
Abstract
Background:
Structural racism measures based on publicly available data alone do not capture the breadth of lived experiences of racism or their impacts. Few studies incorporate measures of lived experience in analyses of structural racism at the neighborhood level. We investigated associations between self-reported experiences of racism, measures of racialized economic segregation at the census tract level (a proxy for structural racism), and birth outcomes among pregnant African American people.
Study Design:
Participants were enrolled in the Atlanta African American Maternal-Child Cohort (N = 297). Experiences of racial and gender discrimination were measured during pregnancy using self-reported, validated questionnaires. The index of concentration at the extremes (ICE) was used to quantify economic segregation (ICEincome) and racialized economic segregation (ICErace-income) for the census tract of residence during pregnancy. An analysis of continuous ICE measures and self-reported experiences of discrimination was conducted using Kruskal–Wallis rank-sum testing. Linear regression was used to estimate associations between self-reported experiences of discrimination and ICE scores with gestational age (in weeks) at delivery and birthweight for gestational age z-scores.
Results:
Participants living in areas of higher racialized economic privilege reported more frequent experiences of discrimination (χ2 ICEincome = 10.81; χ2 ICErace+income = 6.30; p < 0.05). An increase in frequency of self-reported experiences of discrimination was associated with reduced gestational age at delivery (β = −0.08, 95% confidence interval [CI] = −0.13, −0.03) but not with birthweight for gestational age in adjusted models. ICE scores were not associated with either birth outcome.
Conclusions:
In this Atlanta birth cohort, self-reported experiences of racial discrimination, but not measures of racialized economic polarization, were associated with reduced gestational age among African American pregnant people.
INTRODUCTION
In the United States, African Americans (AAs) are over three times more likely to die during pregnancy and are twice as likely to experience a preterm delivery, compared with White pregnant people.1,2 Maternal mortality increased nationwide by 29% between 2014 and 2021, and this rate is significantly higher among Black birthing people compared with other racial/ethnic groups. 3 Significant positive associations between experiencing racial discrimination, preterm birth (PTB), and small for gestational age (SGA) have been consistently identified in the literature. For example, in a study investigating high frequency of police encounters and PTB, odds of PTB were 100% higher for Black Americans living in neighborhoods with high numbers of documented police incidents. 4 These associations are particularly notable across the southern United States. In a study on associations between structural racism as measured by racial residential segregation and risk for stillbirth, Black–White disparities in stillbirth risk rose by over 40% in high-segregation counties compared with low-segregation counties. 5 Self-identified AA women navigate a uniquely complex social environment as people with doubly minoritized 6 identities, who often face compounded experiences of racial and gender discrimination. 7 Increasingly, exposure to structural racism has been identified as a risk factor for adverse birth outcomes, including PTB and SGA.8,9 While the mechanisms underlying these observed associations remain unclear, it may involve stress response through activation of the hypothalamic–pituitary–adrenal (HPA) axis. 10 In this pathway, several hormonal cascades ensue and culminate with the release of cortisol from the adrenal cortex. 11 Among self-identified Black women, cortisol production is significantly elevated following experiences of racial discrimination. 12 Elevated levels of cortisol have also been linked to PTB.13,14 Importantly, however, public health research investigating the relationship between birth outcomes and racism often focuses on population-level metrics and excludes individual perspectives.
The index of concentration at the extremes (ICE) is a commonly utilized metric for quantifying disparities in wealth and privilege, which can be readily quantified using publicly available data. 15 ICEincome reflects the extent to which the population of a given geographic area is concentrated into relative extremes of affluence (≥80th income percentile versus those in the ≤20th income percentile). 16 In a capitalist society such as the United States, higher income is associated with more access to opportunity and economic security, which confers a greater degree of privilege. 17 In addition, ICErace-income accounts for economic and racial segregation by measuring the extent to which geographic areas comprise high privilege (e.g., wealthy, White residents) versus low privilege (e.g., economically disadvantaged, Black residents, representing areas that do not benefit from economic privilege or white supremacy and its affiliated social capital). 18 ICE metrics have been utilized in several studies looking at the relationship between race, income, and maternal morbidity. 19 Overall, these studies demonstrated increased risk for adverse health outcomes in areas of lower socioeconomic status and higher degrees of racialized economic segregation.20,21,22 Although ICE metrics capture economic privilege and racialized economic segregation, population-level aspects of structural racism, they do not incorporate individual, and interpersonal manifestations of structural racism. 23 To engage a robust analysis of the effects of structural racism on health outcomes, both individual- and neighborhood-level manifestations must be captured.
In the present study, we examined associations between self-reported experiences of racial and gender discrimination, ICE metrics, and the outcomes of gestational age at delivery and birthweight for gestational age z-scores (a proxy for fetal growth) in a cohort of AA birthing people in Atlanta, Georgia. A large and growing body of literature has provided evidence for the adverse impact of systemic racism, including racial residential segregation, on birth outcomes across the United States.24,25 Racism can be conceptualized at multiple levels, including interpersonal and systemic. 26 Racialized economic segregation, as measured by ICE, is a systemic manifestation of structural racism that can be experienced at the individual level through economic disenfranchisement and residential racial segregation. We hypothesize that individuals who lived in census tracts with lower ICE metrics (indicating lower economic privilege and greater racialized economic segregation) would report a higher lifetime frequency of individual-level racism. Historic and contemporary divestment in Black communities, especially in terms of health care access, widens disparities in health outcomes and serves as a barrier to adequate access to the full spectrum of reproductive care. 27 We additionally hypothesize that increases in lifetime frequency of self-reported experiences of racism would be negatively associated with gestational age at delivery and birthweight for gestational age, while an increase in ICE metrics (where higher scores reflect more privilege) would be positively associated with birth outcomes and negatively associated with self-reported experiences of gendered racial discrimination.
