvis or major calyces, presented in 67.5%, 23.5%, and 9.0% of cases, respectively, without side and gender difference.
Orientation of minor calyces
In contrast to quantitative indicators, qualitative indicators, in particular orientation, have been the subject of more debate in the analysis of small calyces. Brodel 9 classified calyces as posterior and anterior, orienting them 20° and 70° behind and ahead of the kidney’s frontal plane, respectively. Hodson 33 expressed opposition, stating that the posterior and anterior calyces align 70° and 20° behind and ahead of the kidney’s frontal plane, respectively. Kaye and Reinke partially explained this apparent contradiction in 1984 34 when they published their analysis, finding that most right kidneys tended to resemble Brodel’s type, whereas the left kidneys typically resembled Hodson’s description. In 1979, Hureau 35 confirmed the antero-posterior (AP) orientation of the minor calyces and named it ventro-dorsal. He also came up with the idea that the major calyceal orientation would be cranio-caudal. Sykes concluded that most calyces directed either anteriorly or posteriorly, whereas the author’s description of compound polar calyces more frequently directed superiorly and inferiorly. 11 This concept persisted even after more than three decades, when Takazawa et al. 17 categorized each minor calix into five levels: top, upper, middle, lower, and bottom. The upper, middle, and lower calyces were typically found in pairs: anterior and posterior, whereas the top and bottom constituted the compound calyces and were oriented within the frontal plane and almost vertically.
However, there is another opinion regarding which plane determines the orientation of the small calyces. Thus, in 1988, Sampaio defined the latter as medial or lateral based more likely on sagittal plane. 36 So, a more lateral position was observed for the anterior and posterior calyces in 27.8% and 19.3% of endocasts, respectively, whereas in 52.9% of them, the anterior and posterior calyces had varied positions, superimposed or alternately distributed. 9,36
Being more focused on posterior calyces oriented >30° back to the patient’s frontal plane, Qi et al. 19 have addressed the anatomical and morphological typing of the classical branched pelvicalyceal system type (discussed earlier). So, this type can be further classified into three different types: a, b, and c, with a total of seven subtypes based on the location and number of such calyces. The “a type” consists of three subtypes, where the posterior group of renal minor calyces only associates with the upper group of renal major calyces for type a1, the middle group of renal major calyces for type a2, and the lower group of renal major calyces for type a3. The “b type” type is also classified into three subtypes, wherein the posterior group of renal minor calyces is associated with both the upper and middle group of renal major calyces for type b1, with both the middle and lower group of renal major calyces in type b2, and with both the upper and lower group of renal major calyces in type b3. The type C posterior group of renal minor calyces is associated with an upper, middle, and lower group of renal major calyces without any subtypes. According to the analysis, the more and less common types were b3 (59.16%) and b1 (2.12%), respectively. From the surgical point of view, Pradeepa et al. 37 verified the anatomical veracity of the belief that in order to enter the posterior calix, one must aim for the medial calix during a percutaneous nephrolithotomy (PCNL). Of the 508 calyces studied in 90 patients with maximum intensity projection (MIP), the posterior calix was projecting laterally in 72% and medially in 28%.
The perpendicular orientation of minor calyces draining into the surface of the collecting system during intraoperative fluoroscopy is a crucial feature for endourology. Sampaio stated that such orientation is presented in 11% of cases, 36 whereas a rate less than 10% was also mentioned and was more likely for A1 and B1 types. 24
Focus on specific calyceal group
In many works, one can find various ways of classifying individual groups of calyces according to their level, which were partially mentioned earlier, but for the sake of systematization of data and ease of reading, they should be described in isolation. Generally accepted opinion divides the small calyces into three groups: upper pole, mid zone, and lower pole, based on their location and the drained segments of the kidneys.
