
Abstract
Objective:
Trichinellosis is a foodborne parasitic disease that is acquired by humans through ingestion of raw or inadequately cooked meat containing larvae of different Trichinella species. During a high endemic year, Hunedoara County, part of Transylvania region, was the second most affected Romanian county, with an incidence of 84.8 cases per 100,000 inhabitants. The objective of this study was to bring new epidemiological and clinical data on human trichinellosis from an endemic former industrial area characterized by high rates of poverty and unemployment.
Patients and Methods:
Data have been collected from the medical charts of 492 patients (mean age, 27.6 years) found to have trichinellosis and admitted between 1996 and 2005 in two infectious disease hospitals. A brief review of relevant epidemiological and epizoological information regarding the evolution of the infection in this region was also considered.
Results:
Women (55.1%, n = 271), townsfolk (77.0%, n = 379), and unemployed (40.1%, n = 126) were the most affected categories. The clinical symptoms included myalgia (64.6%, n = 118), edema (45.3%, n = 223), and headache (38.6%, n = 190). Eosinophilia ranged between 10% and 19.99% in 28.0% (n = 138) of the cases. For 47.8% (n = 235) of the patients, the hospitalization period ranged from 1 to 7 days. Thiabendazole was administered in 72.0% (n = 329) of the cases.
Conclusions:
For a long period of time, trichinellosis represented a serious public health and ecological concern because of the favorable social, economic, cultural, and geographic conditions of this territory. Despite rich history, an overall decrease in the number of human trichinellosis cases over the 10-year study period was revealed and the decline might have been favored by the following positive aspects: improvement of sanitary conditions, implementation of a more reliable collaboration between veterinarians and pig breeders/consumers, education of the population, and a more careful supervision of the public health services.
Introduction
Hunedoara County, part of Transylvania region, is situated in the western-central Romania (Fig. 1) and accounts for a population of 485,712 inhabitants. In 1993, the year with the highest incidence of trichinellosis ever recorded in Romania (15.9 cases per 100,000 inhabitants), Hunedoara County was the second most affected county with an incidence of 84.8 cases per 100,000 inhabitants (Neghina et al., 2009b). The industrial and economical potential of the county was focused in its southern part until recently. This territory includes two important regions that proved over time to be highly endemic for trichinellosis: the coal mining region situated on the Valley of Jiu River neighboring and including the town of Vulcan, and the metallurgic region around and including the town of Hunedoara (Fig. 1).
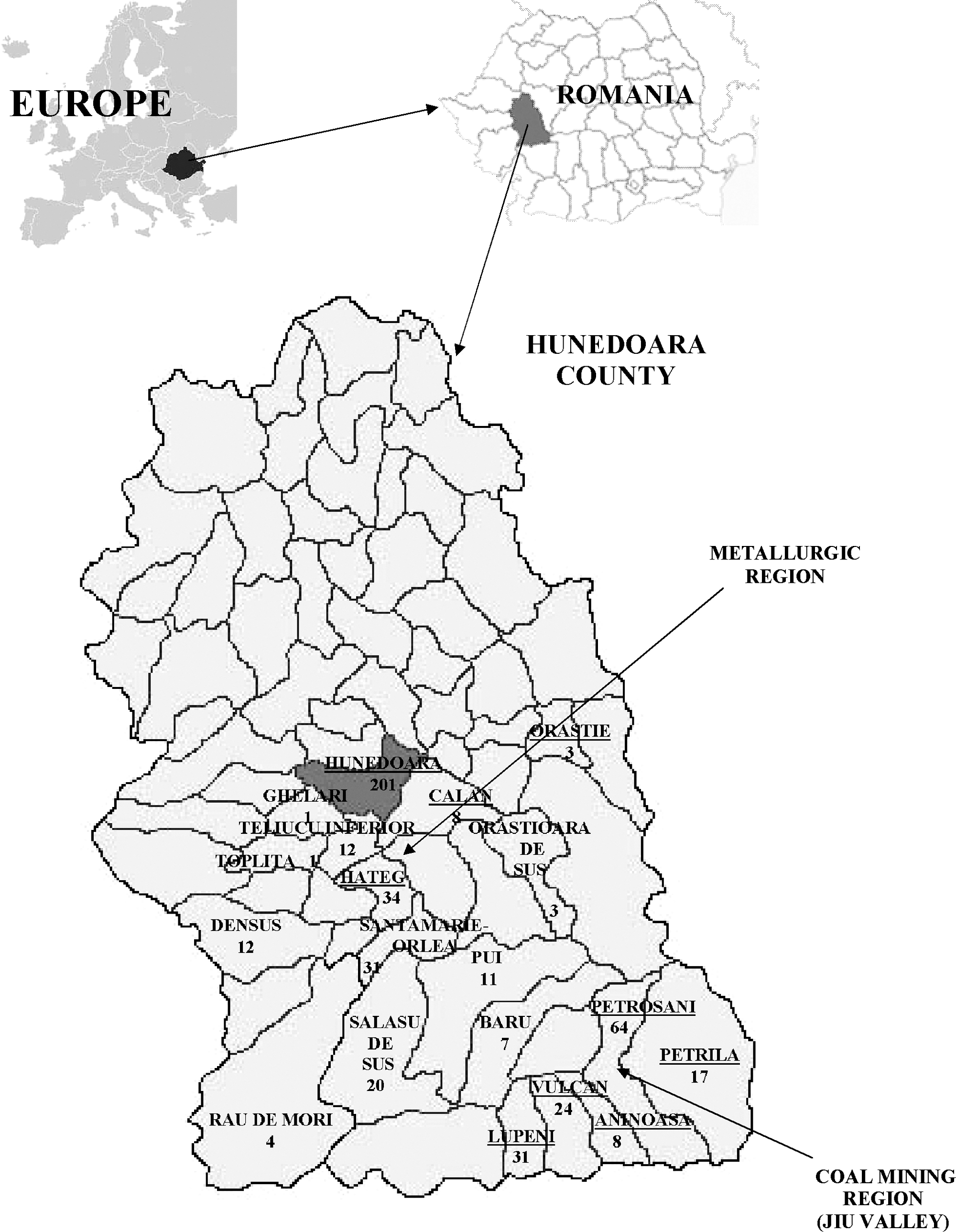
Geographic location of Hunedoara County and distribution of cases in the affected localities. Urban localities are underlined.