METHODS
Study design and population
Participants for this analysis were a subset of 547 individuals enrolled in the Atlanta African American Maternal-Child Cohort for whom maternal address during pregnancy was successfully geocoded to the level of census tract, self-report measures of experiences of racism were available for analysis, and whose pregnancy ended in live birth (N = 297; Supplementary Fig. S1). Detailed information on recruitment and retention is provided elsewhere. 28 Briefly, participants were recruited between 2016 and 2020 from two major metropolitan hospitals in Atlanta, Georgia: Emory University Hospital Midtown and Grady Memorial Hospital. Participants were eligible for inclusion if they self-identified as African American or Black race, were U.S.-born, were pregnant with a singleton fetus between 8 and 14 weeks gestation, were 18–40 years of age, and did not have any diagnosed chronic medical conditions. This study was approved by the Emory University Institutional Review Board, and all participants provided written, informed consent prior to enrollment.
Geocoding of address during pregnancy
Participant self-reported addresses were geocoded in ArcGIS Pro (v 3.1), which includes the underlying locational databases (streets, parcels, rooftops, and administrative boundaries) that addresses match to and the algorithms and codes that attempt to select the best, most accurate latitude/longitude location for each address. To assess the reliability of addresses, a geocoding quality variable was constructed based on our ability to match addresses to a point address with values ranging from 0 to 100 (with 100 being a perfect match). Our inclusion criteria required a level of 60 or higher for geocoding quality to be included in this analysis. We assigned a census tract identifier to each participant address using the appropriate census tract boundary file. When more than one address was available for a given participant during the prenatal period, we used the first reported address during the pregnancy period; 79.46% of our study population had only one address available during the relevant time period. Census-tract level Federal Information Processing Standards (FIPS) codes were then identified. Neighborhood-level measures were obtained by linking the FIPS codes to the American Community Survey (ACS). Study participants were then matched with a neighborhood-level measure value based on the census tract they were residing in during pregnancy.
Assessment of structural racism using the ICE
For participants with geocoded maternal residential address data, we calculated ICE metrics. 29 ICE metrics were calculated using the 2014–2018 ACS 5-year tract group estimates.
ICEincome is calculated as a measure of economic privilege, capturing the extent to which disadvantaged and privileged populations are concentrated within a specific census tract. We defined economically advantaged individuals as those with an annual household income of >$100,000 and disadvantaged individuals as those with an annual household income of <$20,000, reflecting the 80th and 20th percentile of household income, respectively, for consistency with prior research in Georgia. 30
We calculated ICErace-income as a measure of racialized economic segregation, which reflects the concentration of white participants in the 80th percentile of household income, versus Black participants in the 20th percentile of household income, in a specific census tract. Income cutoffs were the same as those used to define ICEincome.
Scores on the ICEincome and ICErace-income range from −1 to +1, where scores closer to +1 reflect more privilege. ICE scores were treated as continuous measures in our primary analyses.
Assessment of self-reported experiences of racial and gender discrimination
The validated experiences of discrimination (EOD) scale was administered at 8–14 weeks gestation and was used to assesses self-reported experiences of racial discrimination in various settings across the lifetime, including in the community and workplace. 31 These experiences are contextualized within the number of situations and the frequency of occurrence over the lifetime (range 0–40).
Experiences of gendered racial stress across the lifetime were assessed at 8–14 weeks gestation using the Jackson Hogue Phillips Contextualized Stress Measure (JHP). 32 This validated questionnaire measures exposure to racial and gendered stress. Total scores on the JHP ranged from 45 to 159.
Scores on the EOD and JHP were treated as continuous measures in our primary analyses, where higher scores corresponded to higher levels of self-reported racial and gender discrimination, respectively.
Birth outcomes
Gestational age at delivery (in completed weeks) was abstracted from the medical record and was determined using the best obstetrical estimate per the American College of Obstetricians and Gynecologists guidelines. 33 Given enrollment criteria, all participants in this study had the estimated date of conception established in early pregnancy (enrollment visit between 8 and 14 weeks) by last menstrual period and/or first trimester ultrasound. Birthweight in grams was abstracted from the medical record and based on the first weight measured in the delivery room by the delivery room attendant. We calculated sex-specific birthweight for gestational age z-scores as a proxy for fetal growth at the time of delivery. 34 Birthweight for gestational age z-scores was sex-specific and estimated from the 2017 U.S. population-based natality files as a reference for singleton births. 35 PTB was defined as delivery prior to thirty-seven completed weeks of gestation. 36 Our reference group for PTB included mothers who experienced healthy, full-term pregnancies (e.g., infants born after 39 weeks) with no history of gestational hypertension, gestational diabetes, or preeclampsia. SGA was defined as birthweight z-score below −1.282 (under the 10th percentile) for sex and gestational age at birth based on a reference standard for singleton births at time of delivery in the U.S. population. 37
Covariates
Information regarding maternal age, educational attainment, and insurance status was assessed at the first prenatal clinic visit via self-reported interview questionnaire in conjunction with medical record abstraction of sociodemographic data. An income to poverty ratio was calculated using a combination of the number of members in the household and self-reported annual household income. Early pregnancy body mass index (BMI; kg/m2) was calculated via maternal height and weight as measured at the first prenatal clinic visit (between 8 and 14 weeks gestation). Information regarding parity (number of prior viable deliveries, coded as 0-integer) and infant sex (male, female assignment at birth) were obtained via medical record abstraction. Information on substance use (including use of tobacco, alcohol, and recreational drugs) was assessed by self-report using the Timeline Followback Questionnaire, 38 which ascertains substance use in the prior month, and medical record abstraction, noting patient report of substance use to their health care provider during initial or subsequent prenatal visits. These self-report questionnaire and medical record data were used to classify patients as users or non-users of substances during pregnancy.
