
Abstract
Background:
An estimated 450,000 cases of shigellosis occur annually in the United States. Outbreaks have been associated with food, water, child daycare centers, and men who have sex with men. However, for sporadic infections, which account for the majority of cases, risk exposures are poorly characterized.
Methods:
Foodborne Diseases Active Surveillance Network (FoodNet) conducts active, laboratory-based shigellosis surveillance in 10 US sites. We interviewed cases with illness onset during 2005 about exposures during the week before symptom onset using a standardized questionnaire. The proportion of patients who denied nonfood risks was used to estimate the burden attributable to foodborne transmission.
Results:
Overall, 1494 cases were identified. The approximate incidence was 3.9/100,000, with the highest rates among children aged 1–4 years (16.4) and Hispanics (8.4). Of the 929 cases interviewed, 223 (24%) reported international travel in the week before symptom onset. Of the 626 nontraveling cases with complete risk factor information, 298 (48%) reported exposure to daycare or a household member with diarrhea; 99 (16%) reported drinking untreated water or recreational exposure to water; and 16 (3%) reported sexual contact with a person with diarrhea. Two hundred and fifty-nine (41%) denied all nonfood exposures examined.
Conclusions:
Sporadic shigellosis is most common among young children and Hispanics. Common exposures include international travel and contact with ill persons or daycare. However, more than one-third of US shigellosis cases annually might be due to food consumed in the United States.
Introduction
Humans are the only reservoir, and the small infectious dose (10–200 organisms) for Shigellae facilitates efficient person-to-person spread. Children aged <5 years have the highest approximate incidence rate. Persistent and widespread outbreaks of S. sonnei infection have commonly occurred in child daycare centers, with illness first occurring in the children and then spreading to staff and family members (Brian et al., 1993; Drees and Hathcock, 2004; Garrett et al., 2006). These outbreaks may be accompanied by community-wide increases in S. sonnei cases, often occurring in periodic “waves” (Shiferaw et al., 2004). Shigellosis has efficiently spread among close-knit and religious communities, presumably from person-to-person spread (Sobel et al., 1998; Garrett et al., 2006). Sexual transmission of shigellosis has also been observed in men who have sex with men (Bader et al., 1977; CDC, 2001, 2005; Aragón et al., 2007). For the purposes of epidemiologic investigations, serogoup identification of Shigellae is helpful. S. flexneri has been more commonly identified than S. sonnei among international travelers (Keusch et al., 1998), whereas S. sonnei has been more frequently found in daycare-associated cases.
Well-documented outbreaks have identified specific risk factors and contaminated vehicles for infection, including international travel (Spika et al., 1987; Lew et al., 1991), contaminated recreational water (Keene et al., 1994; Fleming et al., 2000), drinking water (CDC, 1996), and contaminated foods (Kaiser and Williams, 1962; Spika et al., 1987; Davis et al., 1988; Reeve et al., 1989; Lee et al., 1991; Lew et al., 1991; Hedberg et al., 1992; Dunn et al., 1995; CDC, 2000; Naimi et al., 2003; Reller et al., 2006). Foodborne outbreaks of shigellosis have been linked to a number of raw or undercooked foods, including lettuce (Davis et al., 1988), parsley (Naimi et al., 2003), bean dip (CDC, 2000), cold sandwiches (Hedberg et al., 1992), potato salad (Kaiser and Williams, 1962; Lew et al., 1991), tofu salad (Lee et al., 1991), oysters (Reeve et al., 1989), tomatoes (Reller et al., 2006), and hamburgers (Spika et al., 1987). From 1998 to 2004, 90 foodborne outbreaks of shigellosis were responsible for 5324 illnesses reported to CDC by state and local health departments (Blanton et al., 2006).
While documented outbreaks contribute to the burden of illness caused by Shigellae, most shigellosis cases are sporadic, that is, not associated with recognized outbreaks. It is likely that some cases are acquired from eating foods contaminated with Shigella, but no multistate, population-based studies have investigated risk exposures for sporadic shigellosis.