The objective of this study was to bring new epidemiological and clinical data on human trichinellosis from an endemic former industrial area characterized by high rates of poverty and unemployment. An overview of the relevant epidemiological and epizoological information regarding the evolution of the infection in this region was also considered.
Patients and Methods
Data have been collected from the medical charts of patients found to have trichinellosis and admitted between 1996 and 2005 in two infectious disease hospitals in Hunedoara and Vulcan. The following information was extracted: registration number of the medical record, age, sex, address, date and length of hospital stay, profession, clinical symptomalogy, course of the disease, routine laboratory investigations, and specific therapy. Diagnosis was established according to the algorithm for diagnosing acute Trichinella infections in humans (Dupouy-Camet and Bruschi, 2007), the confirmation criterion being either a positive serology or a positive muscular biopsy. Clinical course of the disease (where available) was established in conformity with the WHO guidelines (Dupouy-Camet and Bruschi, 2007).
The brief overview of the past situation of trichinellosis in the studied area was based upon the review of articles and books published locally by prestigious Romanian researchers.
Statistical evaluation was performed using the software package SPSS version 15.0. All patient characteristics are expressed as mean ± standard deviation. Comparison between patient groups was performed using the independent samples T-test and nonparametric Mann–Whitney test, where appropriate. A p-value of less than 0.05 was regarded as statistically significant.
Results
The study group included 492 patients, of whom 353 were hospitalized in Hunedoara and 139 in Vulcan. The cases were aged 7 months to 78 years (27.6 ± 17). Of them, 314 (63.8%) were adults (over 18 years old) and 178 (36.2%) were children (aged 0–17 years). Age group distribution is highlighted in Table 1. Most of the patients admitted to the hospitals were women (55.1%, n = 271). No statistically significant difference was found between men and women with respect to age (p = 0.197, independent samples T-test). Men predominated in the age groups of 0–9 years (55.2%) and 40–49 years (54.3%). According to their place of inhabitance, 379 patients (77.0%) were townsfolk and 113 (23.0%) were villagers. The number of cases diagnosed in each of the affected localities is shown in Figure 1. Most of the cases (33.1%, n = 163) were registered in 1997 (Fig. 2). The seasonal classification indicated that 316 individuals (64.2%) were admitted to hospital during winter (December to February), 111 (22.6%) during spring (March to May), 42 (8.5%) during autumn (September to November), and 23 (4.7%) during summer (June to August). The distribution on professional categories showed that most of the adult patients (40.1%, n = 126) were unemployed (Table 2). The length of hospital stay ranged between 2 and 25 days (8.6 ± 3.6) with the following distribution: 1–7 days in 223 patients (45.3%), 8–15 days in 235 patients (47.8%), and 15–29 days in 34 patients (6.9%).