Statistical analysis
We restricted our analytic sample to the subset of participants for whom a prenatal residential address was fully geocoded and linked to the ICE metrics and birth outcome data were available (N = 297). The distribution of demographics in our study population was described using frequencies, counts, means, and standard deviations (SDs) and used to confirm that assumptions required for linear regression outcomes were met. We additionally examined the mean and SD of ICE metrics and self-reported experiences of racial and gender discrimination across demographic characteristics. Choropleth maps of metropolitan Atlanta, Georgia, were developed to visualize tertiles of ICE scores and self-reported experiences of racial and gender discrimination across census tracts.
We used unadjusted and adjusted linear regression to examine individual associations between ICE metrics, self-reported experiences of racial and gender discrimination with gestational age at delivery, and birthweight z-scores. Covariates retained in adjusted models included maternal level of education, maternal age, health insurance, income to poverty ratio, substance use, and early pregnancy BMI. These covariates were chosen based on associations between exposures and outcomes in our study population and were guided by a directed acyclic graph (DAG; Supplementary Fig. S2). Most participants in this analysis live in census tracts with at least two other participants. To account for clustering of data across census tracts, we utilized the Huber–White cluster sandwich estimator of variance. 39 In all models that include an ICE metric as the exposure, we included the cluster sandwich estimator as a covariate in our linear models.
As a sensitivity analysis, we used logistic regression to assess associations between ICE metrics and self-reported experiences of racial and gender discrimination with the binary outcomes of PTB and SGA. We also examined term birthweight (birthweight in grams among those delivering ≥37 weeks gestation) as an outcome using linear regression models.
RESULTS
