
Abstract
Purpose:
Many men undergo operation for benign prostatic hyperplasia (BPH) with lower urinary tract symptoms (LUTS). Although most procedures relieve symptoms, some patients experience recurrence or persistence. This study explores rates of and factors contributing to medical and surgical retreatment after index BPH procedure.
Methods:
This longitudinal, retrospective, population-based cohort study used MarketScan commercial insurance claims data. From 2009, men with BPH/LUTS diagnosis were evaluated for medical and surgical retreatment after index operation. Index procedures included holmium laser enucleation of the prostate (HoLEP), laser ablation of the prostate, and transurethral resection of the prostate grouped as traditional procedures, whereas transurethral microwave thermotherapy (TUMT), transurethral needle ablation, water vapor thermal therapy, and prostatic urethral lift (PUL) were minimally invasive surgical therapies (MISTs). Multivariable Cox hazard models (p < 0.05) were used to determine factors associated with retreatment after index procedure.
Results:
We evaluated 10,938 men with median age at diagnosis of 58 years (minimum–maximum 35–65). Five-year surgical retreatment rates were highest for TUMT and PUL (24.5% and 22.3%) and lowest for HoLEP (7%; p < 0.001). One-year medical retreatment rates with bladder outlet medications (i.e., alpha-blockers, 5-alpha reductase inhibitors) were higher after MIST compared with traditional procedures (42.9% vs 27.3%; p < 0.001).
Conclusion:
Surgical and medical retreatment rates are higher than previously reported in clinical trials. MIST procedures and older age were predictive of both medical and surgical retreatment after index operation. HoLEP had the lowest rate of retreatment compared with TUMT and PUL, which had the highest.
Introduction
Benign prostatic hyperplasia (BPH) is experienced by the majority of middle-aged men and can lead to bothersome lower urinary tract symptoms (LUTS). 1 In the United States, BPH treatment accounts for approximately $2.3–4 billion USD spent yearly. 2 Although lifestyle modifications and medications are appropriate first-line therapies, many men opt for surgical treatment when their symptoms are not adequately managed by medical therapy or if medication-related side effects become intolerable.
There are several traditional transurethral surgical treatment modalities for BPH, including electrosurgical resection (TURP), laser ablation, enucleation, and an increasing number of minimally invasive surgical techniques (MISTs), including water vapor thermal therapy (WVTT), prostatic urethral lift (PUL), transurethral microwave thermotherapy (TUMT), and transurethral needle ablation (TUNA). Each technique has strengths and limitations, with differing degrees of symptomatic improvement, invasiveness, and durability. Although most surgical procedures effectively relieve symptoms, a subset of patients experience recurrent or persistent symptoms, prompting them to seek additional treatment. Historically, the gold standard for surgical treatment of bladder outlet obstruction has been transurethral resection of the prostate (TURP), providing a 5-year retreatment rate of ∼5%. 3,4 In clinical trial literature, retreatment rates for WVTT are similar, ∼4% at 5 years, 5 and laser ablation was reportedly in this range as well, whereas other MISTs, particularly PUL, TUMT, and TUNA, have lower reported durability, with 5-year retreatment rates greater than 10%. 6,7 Furthermore, medical retreatment after bladder outlet procedures is infrequently reported on.
The existing literature on retreatment after bladder outlet procedures has primarily relied on single-center studies or meta-analyses, often lacking the breadth and diversity of a large nationwide dataset. We utilized the MarketScan database (IBM Watson Health) to assess the rates and factors contributing to medical and surgical retreatment after index BPH procedure.
Methods
Database and cohort generation
This study utilized the MarketScan Commercial Claims and Encounters database (Merative, Ann Arbor, MI, USA) to evaluate commercially insured men aged >35 years with a diagnosis of BPH or LUTS from 2009 to 2021. MarketScan, a nationwide database, captures de-identified health care claims data from employer-sponsored health plans and includes patients as much as the age of 65. The database includes demographic information, enrollment data, and inpatient, emergency, and outpatient billing claims on over 50 million Americans. 8 In addition, MarketScan includes prescription drug service claims for over 230 million patients. This de-identified claims data study was exempt from institutional review board review.
