
Abstract
Background:
Exposure to environmental toxicants and climate change disproportionately affects communities of color and contributes to worse maternal and infant health outcomes. The aim of this article is to determine the effect of environmental justice (EJ) community status on preterm birth and low birthweight in Suffolk County, Massachusetts.
Methods:
A retrospective secondary data analysis was conducted linking the Massachusetts Registry of Vital Records from 2014 to 2018 to the 2010 EJ population layer. Multivariable logistic regression was performed to evaluate the associations between EJ community status, preterm birth, and low birthweight.
Results:
Living in an EJ community is associated with an increased risk of preterm birth and low birthweight compared with not living in an EJ community. However, regardless of EJ community status, non-Hispanic (NH) Black individuals had double the risk of having a preterm birth and infant born with low birthweight, and Native American/Alaska Native individuals were twice as likely to have a preterm birth in a non-EJ community compared with NH White individuals in a non-EJ community. Birthing individuals from almost all racial groups living in an EJ community had an increased risk of preterm birth.
Discussion:
Living in an EJ versus a non-EJ community is associated with worse infant health outcomes regardless of race; however, for Black and indigenous communities, the safety afforded by living in a non-EJ community does not hold.
Conclusion:
The multiple systemic factors that contribute to environmental and racial injustice need to be addressed if we want infant health outcomes to improve.
Keywords
INTRODUCTION
Preterm birth (PTB) occurs when infants are born earlier than 37 weeks of gestation. Being born too early is associated with low birthweight (less than 2500 g or 5½ pounds) which accounts for 60% to 80% of all infant deaths and contributes to potential health complications that can extend into adulthood.1,2 In 2022 10.4% of all infants in the United States (U.S.) were born preterm and in 2021, 8.5% were born with low birthweight.3,4 In Massachusetts, 9.1% of all infants in 2022 (1 in 11) were born preterm, and 7.8% (1 in 13) were born weighing less than 2500 g. 5 Notably, the rate of PTB in Massachusetts is highest for American Indian/Alaska Native (12.6%) followed by non-Hispanic (NH) Black (11%), Hispanic (9.8%), NH White (8.4%), and Asian/Pacific Islanders individuals (8.3%). 6
Many risk factors contribute to PTB including infection or inflammation, uteroplacental ischemia, stress, and other immunologically mediated processes. 7
More recently, air pollution and climate change, especially high outdoor temperatures, have been associated with PTB and low birthweight.8,9,10,11,12 However, exposure to environmental toxicants and climate change threats is not distributed equally in the population, disproportionately affecting communities of color and contributing to worse maternal and infant birth outcomes. 13
Environmental justice (EJ) is a fundamental civil rights issue and is based on the principle that all people have a right to be protected from environmental hazards and to live in and enjoy a clean and healthful environment.14,15 In Massachusetts, a neighborhood is defined as an EJ population if any of the following are true: the annual median household income is not more than 65% of the statewide annual median household income; minorities comprise 40% or more of the population; 25% or more of households lack English language proficiency; or minorities comprise 25% or more of the population and the annual median household income of the municipality in which the neighborhood is located does not exceed 150% of the statewide annual median household income. 16
In March 2021, Massachusetts Senate Bill 9—An Act Creating a Next Generation Roadmap for Massachusetts Climate Policy became law. 17 One of the many features of this law is that it increases protections for environmental justice communities across Massachusetts through the creation of the Environmental Justice Council which is appointed by the Governor and chaired by the Executive Office of Energy and Environmental Affairs. 18 The primary role of this council is to advise and provide recommendations on policies and standards that achieve environmental justice. For example, state agencies will be required to consider the cumulative impact of pollution that already exists in a community before issuing a permit for a new project. Additionally, the new law provides enforceable tools to protect the life and health of environmental communities. 19 In order to inform policy based on science, the purpose of this study is to determine the effect of living in an EJ population in Suffolk County (Boston, Chelsea, Revere, and Winthrop) and its impact on infant outcomes, specifically PTB and low birthweight.