The majority of the 297 participants in our analytic sample were between 18 and 25 years of age (63%), single or not cohabitating with a partner (52.2%). High school was the highest level of educational attainment for more than one-third of participants (38.7%) (Table 1). Mean gestational age at delivery among participants was 38.23 weeks (SD = 2.77), and mean birthweight for gestational age z-scores was −0.48 (SD = 1.04). Mean levels of self-reported experiences of discrimination and gendered racial stress were higher among those who were >35 years of age and obese relative to those who were younger and had a normal BMI. Mean experiences of discrimination scores were also higher among those who had a college or graduate degree relative to high school and who had private compared with public insurance. Mean gendered racial stress scores were higher among those who reported any substance use versus none and had one or more prior births. Mean ICEincome and ICErace-income scores were lowest (closet to −1, reflecting low privilege) among those who were <25 years, underweight, who had less than a high school education, were single, had an income to poverty ratio <100%, and who delivered at Grady Memorial Hospital. We note minimal differences in the distribution of demographic characteristics between our analytic sample and the larger cohort. However, we do observe a greater percentage of participants in this analysis who utilize Medicaid. Additionally, we note that more participants in the larger cohort had an income to poverty ratio exceeding 300%, when compared with our analytic sample (Supplementary Table S1).
Demographic and Clinical Characteristics of the Atlanta African American Maternal-Child Cohort (2016–2020) and Distributions of Self-Reported Experiences of Racial and Gender Discrimination and the Index of Concentration at the Extremes Across Demographics (N = 297)
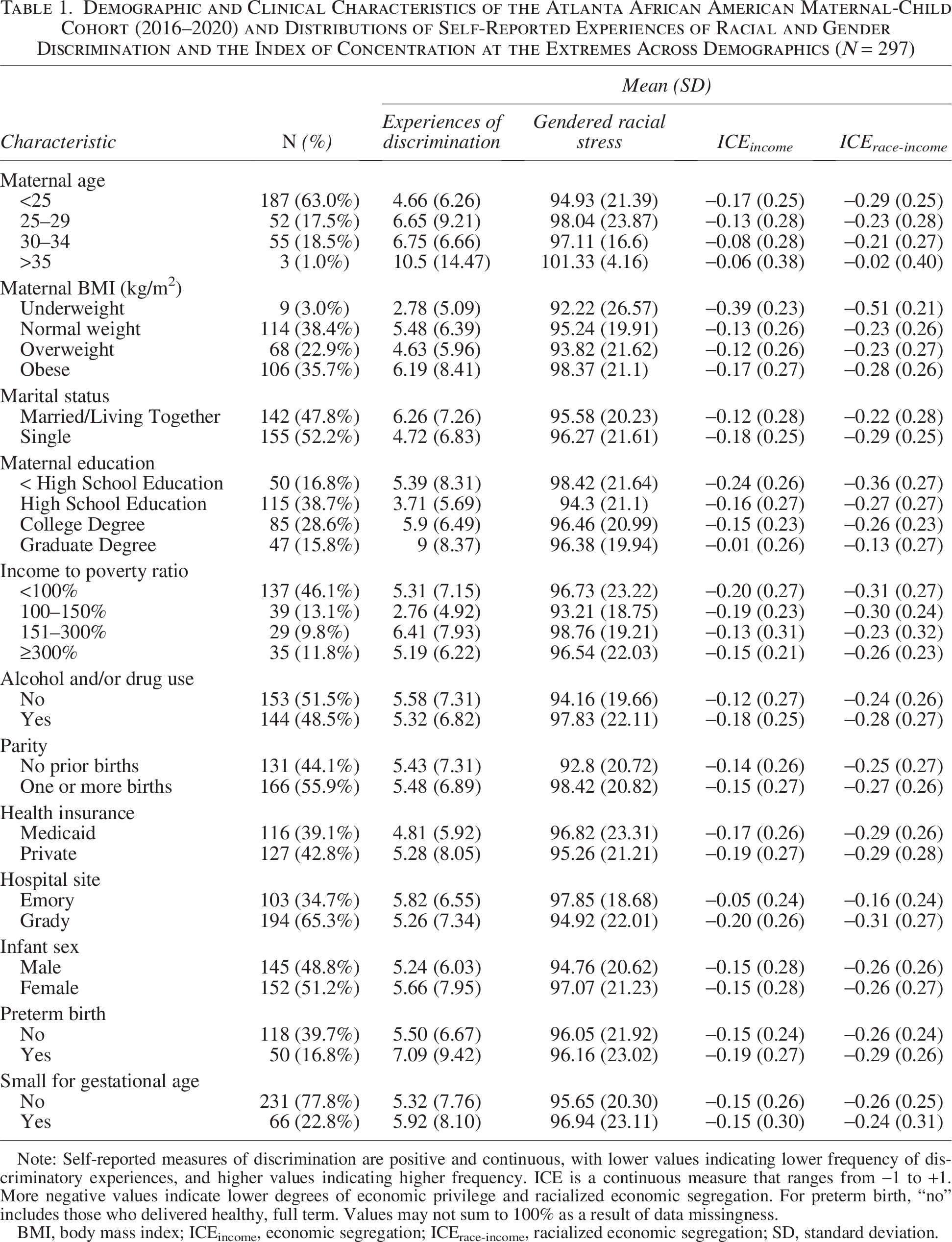
Note: Self-reported measures of discrimination are positive and continuous, with lower values indicating lower frequency of discriminatory experiences, and higher values indicating higher frequency. ICE is a continuous measure that ranges from −1 to +1. More negative values indicate lower degrees of economic privilege and racialized economic segregation. For preterm birth, “no” includes those who delivered healthy, full term. Values may not sum to 100% as a result of data missingness.
BMI, body mass index; ICEincome, economic segregation; ICErace-income, racialized economic segregation; SD, standard deviation.