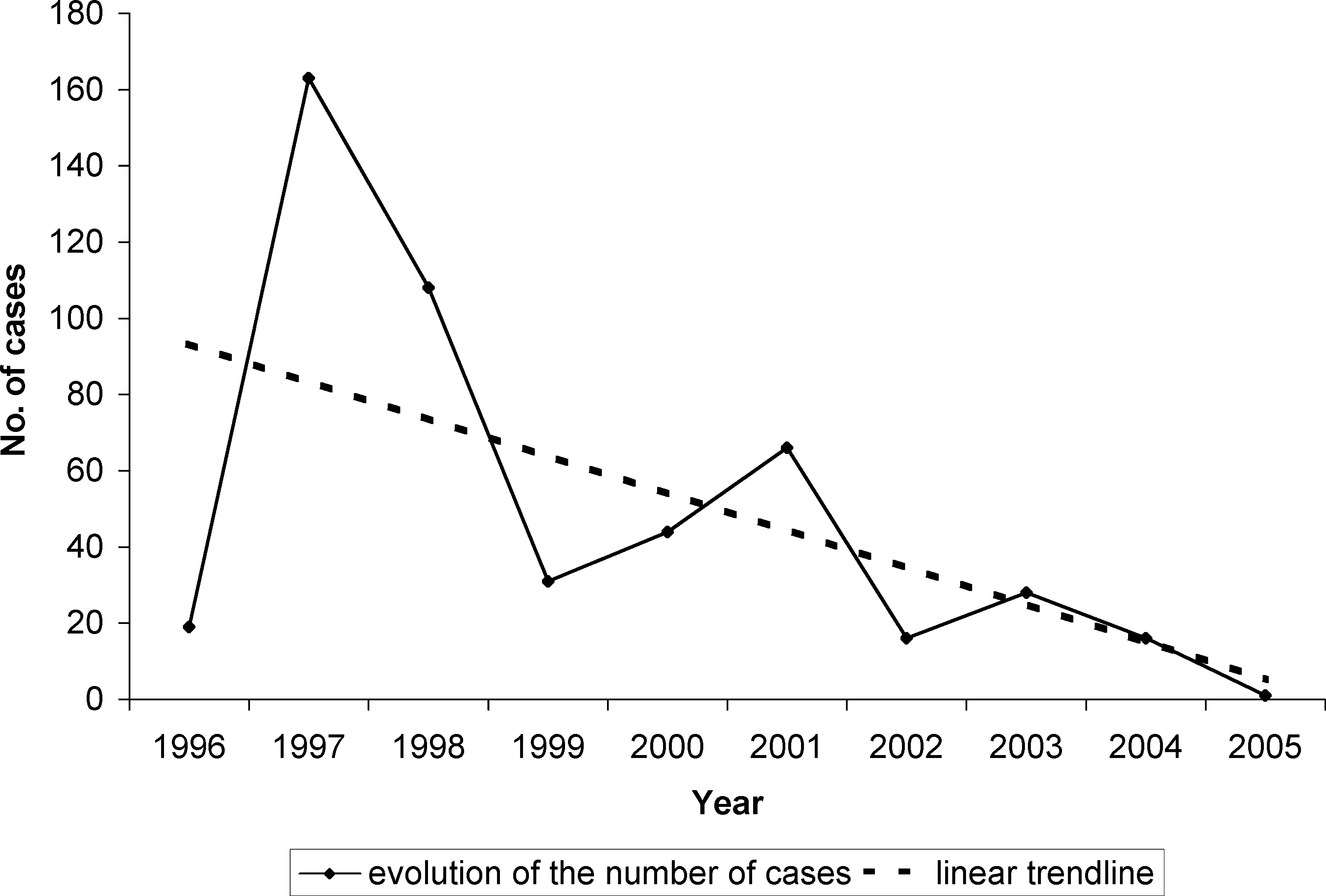
Distribution of cases over the studied period (1996–2005). The trend line shows an overall decrease in the number of human trichinellosis cases.
Clinical symptoms are given in Table 3. The course of the disease was registered as follows: unspecified in 187 cases (38.0%), moderately severe in 164 cases (33.3%), benign in 121 cases (24.6%), severe in 18 cases (3.7%), and complicated by myocarditis in 2 cases (0.4%).