MATERIALS AND METHODS
To assess birth outcomes within Suffolk County, Massachusetts’ Registry of Vital Records dated 2014 to 2018 were obtained as primary source data with approval for the study from both the University of Massachusetts Boston Institutional Review Board and the Massachusetts Department of Health. Additionally, data from the Massachusetts Executive Office of Energy and Environmental Affairs known as the 2010 EJ Populations layer were obtained to link our birth outcomes to the EJ community definition made by Massachusetts described above. For each assessed birth outcome, its corresponding U.S. Census Block (CB) with respective EJ determination was matched prior to statistical analyses.
In the data preparation process, 642 birth records were found to contain either a faulty or no geographic 2010 U.S. CB comprising 1.4% of the total 46,316 birth records for Suffolk County. These records were excluded from the analyses, leaving 45,674 records for valid analyses. Within the Massachusetts EJ Populations layer, 646 Suffolk County U.S. Census Block Groups (CBG) are designated as either positive YES (460) or negative NO (186) EJ geographies. Utilizing QGIS 3.28 Firenze geographic software, the 646 aggregated EJ CBG features were merged with disaggregated 2010 CB feature counterparts, resulting in 8841 unique CB analysis features within Suffolk County. Through a data linking and join script created and executed within R version 4.2.3 software, an EJ designation for each of the 45,674 records was determined. In Figure 1, the study area location is shown featuring the spatial extent of both positive and negative EJ designations within Suffolk County.

Study project area with EJ designations, Suffolk County, Massachusetts. EJ, environmental justice.
With the appropriate geographic identifiers merged to birth outcomes, infant weight and length of gestation were first analyzed with respect to EJ community designation. This designation served as the primary predictor variable. In addition, a series of maternal sociodemographic characteristics were examined. These characteristics included maternal race, education, age, and marital status. Maternal race/ethnicity was classified as NH Black, NH White, Hispanic, Asian or American Indian/Alaska Native/other NH. Maternal education status was classified as follows: less than high school, completed high school, attended college, or completed 4-year college or higher. Maternal age was grouped as follows: less than 20 years, 20–24 years, 25–29 years, 30–34 years, 35–40 years, or 41+ years. Marital status was classified as either married or not married (i.e., divorced, never married, and widowed).
In addition, maternal smoking and alcohol use were measured as (Y/N) during the 3 months before pregnancy or during pregnancy. Finally, other health factors accessed included pregnancy resulting from infertility treatment (yes/no), positive toxicology screening (yes/no), previous PTB (yes/no), and the presence or absence of four maternal medical conditions: prediabetes, gestational diabetes, prehypertension, and gestational hypertension. Of note, we had very little missing data for any of our study variables, and observations with missing data were not included in our regression analysis.
We assessed the associations between EJ community status and sociodemographic and health characteristics using chi-square tests. To evaluate the association between EJ community status and adverse infant outcomes, we used multivariable logistic regression with Stata 17 software (Stata Corporation, College Station, Texas, USA). In these analyses, we adjusted for maternal characteristics in study models 2, 3, and 4, wherein study model 1 was unadjusted; model 2 included adjustment for maternal education, age, and marital status; model 3 additionally health-related maternal characteristics; model 4 adjusted for all 12 maternal characteristics—education, age, marital status, infertility treatment, diabetes prepregnancy, gestational diabetes, prepregnancy hypertension, gestational hypertension, previous PTB, toxicology screening, maternal smoking, and maternal alcohol use. In a second series of models, we used multivariable logistic regression to assess the combined effect of maternal race/ethnicity and environmental justice status using the modeling approach described above.