Upper pole
In addition to the previous section, the isolated discussion of the upper group of calyces is not as extensive and conceptually focuses on their orientation and the presence of compound calyces. It was found by Miller et al. 38 that the main plane of the upper pole calyceal group was medio-lateral (ML) in 95% of kidneys and a mix of AP and ML in 5%. Weltings et al. 31 investigated this aspect on axial computed tomography (CT) with overlapping hours of a clock and found that calyces were predominantly oriented lateral (8–10 o’clock: 44.5%) and medial (2–4 o’clock: 30.5%), which corresponds to determining orientation relative to the patient’s frontal plane rather than the kidney. 35 A similar study was carried out by von Zanten et al. 39 who compared the orientation of the upper calyces affected by urolithiasis. In the first case, transversal calyceal orientation in hours clock was much smaller (7.69 hours vs 8.52 hours), which means that calyces were more dorsally located in kidneys that were forming stones. In the previously mentioned work by Pradeepa et al., 37 the posterior calix on the MIP was projecting laterally in a majority of cases, 94% on the right and 89% on the left. Returning to earlier studies, we can find that Fine and Keen mention the orientation of the lowest calyces of the upper group—backward to papillae on the posterior wall of the sinus. 12
Speaking of compound calyces, in every case observed by Sykes, the superior calix was single, directed superiorly, and was always larger than the average calix. 11 Similar to what Lofgren stated, compound calyces are most often present in the upper group, and 57.4% consist of two fornices. 10 Other authors also concluded that the fewest numbers of calyces are presented in the upper pole, which is often monocaliceal and drained by a single midline infundibulum. 31,36
Mid zone
By analogy with the upper group, the detailed description of the mid zone is not so extensive. However, it is characterized by significant differences from the upper group. This can be partially explained by the fact that it depends not only on the time of onset of branching of the ureteral bud but also on the spatial orientation of the dorsal and ventral halves of the future kidney. For this reason, the calicyes in this location are mostly paired and have variable orientation. 20 However, in most studies, the orientation of the mid-zone calyces is defined as anterior and posterior. 11,36 However, as per Miller et al., 38 the middle calyceal group had a primary plane of AP in 100% of kidneys. Weltings et al. 31 defined that the orientation of the calyces in the mid-segment was mostly lateral at 8, 9, and 10 o’clock (26.6%, 26.6%, and 34.4%, respectively). Pradeepa et al. 37 concluded that calyces seem posteriorly oriented on MIP on the right as medial and lateral with equal probability, whereas on the left, such calyces were oriented medially in 65% of cases. In addition, such fusion of the dorsal and ventral halves of the future kidney caused not only variability of orientation in one plane but also in space as a whole, which explains the A2 type according to Sampaio and Mandarim-De-Lacerda 14 and the presence of the empty space between divided parts, where lower calyces in 87.7% were in a ventral (or anterior) position. 36
For the same reason, during the process of kidney formation, the remaining part of the parenchyma between the calyces of the mid zone prevents their approach and the formation of compound calyces, which explains the lower frequency of occurrence of the latter compared with other zones. 11,31
Lower pole
None of the pelvicalyceal system compartments is as heated a subject of debate as its lower pole. Indeed, if we group together all the studies describing both anatomical and surgical approaches in the classification of this field, both nuances regarding quantity and orientation, as well as different angular measurements, are mentioned in predicting the results of endourological interventions.
According to some data, the lower group is the most branched and can contain four or more small calyces, and there is a dependence on the type of pelvicalyceal system. As was shown by Marroig et al., such a branched structure was presented in 45.67%, 21.43%, 26.19%, and 10.71% among A1, A2, B1, and B2 types, according to Sampaio and Mandarim-De-Lacerda, respectively. 24 Also, this localization is characterized by the presence of compound calyces, but less often compared with the upper group, whereas the presence of compound calyces often correlates with drainage of the lower pole by a single infundibulum located in the middle line, 11,31,40 although there is also contradictory data. 36
Regarding the orientation of the minor calyces in the lower group, Miller et al., analyzing the primary plane wound, found that it was AP in 95% of kidneys, ML in 3%, and a combination of AP and ML in 2%. At the same time, analyzing specific calyces by their level, the most inferior was oriented anteriorly in 75% of cases, with the upper calix from this group oriented posteriorly in 60% of cases. Fine and Keen stated that the upper minor calyces of the lower group faced forward. 12,38 In contrast to the opinion about AP orientation, it was stated by Weltings et al. that orientation was predominantly lateral at 8, 9, and 10 o’clock (67.8%) and anterior at 11, 12, and 1 o’clock (25.1%). 31 Pradeepa et al. found that in the right lower calix, the identified on the MIP posterior calix was pointing laterally in 86%, whereas on the left, it was 64%. 37 Marroig et al. 24 found that lateral orientation is more frequently observed for A1, B1, and B2 types; anterior calyces for A2 types only when compared with B2; and posterior calyces for the whole A group.