The index symptom date was defined as the first claim for BPH or LUTS using International Classification of Diseases (ICD) 9/10 codes (Supplementary Appendix). Starting in 2009, we included men with at least 6 months of continuous insurance coverage before initial diagnosis and with at least 60 months of continuous insurance coverage following diagnosis. Index surgical treatments were identified using the Current Procedural Terminology (CPT) coding system, including codes used for prior BPH database studies 6 (Supplementary Appendix). Using CPT codes, seven endoscopic BPH procedures were then organized into two groups by degree of invasiveness: Traditional (performed in an operating room with more than just local anesthesia) and MIST (Table 1).
Types of Benign Prostatic Hyperplasia Procedures and Total Counts of Index and Second Procedures
Men with diagnosis of BPH with at least 60 continuous months of insurance coverage after diagnosis.
aChi-square p value <0.0001.
bUroLift System (Teleflex Inc., Pennsylvania, USA). 9
cRezūm (Boston Scientific, Massachusetts, USA). 10
Surgical retreatment included any bladder outlet procedure performed at least 30 days after index bladder outlet procedure. Procedure claims within 30 days of the index procedure were excluded to account for immediate posoperative complications, as retreatment for recurrent LUTS would be unlikely within 30 days. Medical retreatment counted 90-day prescriptions filled at any time after the index operation, which could include continuation of preoperative medication or newly started therapy, but would exclude short-course medications for perioperative recovery. Medical treatment was classified into voiding (alpha-blockers and 5-alpha reductase inhibitors) and storage medications (beta-agonist and anticholinergics) (Supplementary Appendix).
Patient demographics and comorbidities were assessed, including age, Charlson comorbidity index (CCI) at diagnosis, health care plan, geographical region, place of service, and relation to insurance benefactors. Patients were excluded if they were <35 years old, missing demographic information, or underwent multiple procedures or had repeat operation claims on the same day.
Statistical analysis
We used bivariate parametric and nonparametric tests to evaluate the associations between treatment utilization and patient characteristics. The generalized chi-square test was used for categorical variables, and the Wilcoxon rank-sum test was used for continuous covariates. We constructed a time-to-event model to calculate the cumulative incidence of surgical or medical retreatment and fitted the multivariable Cox proportional hazards model to identify factors associated with retreatment. All tests were two-sided and p < 0.05. Analyses were conducted using SAS software (Cary, NC, USA).
Results
From 2009 to 2021, we identified 1,480,059 men with a diagnosis of BPH or LUTS. Of those, 512,580 (34.6%) received only medical treatment, whereas 76,048 (5.1%) underwent endoscopic bladder outlet procedure. Table 2 depicts demographics of patients who received any treatment for BPH (medical, surgical, or both). The median (min–max) age at diagnosis was 58 years (35–65). The majority of these patients were CCI 0 (58.5%) and were from urban areas (87.1%). We evaluated 10,938 men with a diagnosis of BPH who received index surgical treatment and with at least 60 months of continuous insurance coverage after diagnosis to ensure adequate follow-up information. Of these men, 65.2% were on medical therapy before index operation (60% outlet alone, 0.5% storage alone, 4.5% outlet + storage medications), whereas 34.8% were not taking any medication. Distribution of index bladder outlet procedures was similar for patients with and without medical therapy leading up to index operation (Table 3).
Demographic Summary of Diagnosis of Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms Receiving Any Surgical or Medical Treatment
*Median (Min–Max).
HDHP/CDHP = High Deductible/Consumer Driven Health Plan; HMO = Health Maintenance Organization; POS = Point of Service; PPO/EPO = Preferred/Exclusive Provider Organization.