RESULTS
Between 2014 and 2018, 46,316 births occurred in Suffolk County Massachusetts of which 45,674 births (98.6%) had a geographical census-identifier code and were included in this analysis. The majority of births occurred in individuals who lived in an EJ community (n = 35,703, 78%) compared with a non-EJ community (n = 9971, 22%). Most individuals had attended or graduated from college (n = 29,713, 67%) and were married (n = 28,133, 62%) (Table 1). More than a third were between ages 30 and 34 years (n = 16,396, 36%), and most were individuals of color or Hispanic. Overall, the prevalence of PTB (<37 weeks of gestation) in Suffolk County was 9.5% (n = 4311), and the prevalence of low birthweight (<2500 g) was 8.5% (n = 3864) (Table 1).
Maternal Characteristics and Birth Outcomes by Environmental Justice Community Status, Suffolk County, Massachusetts, 2014–2018
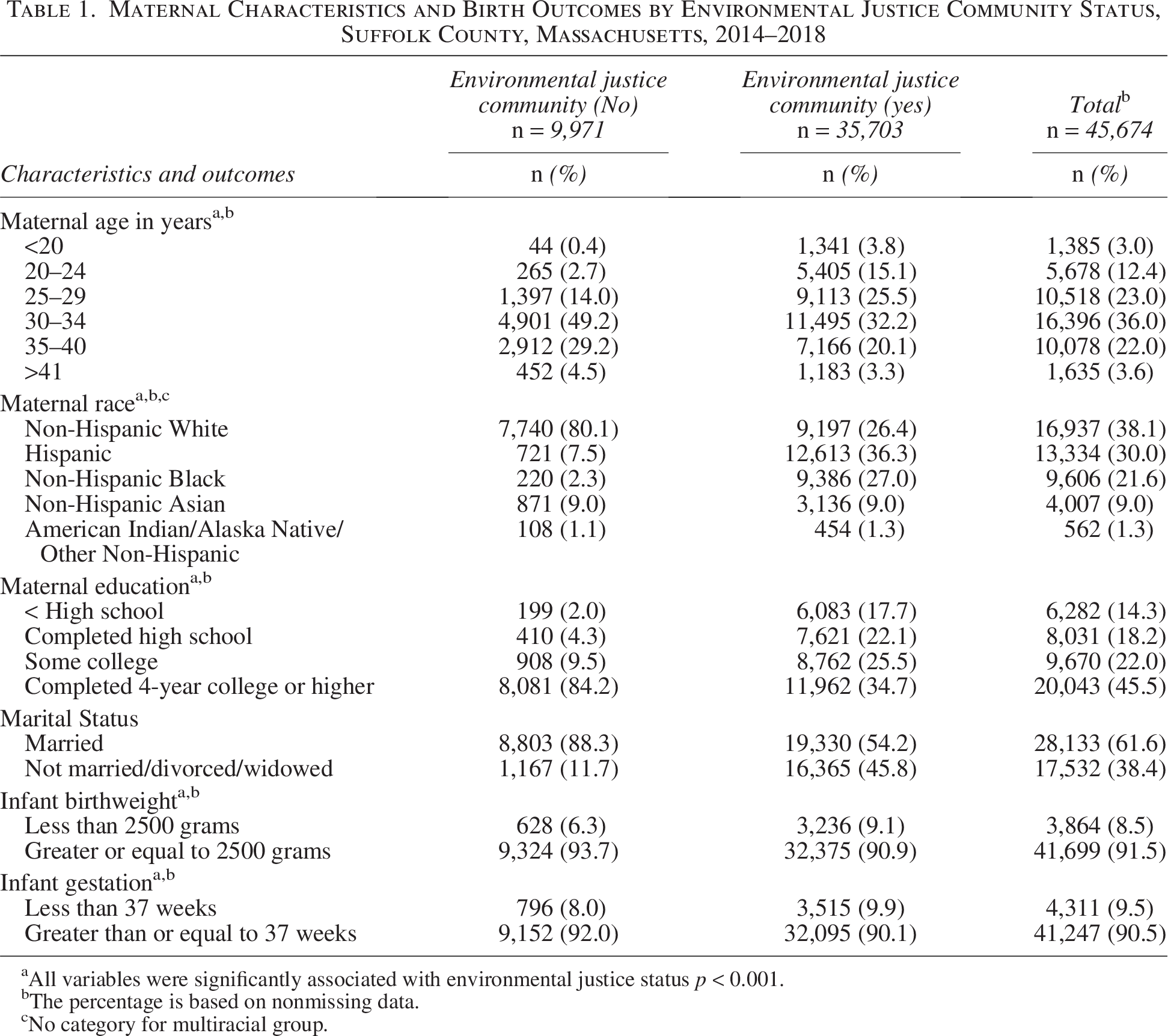
All variables were significantly associated with environmental justice status p < 0.001.