There are other approaches to the classification of the lower pole from the prediction of surgical outcomes point of view, which can be divided into qualitative and quantitative. Thus, at the end of the 20th century, in two studies, the calyces were characterized as favorable (simple transition from minor to major calix and then directly into the renal pelvis) and nonfavorable when predicting extracorporeal shock wave lithotripsy (ESWL) results. However, only in the first study did this characteristic serve as a significant predictor. 41,42 In turn, the literature describes many approaches to measuring the lower group of calyces. Tuckey et al. 43 stated that caliceal pelvic height, defined as the distance between a horizontal line from the lowermost point of the calix containing the stone, in conjunction with other anatomical factors, may more accurately predict the outcome of shock wave lithotripsy. The same was shown for retrograde intrarenal surgery (RIRS) by Resorlu et al. 44 However, the basis of this set is an angle-based approach (Table 4). So, Arpali et al. 45 found the infundibulotransverse angle, which significantly predicted stone clearance after ESWL. Infundibulovertebral angle was also described, which was not effective. 46 In some studies, one can see the lower infundibulum and the inferior minor calix angle, which were significantly smaller in group B than in group A by Sampaio and Mandarim-De-Lacerda. 14,24
Variations for Angle-Based Lower Pole Measurements
There are several approaches to determining the angle between the lower infundibulum/containing stone calix and various lines passing through the UPJ/pelvis, such as those proposed by Elbahnasy, 47 Bagley, 48 Gupta, 49 two methods by Sampaio, 50,51 and one recently proposed by Tung et al. 52 Manikandan et al. 53 compared IPA between affected and healthy kidneys and found that only the Elbahnasy approach found a significant difference. Moreover, interesting results are presented in the description of the modified Takazawa classification, where angle among divided-pelvic types was larger than for nondivided ones, which is also typical for another classification. 18,24 It is logical that when an independent mid zone is formed in the process of forming the pelvicalyceal system, the lower pole moves lower and causes a decrease in the angle.
Discussion
Currently, endourological interventions have almost completely replaced open surgery in the treatment of diseases of the upper urinary tract. This has undoubtedly been facilitated by improved imaging techniques, instruments, and experience within the urological community. 54,55 However, at the same time, the need for a detailed study of the anatomy and sufficiency of spatial orientation skills within the pelvicalyceal system also increases in connection with interventions without direct vision of the surgical field and the transfer of images mainly to a two-dimensional (2D) monitor. 56,57 The anatomy of any organ is a nonmodifiable aspect, unlike other potential risk factors for failure during the surgery, such as body mass index. In this regard, it becomes clear that specialists have been intensely interested in systematizing various variants of pelvicalyceal system and in attempting various measurements within the latter for more than a century. Moreover, the first mention of the anatomy and presumed function of the kidney and pelvicalyceal system was made in the early years of science by Avicenna. 58
There are enough data in the literature to confirm or refute the importance of anatomy as a predictive factor after endourological intervention. So, for the Sampaio and Mandarim-De-Lacerda nomenclature, 14 it was stated that the collecting system with the kidney mid zone drained by crossed calyces (type A2) presented a lower accessibility rate to the small calyces during flexible ureteronephroscopy. 59 Similar conclusions were concluded by Kirecci et al. 60 who found that after RIRS, SFR was significantly lower in subgroup A2 (30.4%) and significantly higher in subgroup B2, whereas the A2 type is also characterized by increased operative duration and fluoroscopy time. Interestingly, an opposed opinion was declared for PCNL: type B1 pelvicalyceal systems necessitate an increased number of access points for achieving stone clearance 61 or there is no influence of pelvicalyceal system type at all. 62 Kawase et al. 63 investigated the impact of the pelvicalyceal system anatomical system according to the simple Takazawa classification 17 on the surgical outcomes of endoscopic combined intrarenal surgery (ECIRS) for renal