Infections transmitted by food are among the most amenable to prevention by regulatory action. Determining the burden of food-related illness from specific organisms is important in assisting policymakers as they set priorities for food safety interventions. The Foodborne Diseases Active Surveillance Network (FoodNet), the principal foodborne disease component of Centers for Disease Control and Prevention's (CDC) Emerging Infections Program, is a collaborative project of the CDC, selected state health departments, the US Department of Agriculture's Food Safety and Inspection Service, and the US Food and Drug Administration. FoodNet, which is demographically similar and represents approximately 15% of the US population, conducts active, laboratory-based surveillance for Shigella and other pathogens commonly transmitted through food to understand better the epidemiology of foodborne diseases in the United States (Scallan, 2007).
The objectives of this FoodNet study were (1) to examine differences in sporadic shigellosis incidence rates by demographic characteristics, species, and sites; (2) to identify potential risk factors for sporadic shigellosis; and (3) to derive an estimate of sporadic, domestically acquired shigellosis potentially transmitted by food.
Materials and Methods
Study population
Cases included those that were laboratory-confirmed among patients in 10 FoodNet sites: Connecticut, Maryland, Minnesota, New Mexico, Oregon, Tennessee, and selected counties in California, Colorado, Georgia, and New York; these jurisdictions account for 15% of the US population, and their racial composition is similar to that of the United States as a whole.
Data collection
As part of routine active surveillance, investigators at each site identify laboratory-confirmed cases through reports to public health departments and by contacting all clinical laboratories serving the FoodNet surveillance area at least on a monthly basis. At least twice yearly, laboratory audits are conducted to ensure complete ascertainment of shigellosis cases at each clinical laboratory. Demographic information is routinely collected on all cases ascertained in FoodNet. From January 1–December 31, 2005, attempts were made to interview by telephone all cases with laboratory-confirmed shigellosis regarding potential risk. Patients were asked about potential exposures in the week before symptom onset, including international travel; primary source of drinking water; exposure to recreational water; work or attendance at a childcare center; and contact with persons who had diarrhea, including children, household members, or sex partners. A childcare setting was defined as any place wherein at least two unrelated children, preschool age or younger and not living in the same household, were cared for.
Analysis
Data were analyzed using SAS (SAS Institute, Cary, NC, version 9.1). We calculated rates using population estimates from the US Census Bureau. Cases linked to an outbreak, as determined by state and local epidemiologists, were excluded from further analysis. We compared risk factors for sporadic cases by demographic characteristics, species, and sites. Cases who reported international travel in the week before symptom onset were considered travel-associated. Sporadic cases in patients who denied all other risk exposures were considered to represent an estimate of the proportion of sporadic shigellosis infections that might have been acquired through consumption of contaminated food in the United States. If a patient answered “no” to a general question but “yes” to a more specific question in that category, for example, “no” to recreational water exposure but “yes” to a specific type of recreational water contact, then the more specific answer was considered accurate.
Results
During 2005, FoodNet sites ascertained 1494 cases of shigellosis; 60 cases were identified as outbreak-associated and excluded from further analysis. Of the remaining 1434 cases, the approximate incidence of shigellosis among the FoodNet sites was 3.9 cases per 100,000 persons. The approximate incidence rates varied by state, where the highest rates were in California (8.8), Tennessee (8.3), New Mexico (6.8), and Georgia (6.3). The lowest rates were in New York (1.3), Minnesota (1.6), Connecticut (1.7), and Maryland (1.7). Illness occurred most frequently (32%) between August and October. Most (96%) isolates were speciated: 1032 (72%) were S. sonnei; 315 (22%) were S. flexneri; 16 (1%) were S. boydii; and 9 (0.6%) were S. dysenteriae. S. sonnei accounted for 54–92% of all shigellosis cases in the 10 sites.
Demographic characteristics
Figure 1 shows the distribution of shigellosis rates by age and species. Age-specific approximate incidence peaked among 1- to 4-year olds (16.4), slightly decreased among 5- to 9-year olds (14.1), and sharply decreased among 10- to 19-year olds (2.2). Approximate incidence was slightly higher among 20- to 29-year olds (3.1) and 30- to 39-year olds (3.3), then consistently decreased for all other subsequent age groups. The pattern of the age profiles were similar for S. sonnei and S. flexneri, but the elevated risk in the 1- to 9-year age group was more pronounced for S. sonnei than for S. flexneri infection (Fig. 1).