The percentage is based on nonmissing data.
No category for multiracial group.
Differences were observed in the characteristics of birthing individuals living in an EJ community compared with those not living in an EJ community. For example, birthing individuals living in a non-EJ community were significantly more likely to be NH White (n = 7740, 80%), married (n = 8803, 88%), college-educated (n = 1716, 94%), and between the ages of 30 and 34 (n = 4901, 49%) compared with women in an EJ community who were more likely to be Hispanic (n = 12,613, 36%) or NH Black (n = 9386, 27%), less likely to be married (n = 19,330, 54%), between the ages of 30 and 34 (n = 11,495, 32%), and college-educated (n = 20,724, 60%). Additionally, the non-EJ community had a lower prevalence of PTB (n = 796, 8%) and low birthweight (n = 628, 6.3%) compared with the EJ community (n = 3515, 9.9%) and (n = 3236, 9.1%), respectively (Table 1). Overall, NH Black birthing individuals had the highest prevalence of PTB (n = 1109, 11.6%) and infants born with low birthweight (n = 1150, 12%) compared with other birthing individuals (Table 2).
Birth Outcomes by Race, Ethnicity, and Environmental Justice Community Status, Suffolk County, Massachusetts, 2014–2018
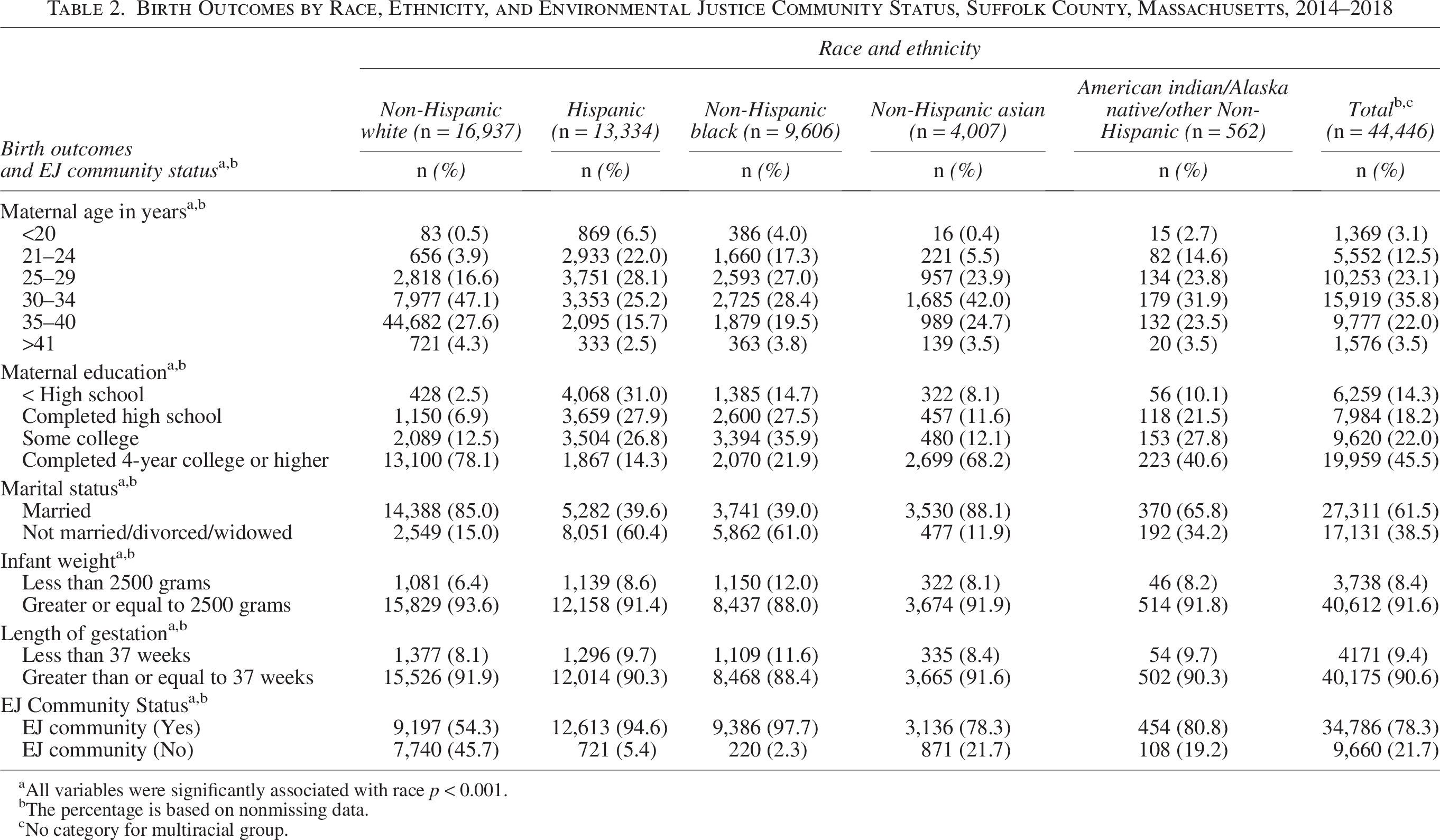
All variables were significantly associated with race p < 0.001.
The percentage is based on nonmissing data.
No category for multiracial group.
Compared with those living in a non-EJ community, those living in an EJ community had a 31% greater likelihood of infants born with low birthweight (adj. relative risk [RR] 1.31, 95% confidence interval [CI] [1.18–1.46]) and 18% greater likelihood of PTB (adj. RR 1.18, 95% CI [1.07–1.31]) adjusted for sociodemographic