Distribution of Index Bladder Outlet Procedures for Patients on Medical Therapy
*Parametric p value calculated by chi-square test.
BPH = benign prostatic hyperplasia; HOLEP = holmium laser enucleation of the prostate; PUL = prostatic urethral lift; WVTT = water vapor thermal therapy; TUMT = transurethral microwave thermotherapy; TUNA = transurethral needle ablation; TURP = transurethral resection of the prostate; MIST = minimally invasive surgical technique.
Surgical retreatment
Of the 10,938 men undergoing bladder outlet procedures, 1104 (10.1%) required surgical retreatment with a median of 733 days (interquartile range [IQR] 308.5–1395.5) after index operation. Table 1 demonstrates distribution of surgical treatment modality for index procedure and secondary surgical treatment; traditional procedures accounted for 72% of index surgeries. Figure 1 depicts surgical retreatment at 1- and 5 years for all included procedures. HoLEP had the lowest 1- and 5-year retreatment rates (1.7% and 7.0%) compared with the highest retreatment rates for TUMT (4.6% and 24.5%), WVTT (8.1% and 17.2%), and PUL (6% and 21.8%) (p < 0.001). For retreatment procedures, 78.3% were traditional procedures (Table 1).

Surgical retreatment rates of endoscopic bladder outlet procedures.