We observed that the mean levels of self-reported experiences of discrimination were highest among those who lived in census tracts with the highest privilege (defined as the upper tertile of ICErace-income and ICEincome) (Table 2). In contrast, mean levels of self-reported gendered racial stress were generally consistent across tertiles of ICErace-income and ICEincome (Table 2). According to Kruskal–Wallis test results, self-reported experiences of discrimination show significant difference according to ICErace-income and ICEincome tertiles (p < 0.05, Table 2). Census tracts with more negative ICE scores (reflecting less privilege) were most concentrated toward the central metro Atlanta area (Fig. 1). In contrast, participants in nearly all tract groups throughout metropolitan Atlanta reported moderate or high frequency of self-reported experiences of racial discrimination and gendered racial stress (Fig. 1).
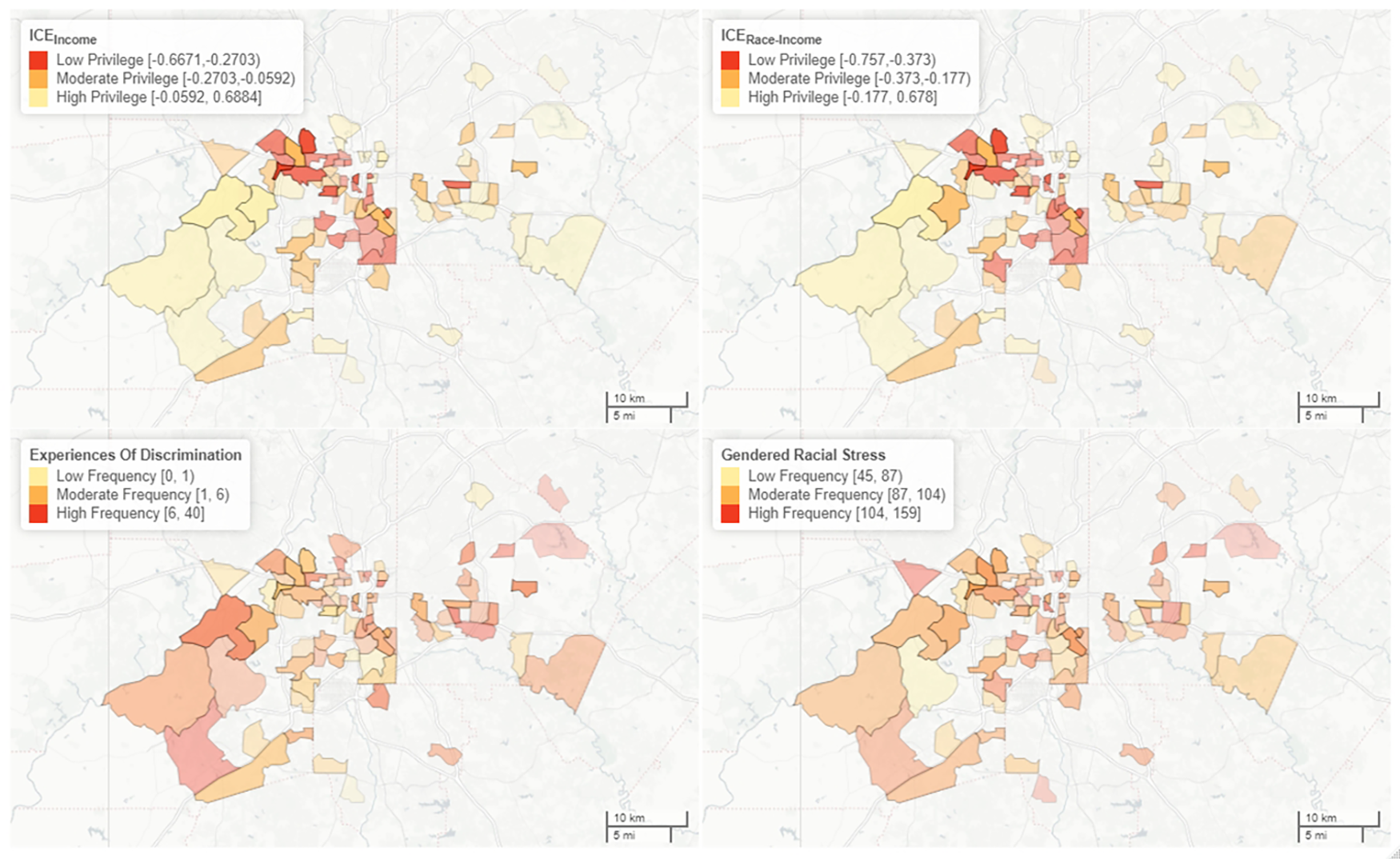
Distribution of index of concentration at the extremes (ICE) metrics and frequency of self-reported experiences of discrimination and gendered racial stress in the Atlanta African American Maternal-Child Cohort (2016–2020) (N = 254). Census tracts with less than two individuals were omitted to protect confidentiality. ICEincome, economic segregation; ICErace-income, racialized economic segregation.
Distribution of Economic Privilege (ICEincome) and Racialized Economic Segregation (ICErace-Income) by Self-Reported Experiences of Discrimination and Gendered Racial Stress in the Atlanta African American Maternal-Child Cohort (2016–2020) (N = 297)
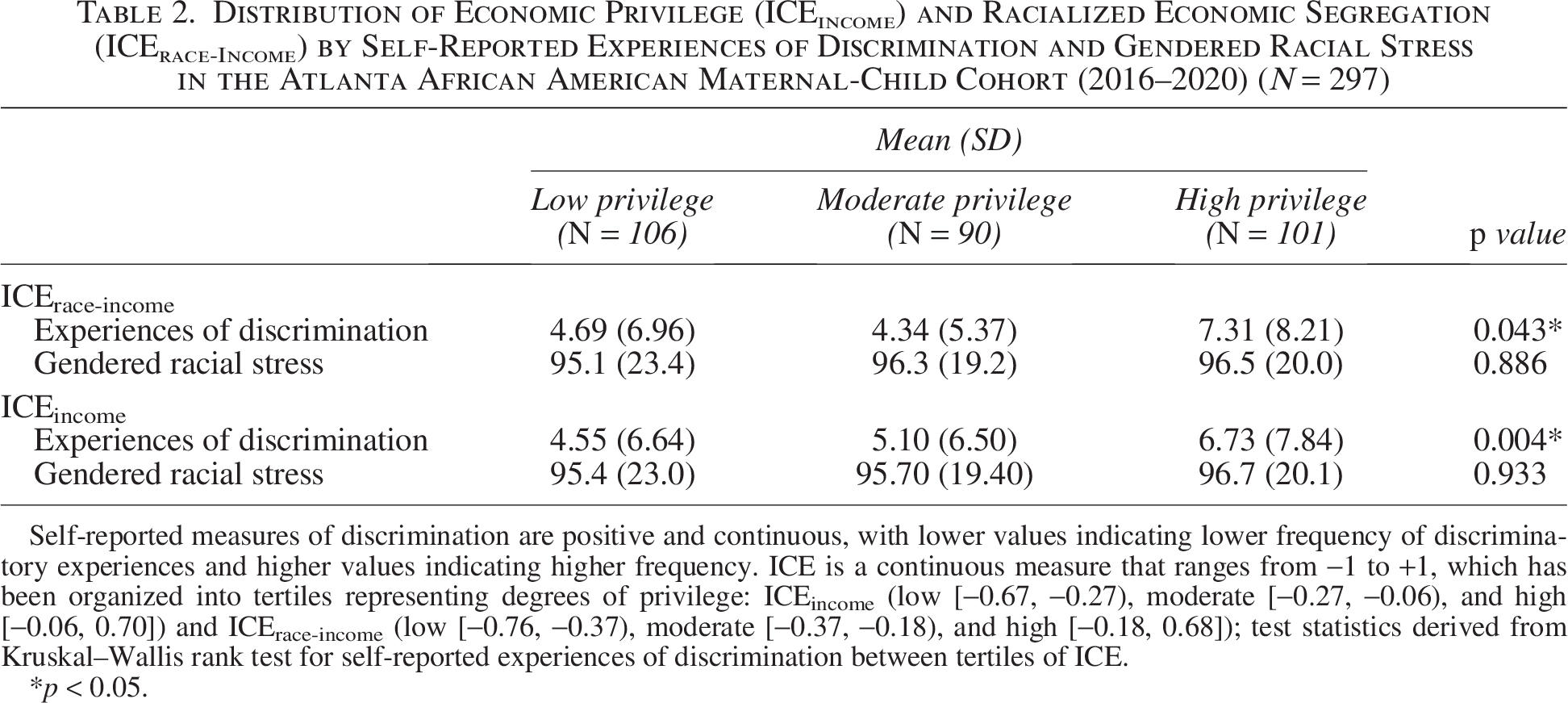
Self-reported measures of discrimination are positive and continuous, with lower values indicating lower frequency of discriminatory experiences and higher values indicating higher frequency. ICE is a continuous measure that ranges from −1 to +1, which has been organized into tertiles representing degrees of privilege: ICEincome (low [−0.67, −0.27), moderate [−0.27, −0.06), and high [−0.06, 0.70]) and ICErace-income (low [−0.76, −0.37), moderate [−0.37, −0.18), and high [−0.18, 0.68]); test statistics derived from Kruskal–Wallis rank test for self-reported experiences of discrimination between tertiles of ICE.