and health characteristics. When we examined the combined effect of race and ethnicity and environmental justice status on birth outcomes, NH Black birthing individuals and Native American/Alaska Native birthing individuals living in a non-EJ community had more than double the risk for PTB compared with their NH White counterparts in the non-EJ community (adj. RR 2.05, 95%CI [1.33–3.14] and adj. RR 2.08, 95% CI [1.09–3.96], respectively) (Table 3). Birthing individuals from nearly all race groups had an increased risk of PTB if they lived in an EJ community when compared with NH White birthing individuals in the non-EJ community (Table 4). Similarly, when compared with NH White birthing individuals in the non-EJ community, NH Black birthing individuals had at least twice the risk for infants born with low birthweight regardless of EJ community status (non-EJ adj. RR 2.23, 95% CI [1.41–3.51]; EJ adj. RR 2.02, 95% CI [1.74–2.33]) (Table 4). For Hispanic and Asian groups as well, living in an EJ community was associated with an increased risk for infants born with low birthweight compared with the NH White group living in a non-EJ community.
Prevalence and Relative Risk for Low Birth Weight and Preterm Birth Related to EJ Status, Suffolk County, Massachusetts, 2014–2018

The reference group is not living in the EJ community, with the risk of living in the EJ community compared with the risk of not living in the EJ community.
Unadjusted model.
Model 2 adjusted for maternal education, maternal age, and marital status.
Model 3 adjusted for maternal education, maternal age, marital status, infertility treatment, diabetes prepregnancy, gestational diabetes, prepregnancy hypertension, gestational hypertension, and previous preterm.