When analyzed by our two predefined groups, surgical retreatment at 1- and 5 years was higher for MISTs (5.2% and 21.6%) compared with traditional procedures (2.2% and 9.0%), p < 0.001 (Fig. 2). Table 3 demonstrates predictors of surgical retreatment at 5 years. MISTs (hazard ratio [HR]: 2.59, 95% Confidence Interval (CI): 2.27–2.96, p < 0.001) and older age (51–55 years, HR: 1.26, 95% CI: 1.04–1.53, p = 0.018; 55 or above, HR: 1.31, 95% CI: 1.09–1.59, p = 0.005) were associated with an increased risk of surgical retreatment. Medications before index operation did not increase likelihood of surgical retreatment at 5 years.
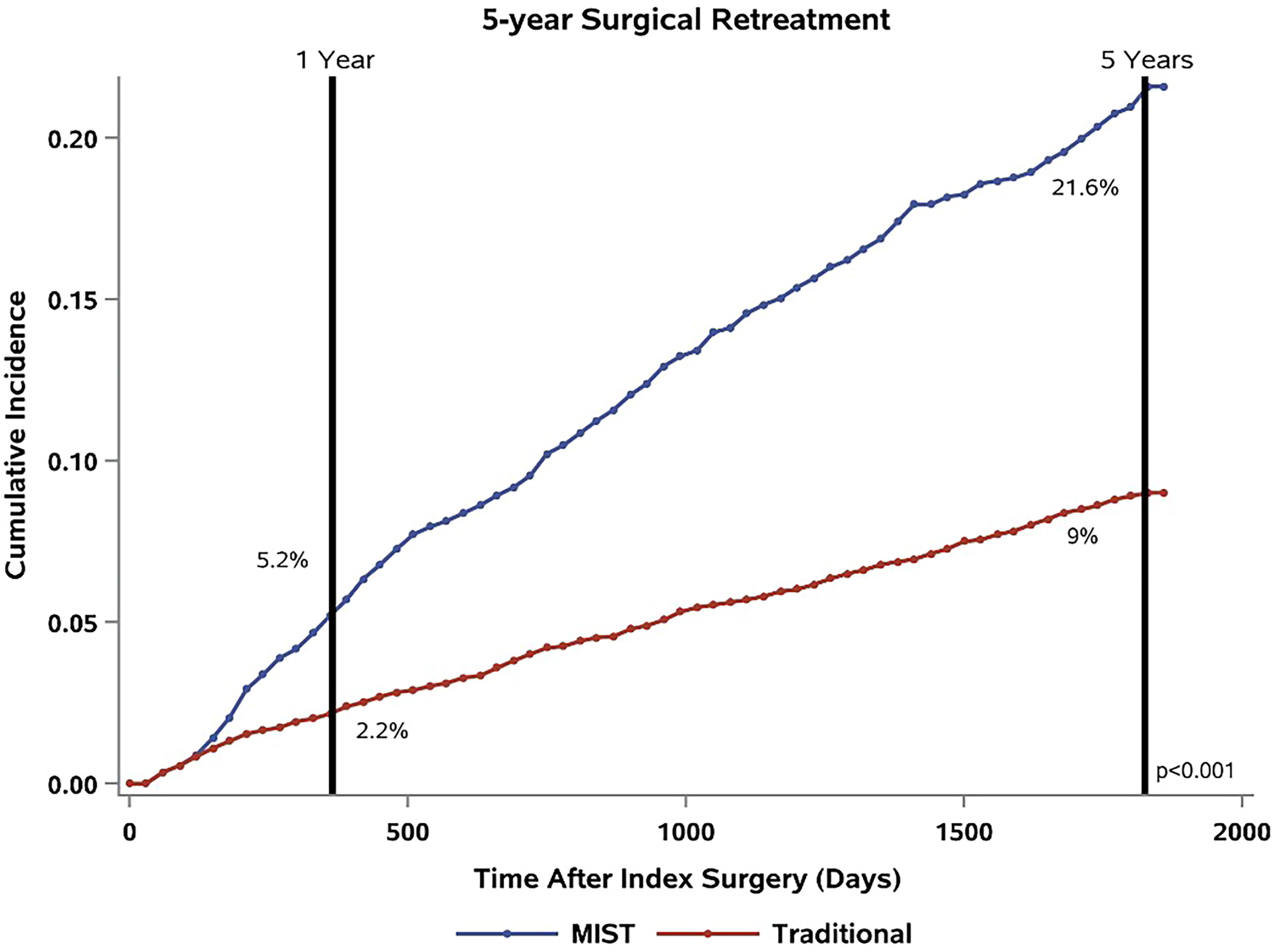
Surgical retreatment rates for MIST and traditional procedures. MIST = minimally invasive surgical technique.
Medical retreatment
Of the 10,938 men who underwent operation, 4867 (44.5%) received medical retreatment, the majority using outlet medications. The median time from index operation to filling 90-day prescription was 41 days (IQR 14–183) for an outlet medication and 127 days (IQR 46–458) for storage medications. At 1 year, HoLEP had the lowest and PUL had the highest medical retreatment rates, 21.9% and 49.2% (p < 0.001), respectively (Fig. 3). Of the HoLEP patients that required retreatment postoperatively, 16.6% received outlet medication compared with 45.9% after PUL (<0.001). When broken down by category of index operation and subclass of medication, outlet medication retreatment was 42.9% and 27.3% (p < 0.001), and incidence of storage medication retreatment was 5.7% and 6.7% (p = 0.08) for MIST and traditional procedures, respectively (Fig. 4).