Listed terms are not mutually exclusive.
The following laboratory test results were extracted from the patients' files: eosinophil counts (16.3 ± 14.3, range: 0–78%) (Table 4), leukocyte counts (7802.6 ± 3444, range: 1500–38,000 cells/mm3), and erythrocyte sedimentation rate (ESR) (14.7 ± 13.8, range: 0–105 mm/h). In 374 patients (76.0%) the leukocyte counts were within normal limits (less than 10,000 cells/mm3) and 81 patients (16.5%) had values ranging between 10,000 and 20,000 cells/mm3, whereas more than 20,000 cells/mm3 were found in 3 patients (0.6%). The leukocyte count values were not specified in the medical records of 34 cases (6.9%). ESR was within normal ranges (0–10 mm/h) in 191 patients (38.8%), 103 patients (20.9%) had values between 11 and 20 mm/h, and 75 patients (15.2%) had values over 20 mm/h. The ESR values were not specified in 123 cases (25.0%).
Therapy administered included an antiparasitic drug alone in 310 cases (63.0%), a corticosteroid alone in 4 cases (0.8%), and a combination of the two aforementioned drugs in 147 cases (29.9%). Neither antiparasitic drugs nor corticotherapy was indicated in 31 cases (6.3%). Of the patients undergoing a specific antiparasitic treatment, 9 (2.0%) were treated with albendazole, 105 (23.0%) received mebendazole, 329 (72.0%) received thiabendazole, and 14 (3.0%) were treated with piperazine.
Discussion
The epidemiology and epizootology of trichinellosis in Jiu Valley was extensively studied over the years by Cristea and collaborators, and therefore, the statistical database is very complex. The first human focus of trichinellosis was officially recorded in 1965 in the town of Aninoasa (Fig. 1). Trichinellosis cases occurred again after 20 years. The highest number of human cases (n = 571) was recorded in 1991, a year of economic transition from socialism to capitalism in Romania. Consequently, Jiu Valley became a hyperendemic area for trichinellosis, situated on the first position in Romania and even in Europe. Data collected over a 20-year period (1987–2006) indicated an annual average incidence of 71.7 human cases per 100,000 inhabitants (totally 2524 cases distributed in 799 foci). Further, the postmortem examinations performed between 1993 and 1996 on 170 deceased bodies of individuals who had never been diagnosed with trichinellosis while alive showed a rate of infection of 27.1%. Therefore, the real incidence of disease was much higher than the figures reported by the official authorities. The prevalence in animals was as follows: 1.94% in pigs (201,650 examined animals during 1988–2002), 41.5% in rats (492 animals examined during 1992–1994), 36.5% in stray dogs (148 animals examined during 1992–1993), 22.58% in wild boars (31 animals examined during 1991–1996), and 31.25% in foxes (16 animals examined during 1992–1996) (Cristea, 1998; Olteanu et al., 1999; Cristea et al., 2005, 2006).
The data available for the metallurgic region surrounding the town of Hunedoara are rather poor, indicating 0.08% prevalence of trichinellosis in pigs (509,797 animals examined during 1998–2002) (Cristea et al., 2003).
This study showed that women were predominantly affected (55.1%), which is in accordance with national statistic data from different periods of time: 54% of cases diagnosed with trichinellosis before 1970 were women and the figures increased to 67% after 1992–1993 (Ionescu, 1995). Urban inhabitants were the most affected category (77.0%), similar to cases from Timis County (70.45%) (Neghina et al., 2009a). The same distribution was found in national epidemiological studies indicating an urbanization of the disease despite the fact that the source of infection (pork) originated in the rural areas. Thus, 60% of the patients came from urban regions in 1987, and during 1991–1993 there was an increase up to almost 90% (Ionescu, 1995). Unsurprisingly, winter was the season when most of the cases (64.2%) were diagnosed, followed by spring (22.6%). Pigs are usually slaughtered during the winter months and the traditional (raw or undercooked) products are largely consumed mainly on special occasions such as Christmas and New Year's Eve, but also later in the months of the spring season. Data reported by two other studies performed in the neighborhood counties show the same seasonal distribution pattern: Timis County, 81.0% in winter, followed by 11.13% in spring; and Arad County, 71.6% in winter, followed by 26.3% in spring. Traditional homemade pork dishes usually include raw/smoked sausages, blood pudding, mosaic salami, salted ham, and bacon (Neghina et al., 2009a, 2009c). The length of hospital stay ranged between 8 and 14 days (10.1 ± 1.8) in most of the cases (47.8%), similar to Timis (52.02%) and Arad (46.0%) counties. Patients aged 40–49 years required the longest hospital stay (9.7 ± 4.3 days, range: 4–20), whereas cases aged 0–9 years were hospitalized for the shortest period of time (7.7 ± 2.7 days, range: 3–15). It was reported that Hunedoara County had the highest unemployment rate (10.9%) in Romania in 2004 (Badulescu, 2006). A lot of people lost their jobs when the unproductive grand metallurgic factories and coal mines were closed down. Therefore, they began to rely on cheap food sources for most of their diet. Pigs were raised in unsanitary conditions in a close proximity with rodents, and unverified pork was illegally traded on a large scale. Hence, most of the patients who acquired the disease were unemployed (40.1%), of whom many individuals belonged to the gipsy minority with unsafe food habits (e.g., consumption of dead pig corpse).