Model 4 adjusted for maternal education, maternal age, marital status, infertility treatment, diabetes prepregnancy, gestational diabetes, prepregnancy hypertension, gestational hypertension, previous preterm, toxicology screening, maternal smoking, and maternal alcohol use.
Adj. RR, adjusted relative risk; CI, confidence interval; EJ, environmental justice.
Relative Risk for Adverse Infant Outcomes with the Combined Effect of EJ Status and Race and Ethnicity, Suffolk County, Massachusetts, 2014–2018
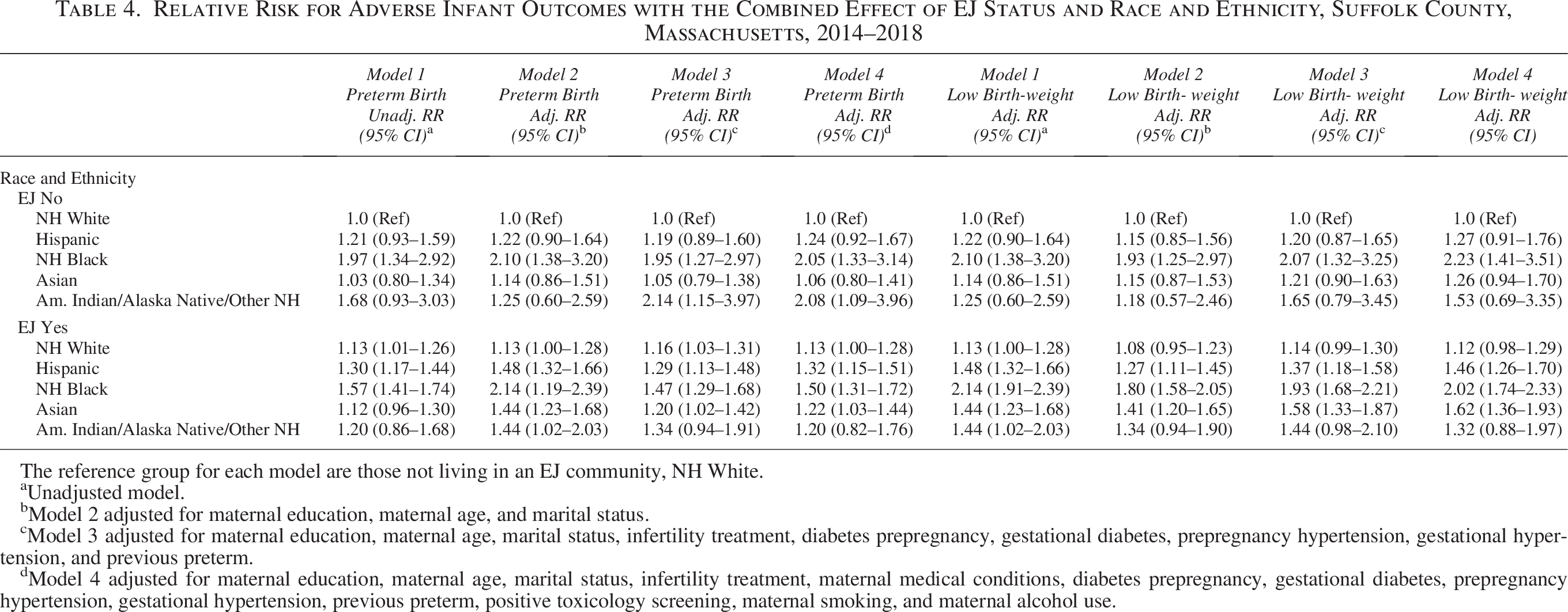
The reference group for each model are those not living in an EJ community, NH White.
Unadjusted model.
Model 2 adjusted for maternal education, maternal age, and marital status.
Model 3 adjusted for maternal education, maternal age, marital status, infertility treatment, diabetes prepregnancy, gestational diabetes, prepregnancy hypertension, gestational hypertension, and previous preterm.