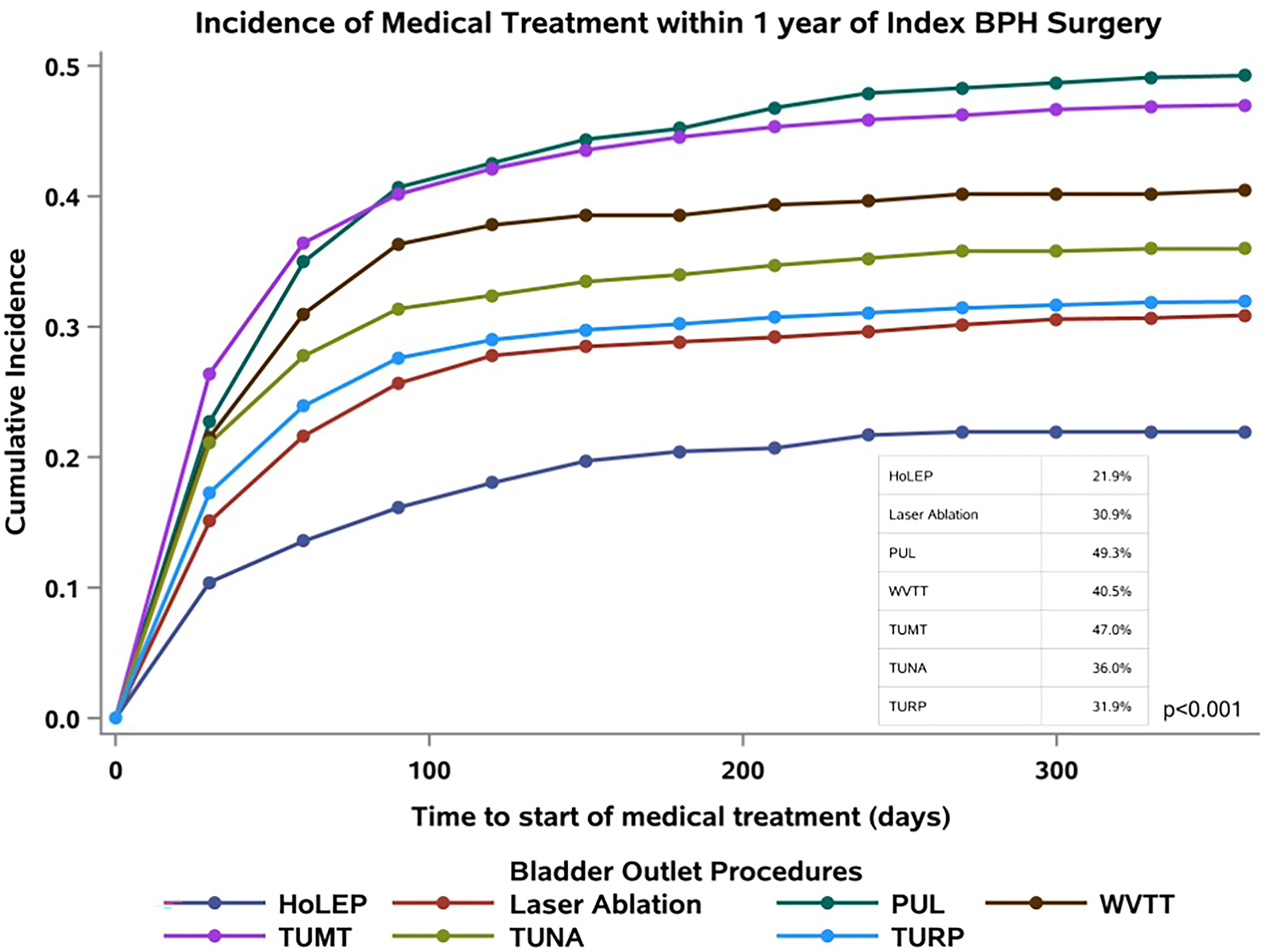
Medical retreatment after bladder outlet procedures.

Medical retreatment by prescription type after MIST and traditional procedures. MIST = minimally invasive surgical technique.
Table 4 demonstrates the factors associated with medical retreatment within 1 year of index operation. MISTs (HR 1.62; 95% CI: 1.51–1.74; p < 0.001), age ≥55 years (HR 1.11, 95% CI: 1.02–1.22, p = 0.022), and higher CCI were associated with an increased likelihood of restarting medication. Men who were not on BPH medications before index operation were less likely to receive postoperative medical retreatment (HR 0.31, 95% CI 0.29–0.34, p < 0.001).
Multivariable Model Evaluating Predictors of Medical Retreatment Within 1 Year of Index Benign Prostatic Hyperplasia Operation
p values (<0.05).