and/or proximal ureteral stones with a diameter >15 mm. According to multivariate analysis, Type II pelvicalyceal system was an independent predictor of residual stones after ECIRS. Interestingly, Type 2 was statistically more often on the left and was a risk factor for stone formation at the top and upper levels. As was discussed by the authors themselves, “the infundibulopelvic width and length of the upper calix in the Type II pelvicalyceal system seem narrower and longer than those in the Type I pelvicalyceal system because the Type II pelvicalyceal system has a bifurcation point between the upper and middle calyces. This morphological feature might cause abnormal urodynamics and result in upper pole stone formation.” The reason for similar patterns between different classifications on the one hand and contradictory results in their prognostic application and the finding of unclassified types of pelvicalyceal system on the other is the very delicate process of formation of the kidney cavity during embryogenesis. The factor that has the greatest significance for the development of a certain pyelic type is whether the primary bifurcation of the ureteral bud occurs early or later, whether it will lie far, close, or within the renal sinus. This determines primarily the main divisions, length of separated parts, and angle between them, and thereby the occurrence of entirely different cavity types. 20 This omission is a drawback of all existing classifications because the authors try to fit within several types, an anatomical structure that is variable not only between individuals 30 but also between residents of different cities in the same country, 15 between genders, 25 and side. 19,36 However, there is also a positive side: the main attempts at classification are aimed specifically at the most variable part: the type of branching of the pelvicalyceal system (Table 1) and the time of branching (Table 2), whereas the morphometric parameters of the funnels and the number of calyces are apparently limited in variability because of the limitation of the process of their formation by the parenchyma of the future kidney itself. 31,39 At the same time, the variability in the branching of the upper urinary tract extends almost throughout its entire length. 64 This also explains the difference in some parameters between individual compartments within the same pelvicalyceal system. Thus, it was shown that the mean upper IL was longer than the middle and lower IL, and infundibular width was most often greater in the lower infundibulum, whereas there was no correlation between the different measurements. 31
The number of samples in studies and the method of pelvicalyceal system observation are the next problems with existing classifications. As shown in Table 1, only a few studies have studied 500 or more kidneys, with the maximum number used in work to identify patterns with an emphasis on posteriorly oriented kidneys without covering all variants, 19 which, given the world population and the high variability of the pelvicalyceal system structure, is a small number. In addition, most studies are based on endocast analysis. 19 This approach, although providing detailed casts, is very limited for many medical centers. The solution to this is to determine the anatomy using urography and CT imaging. Indeed, the use of instrumental diagnostic methods allows both retro- and prospective collection of more data for analysis. 17 –19 However, there are contradictions here too. Some argue that there is no difference between urography and CT in terms of analyzing the anatomy of pelvicalyceal system. 65,66 Some, on the contrary, emphasize the superiority of CT scans. 67 Indeed, there are several obvious disadvantages to intravenous urography (IVU). The most significant of them is observation in one 2D plane without the possibility of studying the anatomy of the pelvicalyceal system in other orthogonal planes or even three-dimensionally. This makes it difficult not only to determine the true inclination of the kidney and, accordingly, its cavities, but also does not allow reliably studying the orientation of separately taken small calyces, in particular perpendicular ones. 24,27,36 For studies on the types of structure of the pelvicalyceal system, this is not critical, as only one study indicates the use of roentgenography to determine the anatomy of the renal cavity. 27 However, this is important to remember in connection with another approach to its classification: surgical, as many studies perform morphometric measurements specifically based on IVU.