Model 4 adjusted for maternal education, maternal age, marital status, infertility treatment, maternal medical conditions, diabetes prepregnancy, gestational diabetes, prepregnancy hypertension, gestational hypertension, previous preterm, positive toxicology screening, maternal smoking, and maternal alcohol use.
DISCUSSION
The main findings from our study show that living in an EJ community is associated with an increased risk for PTB and low birthweight compared with not living in an EJ community. However, regardless of EJ community status, NH Black birthing individuals had double the risk of having a PTB and infant with low birthweight compared with NH White birthing individuals living in a non-EJ community, and Native American/Alaska Native birthing individuals living in a non-EJ community were twice as likely to have a PTB compared with NH White birthing individuals in a non-EJ community. Notably, birthing individuals from almost all racial groups living in an EJ community had an increased risk of PTB, and Hispanic and Asian individuals had an increased risk of having an infant born with low birthweight if they lived in an EJ community, but not a non-EJ community.
Compared with national and state rates for PTB and low birthweight, the birthing individuals included in our study had a slightly higher rate of PTB (9.5%) compared with Massachusetts state figures (9.1%) but a lower rate compared with the national preterm rate (10.4%). Among our urban Suffolk County population, there was a slightly higher prevalence of PTB among NH Black individuals (11.6%) compared with the Massachusetts state rate for NH Black individuals (11%). The most recent national rate for low birthweight is 8.5%, and for Massachusetts it is 7.8%. 20 The prevalence of low birthweight for our study population was 8.5% with a similar percentage among Hispanic and Asian groups, yet the prevalence was highest among NH Black individuals (12%) and lowest for NH White individuals (6.4%). It is important to note that some of the observed differences might be attributable to population distributions according to environmental justice status and urban–suburban–rural residence.
Our findings are similar to other studies in that living in an environmental justice community is associated with PTB or low birth weight and disproportionately affects marginalized individuals, especially NH Black birthing individuals.21,22,23,24 Notably, environmental justice communities have higher rates of pollutants that worsen air quality, and they also have increased levels of lead in their homes and drinking water which are linked to PTB.25,26
Overall, Black, Hispanic, and Asian individuals are exposed to higher concentrations of air pollution from all major emission groups compared with NH White individuals. 27 These pollutants come from an increased proximity to highways, industrial facilities, restaurants, houses, and apartment buildings where exposed residents reside. These environmental stressors are embedded into the very structures of EJ communities.
Although the air quality in the U.S. has improved over the last 20 years, the decline in PM2.5 has not been found to be equitable in all communities, especially impacting communities of color. 28 In our study, all birthing individuals regardless of race who lived in an EJ community had a higher likelihood of PTB or low birthweight infants compared with NH White birthing individuals living in a non-EJ community which could be explained by their increased risk of exposure to environmental hazards. As such, all sectors of society need to be engaged in drafting environmental laws, regulations, and policies so that individuals living in EJ communities can have a clean and healthy environment in which to be born, live, work, play, and thrive.
Notably, NH Black birthing individuals in our study had the highest rates of PTB and low birthweight, a finding that is consistent with a report on U.S. trends in preterm infant mortality. 29 Yet, in our study, this finding persisted for NH Black birthing individuals regardless of EJ community status in that living in a non-EJ community was not a protective factor as it relates to birth outcomes. This finding could be due to the disproportionality of residence in our study as there were small numbers of NH Black individuals living in a non-EJ community (n = 220) who also had a PTB (n = 26).