BPH = benign prostatic hyperplasia; HDHP/CDHP = High Deductible/Consumer Driven Health Plan; HMO = Health Maintenance Organization; MIST = minimally invasive surgical technique; POS = Point of Service; PPO/EPO = Preferred/Exclusive Provider Organization.
Discussion
This is the largest longitudinal study to evaluate both medical and surgical retreatment rates after bladder outlet procedures in men with BPH/LUTS. As expected, different procedures demonstrated differing retreatment rates, but this real-world claims data overall showed higher retreatment rates compared with previously published data. 3,6,11 –13 Surgical retreatment was highest for MISTs, specifically WVTT and PUL at 1 year and TUMT and PUL at 5 years, and lowest for traditional procedures, specifically HoLEP at 1 and 5 years. Overall, the rate of medical retreatment was high, with as much as 40% of patients prescribed outlet medications in the first year after operation. The ongoing medical therapy was most pronounced after MISTs, with half of PUL patients still taking medication within 1 year of index operation.
The MarketScan database provides a comprehensive assessment of U.S. health care commercial claims; thus, these data represent a real-world analysis of BPH procedure compared with initial studies that come from high-volume centers with strict inclusion criteria. 13 This commercial insurance claims database captures a younger, likely healthier population (evidenced by high percentage of CCI 0 patients) who may be more inclined to pursue surgical retreatment for recurrent symptoms compared with older or more frail patients. However, the multivariate analysis in Table 5 shows higher surgical retreatment rates for the older cohorts and that CCI had no significant impact. Furthermore, this study may underestimate surgical retreatment as some patients could pursue retreatment after transitioning to Medicare coverage, outside of this commercial database.
Multivariable Model Evaluating Predictors of Surgical Retreatment within 5 Years of Index Benign Prostatic Hyperplasia Operation
p values (<0.05).
BPH = benign prostatic hyperplasia; HDHP/CDHP = High Deductible/Consumer Driven Health Plan; HMO = Health Maintenance Organization; MIST = minimally invasive surgical technique; POS = Point of Service; PPO/EPO = Preferred/Exclusive Provider Organization.
HoLEP achieved the lowest retreatment rates, but compared with previously reported retreatment rates of 1% at 10 years, 14 our study found 7% retreatment within 5 years. This could reflect the learning curve for new providers outside of high-volume centers, where median lobe or partial gland enucleation may be performed. 15 In addition, this study is the first to report the medical retreatment rate after HoLEP as 22%, which is higher than expected, with about two-thirds continuing outlet medications postoperatively. This finding may reflect the use of HoLEP in highly dysfunctional bladders, as it has reported good catheter-free rates even in men with acontractile bladders. 16,17 Some of the medication may be tapered off with time after operation, but the utilization is still higher than expected following procedures intended to eliminate need for medication.
As an alternative to traditional endoscopic treatments, MISTs attract men who want to avoid general anesthesia, have significant comorbidities, or want to preserve ejaculatory function. The large BPH population drives treatment innovation, and new MISTs (WVTT and PUL) were developed within the time frame of this study. Starting in 2021, American Urologic Association (AUA) BPH guidelines no longer recommend TUMT and TUNA because of high retreatment rates. 18 Expectantly, the utilization of TUMT and TUNA fell off significantly around this time, but this decrease matched a rise in newer MISTs (particularly PUL) rather than in traditional procedures (unpublished data). In properly selected patients, these treatments provide good symptom improvement, but the real-world retreatment rates were notably higher than reported in the clinical trials.
MISTs are sometimes suggested as an earlier option in the treatment pathway to reduce medication burden with low morbidity, even if they may require future “touch ups.” Nevertheless, the reduction in medication was actually more pronounced for traditional procedures. In addition, traditional procedures accounted for a higher percentage of retreatment operation than index operation (78.3% vs 72.1%, p < 0.0001) suggesting that patients were less likely to elect for a “touch up” with MIST if they had recurrence of symptoms. Balancing patient preferences between relief from medications against surgical invasiveness, morbidity, and complications (outside the scope of this study) is always a challenging task and to that end MISTs are an important option in this treatment space. It should be noted that although there was a higher rate of medical retreatment after MIST, a majority of men still did not require any additional treatment.