*p < 0.05.
In adjusted models, an increase in the frequency of self-reported experiences of discrimination was associated with a significant decrease in gestational age (β = −0.08, 95% confidence interval [CI]= −0.13, −0.03) (Fig. 2; Supplementary Table S2). While the point estimate for the association between self-reported experiences of discrimination and birthweight z-score was negative, the CI included the null value (β = −0.01, 95% CI = −0.02, 0.01) (Fig. 2; Supplementary Table S2). We observed null associations between self-reported experiences of gendered racial stress, ICEincome, ICErace-income scores, and birth outcomes in adjusted and unadjusted models (Fig. 2; Supplementary Table S2).
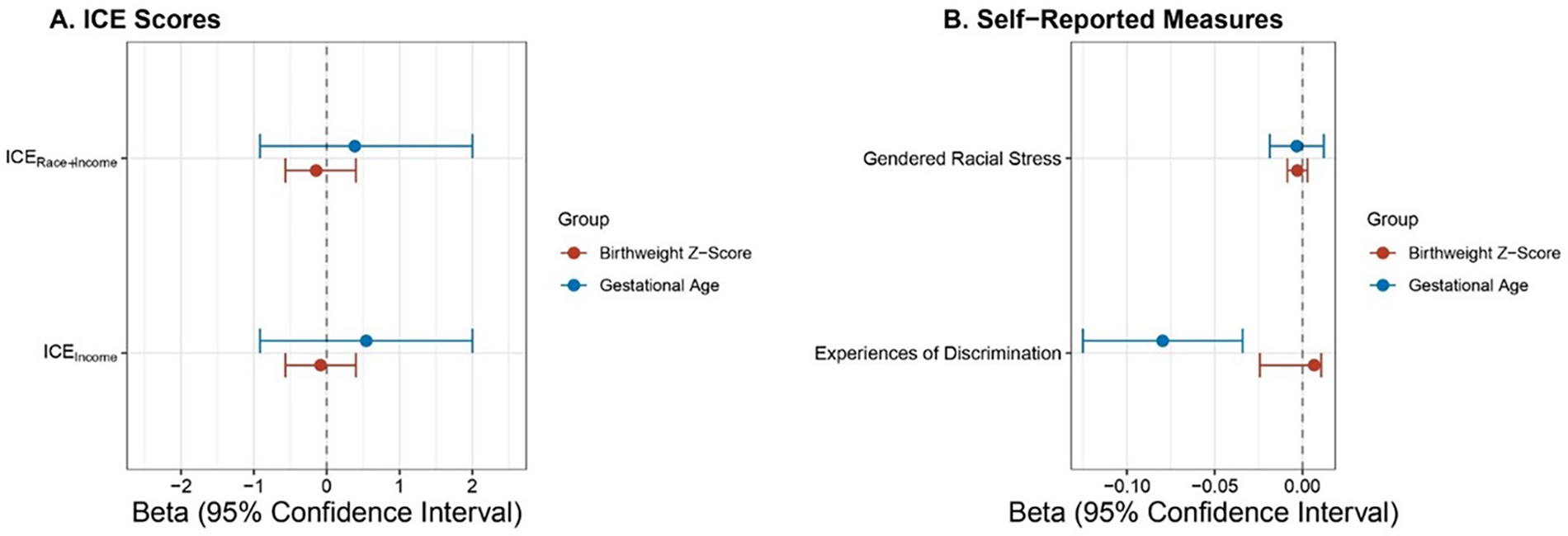
Adjusted linear regression coefficients and 95% confidence intervals for gestational age at delivery and birthweight z-scores with an increase in
In analyses examining PTB and SGA as outcomes, we observed that increasing frequency of experiences of discrimination was associated with an increase in odds of PTB (odds ratio [OR] = 1.04, 95% CI = 1.00, 1.11) (Supplementary Table S3). SGA was not strongly associated with ICE scores or self-reported measures (Supplementary Table S3). We observed no significant associations with term birthweight (Supplementary Table S4).