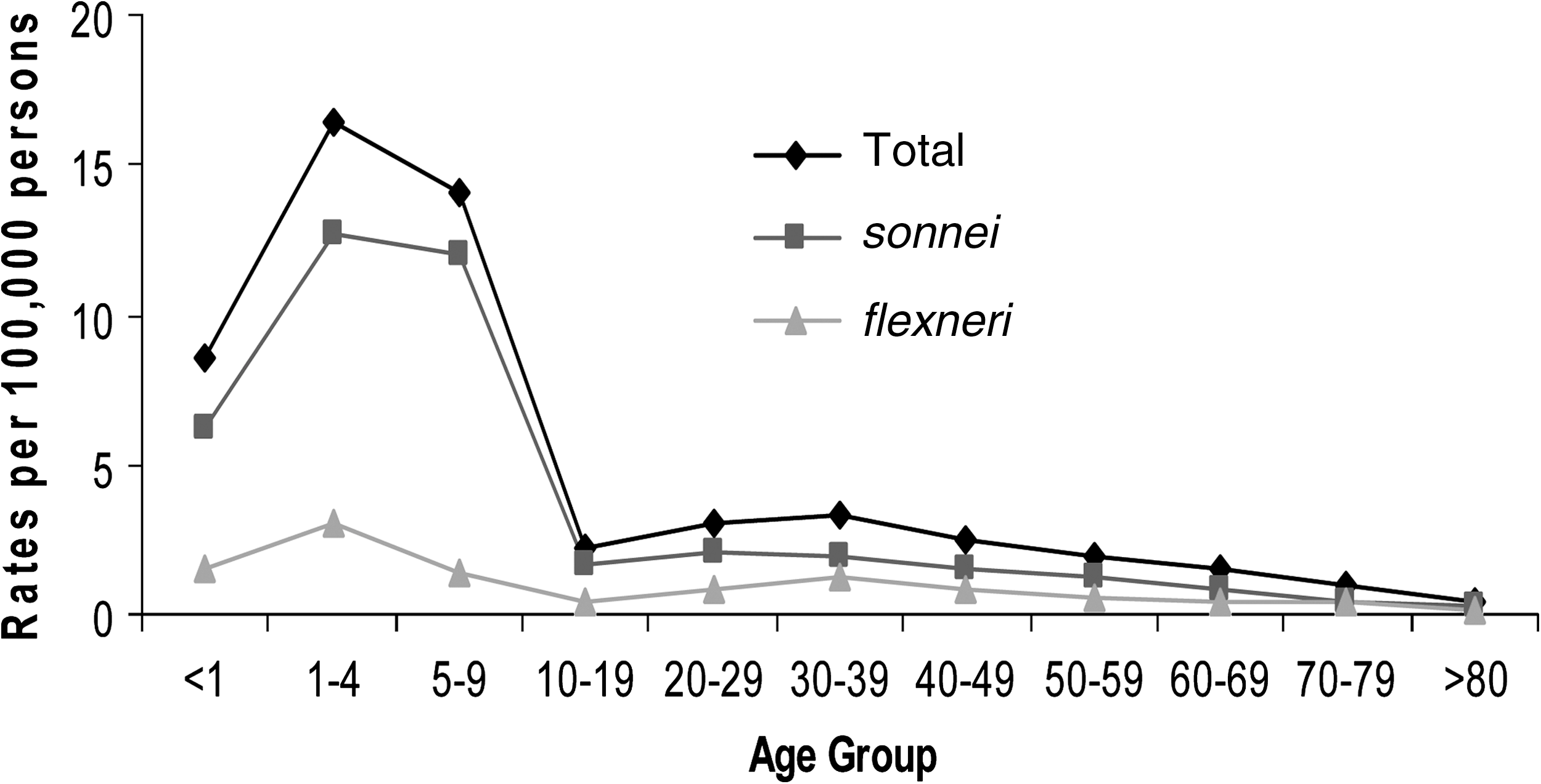
Shigellosis rates by age group and serogroup—FoodNet, 2005.
The overall approximate incidence for men was 3.8/100,000 population and for women was 3.7/100,000 population. Hispanics had the overall highest approximate incidence (8.6), followed by Native Americans/Alaskan Natives (7.0), blacks (3.8), and whites (3.0). Race- and ethnicity-specific rates varied by state, with the highest rates among Native Americans/Alaskan Natives in California (18.4) and New Mexico (13.3) and Hispanics in Minnesota (15.4) and California (12.7). S. sonnei was the predominant species within each racial and ethnic group.