Nevertheless, this finding is not entirely new in that Black individuals in the U.S. have the worst maternal and infant health outcomes regardless of economic status. 30 For example, education and marital status are often used as indicators of socioeconomic status, yet the NH Black individuals in our study had a higher percentage of completing a 4-year college education (22%) and the same level of marriage (39%) compared with Hispanic individuals (14%, 39.6%, respectively), and yet, Hispanic individuals had much lower rates of PTB and infants born with low birthweight compared with NH Black individuals in a non-EJ community. Other reasons for this health inequity could be related to the use of products that contain phthalates which are associated with PTB and low birth weight infants. Literature reviews suggest that NH Black individuals have higher levels of low molecular phthalates resulting from exposure to personal care products specifically marketed to them. 31
Nonetheless, our study cannot explain why there are higher rates of PTB and low birthweight for NH Black individuals living in a non-EJ community compared with an EJ community, or why living in a non-EJ community did not offer some protection to NH Black individuals. However, to better understand why this might be, we must examine our findings utilizing an intersectionality lens. Importantly, the births included in our study occurred in a densely populated geographic area of Massachusetts. The reality is that individuals living in a non-EJ community do not stay within the confines of that community but most likely cross into the EJ community to work, visit family and friends, and for many of them, deliver their infant in an EJ community.
Moreover, the definition of an EJ community is limiting in that it only includes income, minority status, and English proficiency and does not consider a birthing individuals’ gender, pregnancy, perceptions of support, or the perceived and actual experiences and reactions to institutionalized, interpersonal, and structural racism, all of which are known to contribute toward birth outcomes regardless of where an individual lives.32,33,34,35
Consequently, it is critical that we address environmental and racial injustice to attempt to reverse the serious health risks to Black birthing individuals and their infants, specifically as it relates to PTB and low birthweight outcomes. Suggested strategies include professional, community, and patient education on the impacts of environmental insults on birth outcomes; implementation of local, state, national, and workplace policies that advocate to protect mothers and infants; and research and targeted funding to address the challenge.
LIMITATIONS
Our study had limitations. Although birth registry data are widely used in maternal–child research, the quality of birth registry data has been questioned and is a potential limitation of our study. For example, some of the variables we controlled for such as maternal health conditions (hypertension and diabetes) or pregnancy history data may be underreported.36,37
Nevertheless, our main study outcome variables (gestational age and infant birth weight) have been shown to be highly reported.38,39 Additionally, we did not limit our sample to include only singleton births. Although multiple gestation birth is associated with PTB, a very small percentage of births in Massachusetts is multiple gestation (3.4%), and based on the low percentage, we do not believe this affected our overall findings. 40 Also, the majority of birthing individuals in our study lived in an EJ community, including NH White individuals. Conversely, very few Black and Native American/Alaska Native birthing individuals lived in non-EJ communities, which may have impacted our analysis even after we controlled for maternal demographic characteristics. Nonetheless, we were able to detect substantial and expected differences between groups based on EJ community status, race, and ethnicity.
CONCLUSION
PTB and low birthweight inequities are an opportunity for public health and other interventions to address social determinants of health. As we consider the Massachusetts definition of an EJ community and who lives in a designated EJ community, we want to emphasize that it is not the race and economic status of the people in these communities, but the structures and systems that drive the poor infant outcomes. We, therefore, recommend utilizing an intersectional antiracist lens when developing interventions to address birth inequities for Black individuals and for individuals living in an EJ community as these approaches have been shown to be generally more targeted and, hence effective.41,42,43,44,45
AUTHORS’ CONTRIBUTIONS
L.H.-F.: Conceptualization, formal analysis, resources, data curation, writing original draft, supervision, funding acquisition, and visualization. G.D.: Methodology, software, formal analysis, writing review, and visualization. S.M.: Conceptualization, software, visualization, and writing—review and editing. L.N.-J.: Visualization and writing—review and editing. C.D.: Conceptualization, visualization, and writing—review and editing. S.L.: Methodology, formal analysis, visualization, and writing—review and editing. L.S.: Methodology, software, formal analysis, writing—review and editing, and visualization.
Footnotes
AUTHOR DISCLOSURE STATEMENT
All authors declare that there are no ethical or financial conflicts of interest to report.
FUNDING INFORMATION
Sustainable Solutions Lab at the University of Massachusetts Boston for $7500 to fund study.