Notwithstanding the above, both IVU and CT are static imaging modalities, whereas the true anatomy of the pelvicalyceal system is a dynamic structure and depends on the patient’s position, the position of the kidney in the retroperitoneum, and the degree of filling. 30,38,68 –70 This, along with the quality of the images themselves, 38,71 also skews the reliability of both endocast-based and CT-based classifications described in the literature using precise morphometric cut-off values in determining a specific type. This contributes to the variation of various measurements as they may be different intraoperatively from those on preoperative films. Moreover, there is evidence in the literature regarding the usefulness of measuring the volume and area of pelvicalyceal system for assessing the risk of stone formation and predicting endourological interventions. 62,72,73 In general, the authors agree that an increase or decrease in these indicators is a risk factor for urolithiasis and is more favorable during surgery, respectively. However, they are based on IVP with the determination of the volume of the entire cavity using a special formula: 74 formula defined as 0.6×(area), 1 27 which, in light of the above, is burdened by several biases and deviations.
Although the proposed classifications note the main elements of variability, there is no single classification that combines branching time and type at the same time. A correlation of classifications to clinical outcomes are increasingly being reported. Thus, there is evidence that length was an independent risk factor after RIRS, 75 whereas a recent meta-analysis showed that only IPA seems to be the most important predictor. 76 This is confirmed in another meta-analysis, where an IPA of <30° indicates that no patient was stone-free, whereas at > 50°, all patients were stone-free after ureteroscopy. However, as stated by the authors themselves, although with a very low certainty of evidence, most studies were performed after the Elbahnasy approach. 77 There is no general consensus on which IPA measurement should be used. 78 Even if we accept one method as the correct one, another problem awaits us: the lack of automation in measurement and the high influence of intra- and inter-variability. This was highlighted back in 2003 by Knoll et al. 79 Considering that one of the classifications uses similar measurements, this is an incident not only in understanding the anatomy of pelvicalyceal system but also in using the latter as a predictor of the success of endourological interventions.