Risk exposures
Interviews were completed with 929 (65%) of the 1434 eligible sporadic shigellosis cases. Reported risk exposures (potentially more than one per case) are shown in Figure 2. Of the 929 cases interviewed, 223 (24%) reported international travel in the week before symptom onset. An additional 80 (9%) had incomplete exposure information. Of the remaining 626 cases, 298 (48%) reported attending or working in daycare or contact with a child or household member with diarrheal illness; 99 (16%) reported drinking untreated water or recreational exposure to water; and 16 (3%) reported sexual contact with a person with diarrhea. In addition, 45 (7%) of the 626 persons who did not travel internationally reported more than one exposure.
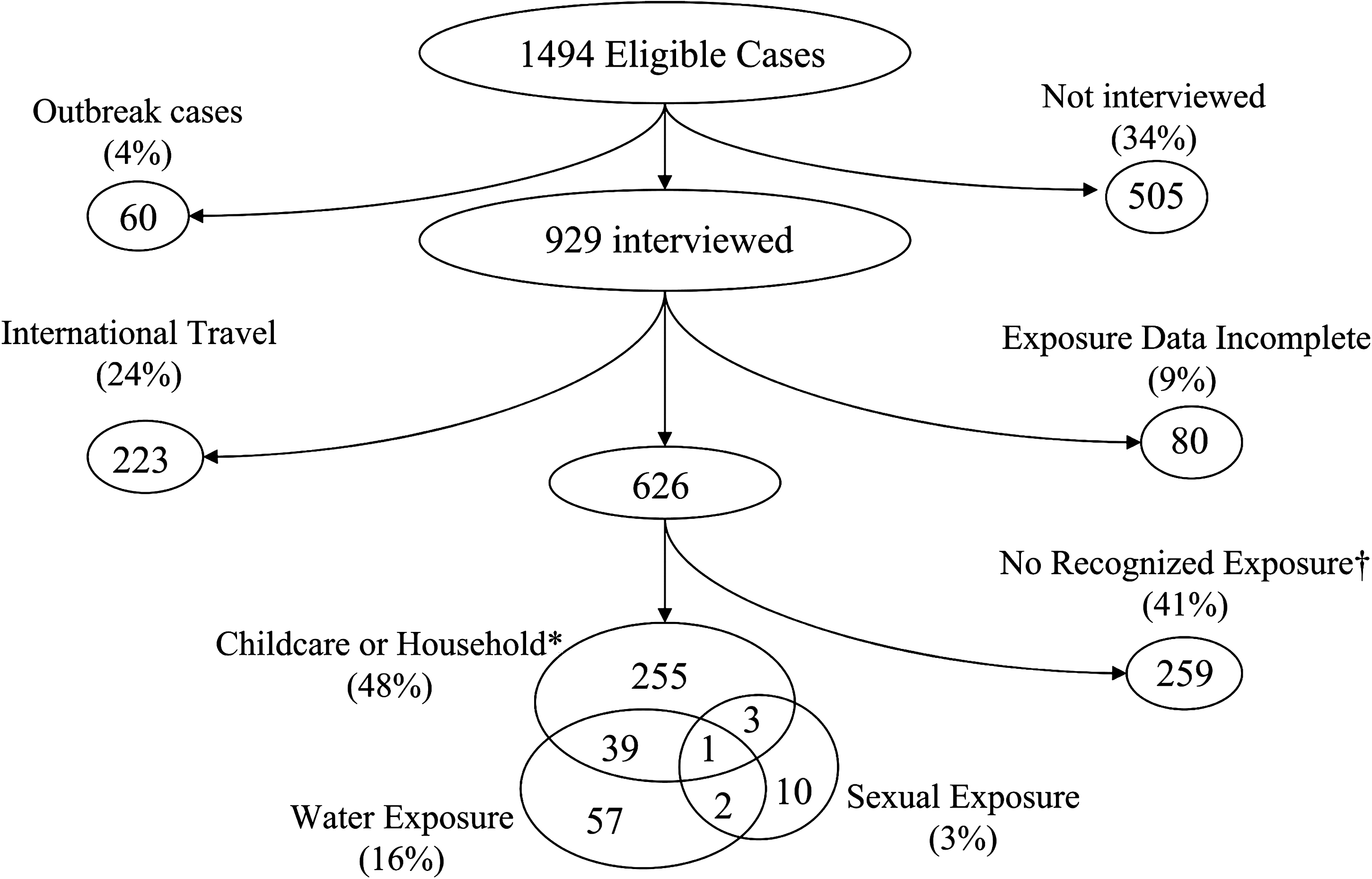
Shigella cases by multiple exposures—FoodNet, 2005. *Includes attending or working in childcare, nonsexual contact, including children, with a household member with diarrhea. †Denied all risk exposures on interview (estimate of proportion attributable to foodborne exposures in the United States).