DISCUSSION
Within a prospective cohort of AA birthing people, we observed that self-reported experiences of discrimination across the lifespan were associated with a statistically significant decrease in gestational age at delivery but not birthweight z-scores. ICE metrics, which reflect racial and economic segregation at the census tract level, were not associated with adverse birth outcomes. Our findings have important public health and policy implications for studies assessing the impact of racism on perinatal health outcomes, underscoring the critical importance of including measures of individual experiences to assess health impacts of structural discrimination. Structural racism can not only be defined by objective measurements of success, wealth, or privilege, such as income, but must also incorporate individual-level perspectives that illustrate how systems reinforce discrimination.
The results from our analysis of self-reported experiences of discrimination across socioeconomic strata point to older age and higher educational attainment as indicators for higher frequency of experiences of discrimination. Our findings also demonstrate that individuals in all levels of economic privilege experience gendered racial discrimination at similar frequency, and experiences of racial discrimination are experienced with greater frequency in areas of highest economic privilege. These findings are supported by both qualitative and quantitative research. For example, in a qualitative study on experiences of racism and gender discrimination among AA birthing people during pregnancy, participants expressed encountering racism and gender discrimination with high frequency during pregnancy and identified gendered racial discrimination as a significant source of stress during this critical developmental period. 40
Racialized economic segregation refers to historic and contemporary practices and policies that restrict both social mobility and generation of socioeconomic capital for minoritized populations. While we did not observe associations between economic privilege, racialized economic segregation (i.e., ICE scores), and birth outcomes, literature has shown that individuals who live in areas with extreme economic polarization (ICEincome) or racialized economic segregation (ICErace-income) experience adverse perinatal health outcomes and severe maternal morbidity.41,42 It is possible that differences are the result of the underlying makeup of the study populations, as ours solely included AAs. This is the first study to examine associations between ICE scores and birth outcomes in metropolitan Atlanta, which may represent a unique geographic area as AAs makeup over 50% of the population. To date, one study on birth outcomes and associations with ICE has been conducted in the southern United States, 43 but none in Georgia, which is ranked 39th in the nation for maternal mortality and 44th for concentrated disadvantage. 44
Our study builds on existing literature in several important ways. Our cohort is comprised exclusively of self-identified AA birthing people who have no comorbid conditions, which is a unique feature of this study in the landscape of research investigating associations between socioeconomic status as measured by ICE variables and maternal health outcomes. A 2022 systematic review by Larabee Sonderlund et al. found that maternal comorbidities may exist on the causal pathway associations between racialized economic segregation (as measured by ICE) and birth outcomes (i.e., maternal comorbidities are acting as mediators). 45 Our cohort provides insight into impacts of structural racism on AA birthing people in the context of otherwise healthy pregnancies. Prior research examining adverse pregnancy outcomes has leveraged ICE metrics corresponding to areas where participants spent the majority of their early childhood in order to account for chronic stress and intergenerational impacts of structural racism. 46 In this study, we utilized current location of residence, which provides insight into impacts of structural racism in participants’ everyday environments. Published research from investigations on ICE and adverse birth outcomes are not unanimous in their findings. 47 In a study on redlining and PTB in New York City, investigators found that women who lived in historically redlined areas were 55% more likely to deliver preterm than their counterparts who lived in non-redlined (“green”) census tracts. 48 However, these outcomes attenuated when controlling for the ICE metrics. Additionally, in a 2022 study investigating the relationship between racialized economic polarization, PTB, and infant mortality based in California, women who lived in areas at the extremes of poverty were significantly more likely than affluent women to experience PTB. 49 Similarly, a study by Krieger et al out of Boston found that participants in low-income neighborhoods were significantly more likely to deliver preterm. 50 Results from our sensitivity analyses measuring associations between ICEincome, ICErace-income and PTB were null. However, evidence demonstrates that Black birthing people across the United States are significantly more likely to deliver preterm than recently emigrated Black birthing people (<10 years), 51 suggesting that mechanisms that include racialized economic polarization are perhaps at play in the southern United States but may be comparatively more nuanced than what is observed in other regions.
We also observed that individuals who have greater economic wealth and who live in neighborhoods with greater concentrations of White people experience higher frequency of discrimination compared with individuals living in neighborhoods with greater concentrated disadvantage. Importantly, these findings highlight that wealth is not protective against experiences of discrimination for AA birthing people. Social support, however, is identified as an important potential intervention to consider. In a study on a community sample of AA church-going adults, it was demonstrated that social support significantly buffered associations between experiences of discrimination and psychological distress. 52 Cultivating community, according to that study, is an intervention that has the potential to attenuate negative impacts of discrimination on health outcomes. However, in a separate study on the impact of exposure to racism experienced by caregivers on Black children, outcomes demonstrated that cultural socialization was not significantly protective against anxiety and depressive symptoms exhibited by children. 53 Although that study’s findings and others demonstrate that social support may play a role in the lived experience of racism, aiming to attenuate its effect is not the answer—systemic racism itself must be ameliorated.
The Atlanta African American Maternal-Child Cohort specifically recruits individuals who self-identify as AA and who are pregnant. As such, our participants experience, firsthand, the consequences of structural racism for individuals with intersecting identities (both Black and female). Scientific research commonly uses race as a proxy for racism, which frames societal ills as individual failures and, importantly, comes dangerously close to perpetuating notions of racial essentialism. 54 The scientific community must think beyond race to interrogate our knowledge about how an individual’s experience of racism contributes to negative health outcomes. Black birthing people are four times as likely to die from pregnancy-related complications compared with White birthing people, and there is much to be gleaned from lived experience of pregnancy when investigating this disparity. 55 Including Black birthing people in scientific research, and centering their intersectional experiences, is critical to fully conceptualizing the impact of gendered racial discrimination and ultimately reducing racial disparities in adverse birth outcomes.