Several studies addressing treatment cost and QoL have found that earlier surgical intervention was associated with lower cost and increased Quality of Life Years (QALY) for the patient compared with initial medical therapy followed by surgical treatment. 3,9,19 –21 The men who did not take BPH medication before index operation were less likely to take medications after, but they showed no clear preference toward MIST and had similar rates of surgical retreatment compared with men on medications preoperatively. This supports the idea that some men prefer upfront surgical intervention rather than ongoing medical therapy, but they may be more motivated by surgical efficacy for avoiding medication rather than minimizing morbidity with MISTs.
Our study has several limitations, primarily related to the nature of the large-claims database analysis. These databases lack granular patient data, most importantly prostate size and bladder health. Larger prostates typically having higher retreatment rates, 3 and AUA guidelines recommend that treatment selection considers size and shape of the prostate. 18 Real-life practice may push the limits of size recommendations. Guidelines are not rigid, and shared-decision making, particularly regarding use of MISTs on larger prostates, is within the purview of the informed consent process. This process should disclose that medical and surgical retreatment rates are likely higher for prostates outside of the recommended size criteria.
This study stratified groups by CPT code and not necessarily location of treatment. MISTs have the potential benefit of being performed as outpatient and in the clinic setting, but some cases will be done in the OR with anesthesia, further decreasing their cost effectiveness compared with traditional procedures. Furthermore, traditional procedures can be performed safely in an outpatient setting. 22 Typically, same day discharge provides increased convenience to the patient, however, should not affect >30-day retreatment rates and thus we did not include this in our analysis. Future studies may assess the evolving landscape of BPH procedure utilization as the rate of outpatient procedures increases.
Within MarketScan, the billed CPT code is reported with no capacity to validate the exact procedure. Consequently, robotic simple prostatectomy was not included as it lacked a dedicated CPT code until 2023. Given the anatomical planes, simple prostatectomy achieves comparable retreatment rates to HoLEP 3 ; however, their inherent differences make comparison difficult. Another recent addition to BPH treatment is aquablation, with reported retreatment rates comparable with traditional procedures in clinical trial. 10 Aquablation was not included in this study as it is too new to have sufficient patients with 5-year follow-up in this database. Despite a large population database, our sample size for certain procedures was relatively small (particularly WVTT, HoLEP, and TUNA). This is predominately because of our strict inclusion criteria—aiming to capture patients with 5 years of continuous insurance to determine long-term retreatment rates. But these patient numbers are still larger than those reported in the clinical trials that established retreatment rates. 5
A limitation of medical retreatment analysis was the exclusion of phosphodiesterase 5 inhibitors (PDE-5) inhibitors. This medication may be used for BPH and erectile dysfunction but were excluded because patients with symptomatic relief after surgical BPH treatment may opt to continue PDE-5 inhibitors for erectile dysfunction rather than ongoing LUTS, thus inflating retreatment rates.
Conclusion
Endoscopic procedures are an important option in the treatment of BPH/LUTS, with different procedures resulting in different rates of medical and surgical retreatment in this real-world claims database study. Traditional procedures, particularly HoLEP, have the lower rates of medical and surgical retreatment compared with MISTs. These findings can guide patient counseling, inform clinical decision-making, reform health care policies, and contribute to the ongoing optimization of BPH management strategies.
Footnotes
Authors’ Contributions
T.H. and D.P. contributed to the design and implementation of the research, D.P. contributed to the analysis of the results and statistics, and T.H. and S.M. contributed to the writing of the article. B.B. conceived the original and supervised the project.
Author Disclosure Statement
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
This study was unfunded.
Supplementary Material
Supplementary Appendix
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.