Risk exposures by species
We compared the prevalence of risk exposures among cases with S. sonnei or S. flexneri, the two most common species identified (Table 1). The proportion reporting international travel, water, and sexual exposures were similar for both species. However, S. sonnei cases were more likely than S. flexneri cases to report a childcare or nonsexual household contact (58% vs. 18%; prevalence ratio [PR] 1.9, 95% confidence interval [CI] 1.7–2.2). This comparison was similar regarding attending or working in a childcare setting (S. sonnei 34% vs. S. flexneri 5%; PR 1.3, 95% CI 1.2–1.4) and having contact with a child or nonsexual contact with a household member with diarrhea (55% vs. 17%, PR 1.3, 95% CI 1.2–1.4).
Percentages within subtypes may total more than 100% since patients may have multiple risk exposures and also may total less than 100% since those reporting no risk exposures, but not having a response to all risk exposure questions, would not be included in any category.
If traveled internationally, not included in other exposure categories.
Work or attendance in childcare facility; or household member with diarrhea in 7 days before illness onset.
Diarrhea contact in the 7 days before illness onset, with partner with diarrhea.
Cases who responded “No” to all exposures.
PR, prevalence ratio; CI, confidence interval.
Estimate of proportion acquired from food
Of patients who answered all requisite questions, 259 denied all typical nonfood risk factors for shigellosis and were considered possibly foodborne (Fig. 2); they represent 31% of the 849 sporadic cases with sufficient response data and 41% of the 626 sporadic cases who had not traveled outside the country. The proportion of S. sonnei patients denying all risk exposures, and therefore classified as possibly foodborne, was 32% as compared with 68% of S. flexneri cases (PR = 0.5, 95% CI 0.4–0.6; Table 1).
Of the 1494 cases, 505 were not interviewed. Of these, 226 (45%) were in Tennessee, and 279 were distributed among seven sites, each of which accounted for 2–18% of noninterviewed cases. Tennessee experienced a wave of shigellosis accompanied by several large daycare-associated outbreaks of S. sonnei infection in 2005, making comprehensive case follow-up difficult. To account for the possibility that some Tennessee outbreak-associated cases were reported as sporadic, we also analyzed the data excluding all Tennessee cases. The patterns and proportions in this analysis remained consistent with the analysis that included Tennessee; the proportions of S. sonnei and S. flexneri cases denying all risk exposures were 46% and 67%, respectively. Similarly, we found that removing other sites' cases from the analysis did not alter the findings (Fig. 3).