Our study has several strengths and limitations. First, we included two validated measures of discrimination, one of which was designed specifically to assess intersectional racial and gender discrimination. However, measures of self-reported racial discrimination are subject to exposure misclassification, which may introduce bias toward the null and mask true differences in birth outcomes among individuals with varying experiences of discrimination over the lifetime. Additionally, selection for this study was restricted to individuals who were already presenting for prenatal care and who were willing to express interest in participating in a research study. This approach to recruitment may introduce selection bias, thus restricting our ability to capture associations between exposure and outcome only among individuals who are presenting for prenatal care and who voluntarily expressed interest in participation. Both of these factors can be influenced by access to health care and trust (or lack thereof) in scientific research and the medical enterprise. There is a growing body of literature that provides data to evidence Black women’s experiences of racial bias in the health care setting,56,57,58,59 and participants in this study may be more likely to experience racial bias than those who do not present for care. This would bias our results away from the null and increase likelihood of observing associations between experiences of discrimination and adverse birth outcomes, compared with the general population.
Utilization of the ICE metrics is an important strength of this study, allowing for a multidimensional analysis of structural racism incorporating both racial composition and socioeconomic markers (rather than one variable alone, such as racial majority, income, or median home value). Additionally, ICE measures polarization between individuals at extremes of privilege, rather than summarizing a geospatial area using the average measure for multiple demographic variables (e.g., the social vulnerability index or neighborhood depravity index). Calls for incorporating measures of self-reported experiences of racism in the research landscape have grown in recent years, and our incorporation of both geospatial and individual-level metrics measuring racial discrimination in this study fills gaps in existing literature, providing a more nuanced approach to investigating racial bias and social disadvantage in the context of pregnancy among Black women. Additional strengths of this study include ascertainment of pregnancy outcomes through medical record abstraction among those who presented for clinical prenatal care; thus, precision and accuracy of gestational age dating are high. All participants in the present study self-identify as AA, which we recognize as a strength in the context of the history of scientific research excluding participants on the basis of race and gender, and in light of ongoing disparities underlying the maternal health crisis in the United States. Nonetheless, we recognize that racial homogeneity may be considered a limitation for the generalizability of our results to a racially heterogenous population, at large. We posit, however, that the emphasis placed on comparison of this cohort to the white population is rooted in racial hegemony and should be interrogated through an interpretation of our results.
CONCLUSIONS
Our study reveals that participants who live in areas with higher economic privilege and increased racialized economic segregation experience, on average, higher frequency of racial discrimination when compared with participants who live in areas with lesser economic privilege. Of note, we observed that increased frequency of self-reported experiences of discrimination, but not objective measures of racialized economic segregation, was associated with a statistically significant reduction in gestational age only. Opportunities to expand on this research include expanding sample size, measuring clinical significance of adverse birth outcomes associated with experiences of gendered racism, and incorporating the impact of geospatial racial, economic, and social segregation on both physical and mental health. Extrapolating these findings to evidence-based discussions on increased maternal morbidity among Black birthing people across the socioeconomic spectrum, we argue that assessing the impact of individual and interpersonal structural racism is necessary to (1) assess root causes of racial disparities in maternal health accurately and (2) design effective risk mitigation strategies. Racism, not race, must be the center of these discussions. Assessing multilevel indicators of structural racism, including the internalized and interpersonal, is critical to understanding root causes of health disparities, particularly in the perinatal period.
AUTHORS’ CONTRIBUTIONS
J.A.E. was responsible for formal analysis, investigation, writing—original draft, writing—reviewing and editing, and visualization. K.O. was responsible for visualization and writing—reviewing and editing. A.L.D. contributed to investigation, resources, data curation, writing—reviewing and editing, project administration, and funding acquisition. D.B.B. contributed to methodology, validation, resources, data curation, writing—reviewing and editing, supervision, and funding acquisition. C.C.H. contributed to methodology, resources, and writing—reviewing and editing. P.A.B. contributed to investigation, resources, data curation, writing—reviewing and editing, project administration, and funding acquisition. P.B.R. contributed to methodology, validation, resources, data curation, writing—reviewing and editing, supervision, and funding acquisition. D.L. contributed to conceptualization, methodology, investigation, writing—reviewing and editing, and funding acquisition. E.J.C. contributed to investigation, resources, data curation, writing—reviewing and editing, project administration, and funding acquisition. K.R.T. contributed to writing—reviewing and editing. Y.T. contributed to data curation, methodology, resources, and writing—reviewing and editing. S.M.E. was responsible for conceptualization, methodology, investigation, writing—original draft, writing—reviewing and editing, and supervision.
Footnotes
ACKNOWLEDGMENT
The authors would like to thank the study participants who participated in the Atlanta African American Maternal-Child Cohort study and the clinical health care providers and staff at the prenatal recruiting sites for helping with data collection.
AUTHOR DISCLOSURE STATEMENT
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
FUNDING INFORMATION
This work was supported by the National Institute of Health (NIH) research grants (R01NR014800, R01MD009064, R24ES029490, R01MD009746, R21ES032117, K01ES035082, F30ES036439), NIH Center Grants (P50ES026071, P30ES019776, UG3/UH3OD023318, U2CES026560), and the U.S. Environmental Protection Agency center grant (83615301). S.M.E. was additionally supported by the JPB Environmental Health Fellowship.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.