Even more confusing are the differences in approaches to classifying small calyces (Figs. 1 and 2). The determination of the orientation both of the entire calyceal groups 38 and separated small calyces has been described. In the latter case, the frontal plane of the kidney or patient can be used, in which the calyces have an anterior or posterior direction; 9,17,19,33 –35 or we can use the sagittal plane and define calyces as medial or lateral. Moreover, perpendicular orientation has also been described. 24,36 In this case, where is the clear line between perpendicular, anterior/posterior, and lateral/medial orientations? Perhaps the answer can be found by using clock mapping. 31,39 Finally, we may have missed the importance of studying the necks of the minor calyces, which determine their angle, and instead of accurately measuring orientation, maybe we need to return to this approach. 29

Existing approaches to classify whole minor calyces as well as the separated group.
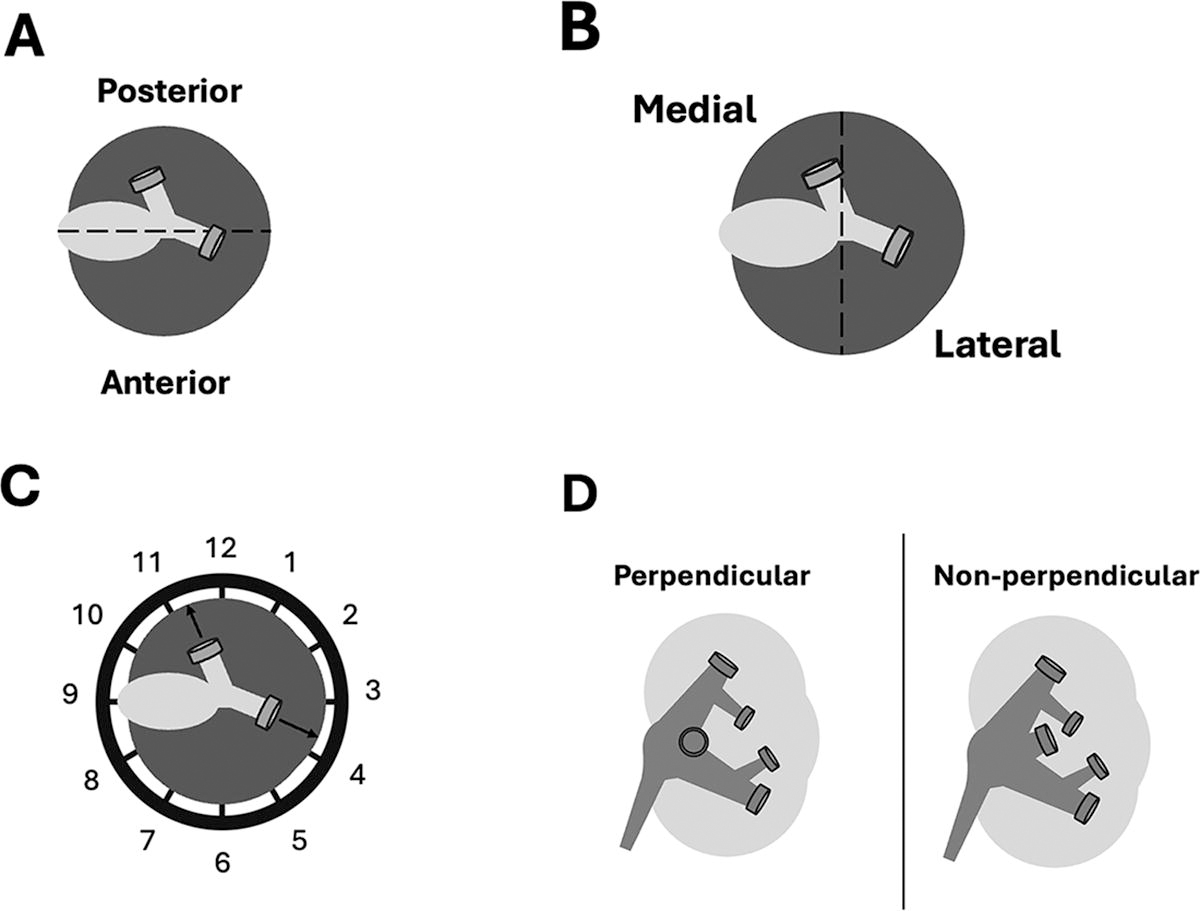
Existing approaches to define orientation of defined minor calyx.
Summarizing the above limitations, it is worth reflecting on one example that clearly shows our lack of understanding of how to classify pelvicalyceal system patients with a single stone in the lower group of calyces measuring 12 mm. The anatomy of the kidney cavity corresponds to the B2 type according to Sampaio and Mandarim-De-Lacerda, which is a favorable factor for performing RIRS. 59,60 However, this type is characterized by a larger cavity volume compared with the A group because of the absence of the inter-pyelocaliceal space 14 and by a lower IPA. 24 The latter seems to be the most important predictor of RIRS success. 76 Therefore, the question remains regarding whether we need to have a better understanding of combining the various classifications of pelvicalyceal system with clinical data.
The limitations of our study are related to a nonsystematic review of literature with some studies dating back over 100 years. Similarly, more work needs to be done in correlating the basic science work in conjunction with clinical work. Perhaps, there will be an increasing role of AI in helping this in the future. 80
Conclusion
Despite the numerous approaches to identify pelvicalyceal system from both morphological and surgical perspectives, there are significant gaps in our understanding of the real anatomy of the renal cavity that, even after more than a century, remain unanswered. There needs to be more correlation of anatomy with modern minimally invasive clinical interventions for stone disease.
Footnotes
Authors’ Contributions
A.T.: Formal analysis and writing—original draft preparation. P.J.J.: Review and editing. B.M.Z.H.: Review and editing. A.P.: Review and editing. L.T.: Review and editing. B.K.S.: Conceptualization, methodology, and review and editing.
Ethics and Consent
The research protocols performed in this study complied with the ethical principles of the Declaration of Helsinki. As this is a review article, no ethical or consent issues were there.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.