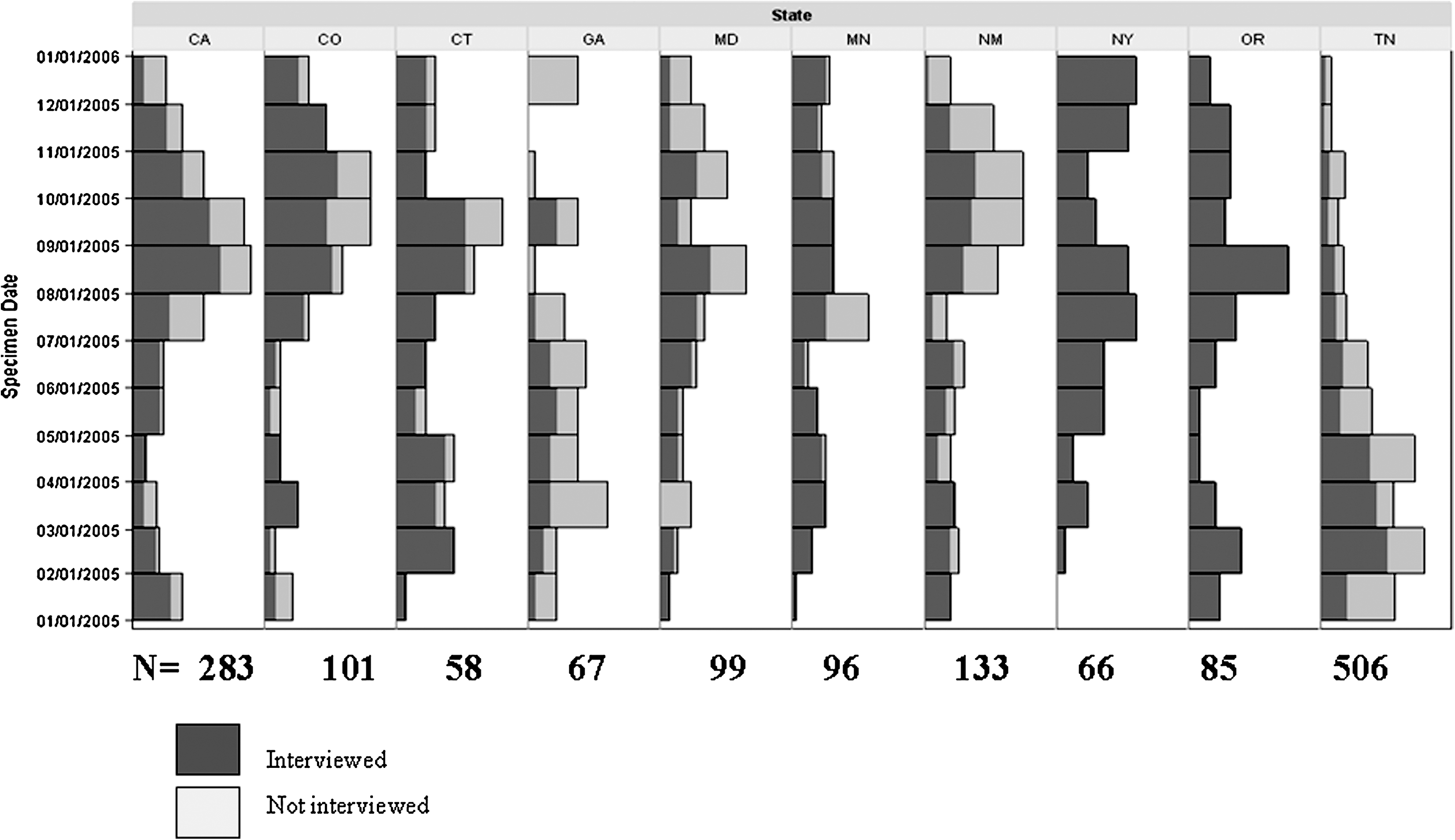
Distribution of Shigella cases by state, month, and interview status.
Discussion
The vast majority of reported cases of shigellosis—96% in our study—are sporadic, that is, apparently unassociated with any recognized outbreak. Given that foodborne transmission has been documented in many shigellosis outbreaks, it is likely that a significant proportion of sporadic cases acquired infection through contaminated food. This proportion is important in assessing and improving foodborne disease prevention efforts. Three previous studies have estimated the percentage of shigellosis transmitted by food in the United States, England and Wales, and Australia to be 20%, 8.2%, and 10.7%, respectively (Mead et al., 1999; Adak et al., 2002; Hall et al., 2005). These studies were based on expert opinion and extrapolation from outbreak data, which may not be representative of sporadic illnesses, to estimate the foodborne proportion of all shigellosis, regardless of outbreak association. In contrast, we limited our analysis to sporadic cases and used surveillance and interview data from a defined population to estimate the foodborne fraction as a diagnosis of exclusion: 31% of all persons with sporadic shigellosis and 41% of persons with domestically acquired sporadic shigellosis denied all typical risks for person-to-person acquisition and high-risk water exposures.
Consistent with data from outbreak investigations, we found cause to believe that a large proportion of sporadic shigellosis is transmitted directly from one person to another (Brian et al., 1993; Shane et al., 2003; Garrett et al., 2006). Most childcare-associated shigellosis outbreaks are caused by S. sonnei; we found particularly high rates of S. sonnei infection among young children, and a high proportion of our S. sonnei cases reported attendance at or work in a childcare center. However, some person-to-person transmission may have been acquired through food. This transmission could be prevented if we protected the food supply.