The most frequent symptom was myalgia, similar to other studies (Jansen et al., 2008; Neghina et al., 2009a). An interesting fact was that 17.1% of the patients were asymptomatic. They were hospitalized and found to be infected only because of positive history of ingestion of infected meat. The moderately severe course of disease predominated (33.3%), similar to the results reported for the neighborhood counties: 33.97% in Timis and 56.1% in Arad (Neghina et al., 2009a, 2009c). Cases complicated with myocarditis had the highest values of leukocyte counts (16,950 ± 9687.4, range: 10,100–23,800) and eosinophil counts (37 ± 12.7, range: 28–46) when compared with those with benign course who had the lowest values (leukocyte counts: 6600 ± 2273.6, range: 2800–17,000, p = 0.027, Mann–Whitney U test; eosinophil counts: 10.4 ± 8, range: 0–38, p = 0.020, Mann–Whitney U test).
Thiabendazole was the specific antiparasitic drug administered in most of the patients (72.0%) because of its wide availability in hospitals. Nevertheless, the guidelines do not recommend this drug because of its multiple side effects (Dupouy-Camet and Bruschi, 2007). The hospitalization period was shorter for patients who were treated with mebendazole alone (7.1 ± 2.8 days, range: 2–17) when compared with those treated with albendazole alone (11.3 ± 4.6 days, range: 6–21, p = 0.001, Mann–Whitney U test) and thiabendazole alone (9.1 ± 3.6 days, range: 3–25, p = 0.000, Mann–Whitney U test), respectively. In patients who received corticosteroid-associated therapy, mebendazole proved as the most efficient antihelmintic drug—the mean hospitalization period was 8.3 ± 2.7 days (range: 2–17), but not significantly different from thiabendazole (9.5 ± 3.9, range: 3–25, p = 0.263, Mann–Whitney U test). Those who received albendazole in combination with corticotherapy required a significantly longer period of hospital stay (11.2 ± 2.7 days, range: 10–16, p = 0.016, Mann–Whitney U test).
Conclusions
For a long period of time, trichinellosis represented a serious public health and ecological concern in Hunedoara County because of the favorable social, economic, cultural, and geographic conditions of this territory. In the past endemic years, the massive confiscation of infected pork, prolonged sick leave granted to the affected laborers, and high morbidity and mortality rates in humans led to huge economic losses and negative psychological effects on population. An important role in the spread of the disease was played by the lack of specific crematoria for destruction of the infected meat. The infected meat is usually thrown by the owners into waste containers for home clean-out or at the periphery of localities where it is ingested by rats and stray dogs. Trichinellosis became endemic because of the following reasons: ignorance of basic safety rules (trichinelloscopic examination of the meat was performed only sporadically), lack of information about the malady and its consequences, and different food habits of a population having roots in various parts of the country (Cristea, 1998).
In this study, despite rich history, an overall decrease in the number of human trichinellosis cases over the 10-year study period (Fig. 2) was revealed and the decline might have been favored by the following positive aspects: improvement of sanitary conditions, implementation of a more reliable collaboration between veterinarians and pig breeders/consumers, education of the population by general practitioners, and a more careful supervision of the veterinary and human public health services.
Footnotes
Acknowledgment
The authors express their gratitude to Mirela Mititelu for collecting the data from the Hospital of Infectious Disease in Vulcan.
Disclosure Statement
No competing financial interests exist.