During 2005, Tennessee experienced a general increase in shigellosis accompanied by several large daycare-associated outbreaks of S. sonnei infection. However, the proportion of Tennessee cases reported as associated with an outbreak did not reflect these events. The knowledge that Tennessee did experience outbreaks of shigellosis that were not reflected in the frequency of outbreak-related cases gave us the opportunity to test the impact that the noninterviewed cases have on the data. To test the bias that misclassification may have introduced, we analyzed our data without Tennessee cases. Excluding Tennessee from the analysis resulted in a decrease in the proportion of S. sonnei cases reporting childcare and other nonsexual exposures, suggesting that this risk factor was inflated by the wave of shigellosis cases in Tennessee. However, an examination of rates in FoodNet by year suggests that the overall contribution of S. sonnei and S. flexneri in FoodNet in 2005 was consistent with previous years and that a similar wave of shigellosis occurred each year in different sites. Notably, the proportion of possibly foodborne shigellosis remained similar even when Tennessee cases from 2005 were excluded.
With numerous documented outbreaks associated with international travel, particularly travel to developing countries, it is reasonable to suspect that a substantial proportion of sporadic cases are also acquired abroad (Gross et al., 1979). Our data are consistent with this hypothesis: international travel in the week before symptom onset was reported by one-quarter of cases interviewed. This proportion was similar for infections caused by S. sonnei and those caused by S. flexneri. Of those that traveled, 66% traveled to Latin America in the week before illness onset and half of all travelers went to Mexico. Interestingly, S. sonnei was identified in the majority of Latin American travelers (80%), which was similarly seen in travelers to Asia (60%), Europe (56%), and Africa (55%). Although we did not interview controls, this proportion of shigellosis cases reporting international travel is certainly much greater than would be found in the general population; for example, a telephone survey in FoodNet sites during 2002–2003 found that only 212 (1.3%) of 16,435 respondents had traveled outside of the United States in the previous 7 days (CDC, 2004).
Our data did not support the notion that water is a major vehicle for sporadic shigellosis. Recreational water exposure or drinking surface or well water was reported by only a small proportion of cases.
Limitations
This study has several limitations. It has been estimated that only one in 20 cases of shigellosis is diagnosed and reported to public health authorities, because some patients may not seek medical attention, and some who do may not be tested (Mead et al., 1999). Our data were collected in a single year and within a limited population, thereby limiting their generalizability. Recall bias poses a possible limitation since cases may have forgotten or been unaware of their exposures; such recall bias would lead to an overestimation of the proportion that might be attributable to food.
We would not have identified instances of person-to-person transmission if patients had had contact with persons with undisclosed diarrhea or who had been shedding Shigella asymptomatically. In 2005, FoodNet did not collect ethnicity or race data on 35% of shigellosis cases. This may lead to a misrepresentation of the proportion and approximate incidence rate among ethnic and racial groups. Questions about contact with a sexual partner with diarrhea may not have been answered truthfully. This could lead to underreporting of sexual contact as a risk exposure, inflating the foodborne estimate. In contrast, the assumption that a reported traditional risk factor was the cause of a person's infection may substantially underestimate the proportion attributable to food consumed in the United States. Similarly, a physician bias in favor of testing persons with usual suspect exposures, for example, childcare attendance, would have led to an overrepresentation of such persons among those whose shigellosis was confirmed by culture, leading to an underestimate of the proportion attributable to food.
Conclusions
Childcare, person-to-person contact, and international travel have been associated with outbreaks of shigellosis, and our data suggest that they are frequently associated with sporadic cases of shigellosis as well. On the other hand, well water and recreational water use are not frequently found among sporadic cases of shigellosis. After contact with children in childcare centers or with household members who carry the pathogen, contaminated food may be the most common means of acquiring shigellosis that appears at first blush to be sporadic. While this may be an overestimation of the foodborne component of shigellosis among domestically acquired sporadic infections, it is the first attempt at quantifying the proportion in a manner that accounts for other well-known risk factors. Public health officials should look assiduously for potential common food sources among cases—especially those caused by S. flexneri—that appear to be clustered in time and space or that share serologic or molecular markers.
Footnotes
Acknowledgments
We thank the FoodNet Attributions WG for their support and guidance. This study was funded by the Centers for Disease Control and Prevention, National Center for Infectious Diseases; US Department of Agriculture, Food Safety Inspection Service; and US Food and Drug Administration, Center for Food Safety and Applied Nutrition.
Disclosure Statement
No competing financial interests exist.