
Abstract
Shiga toxin–producing Escherichia coli (STEC) infections are an important cause of foodborne disease in Australia. Three percent to 7% of sporadic patients develop hemolytic uremic syndrome (HUS) and 40% of patients with HUS develop chronic complications. To examine costs associated with illness, we interviewed patients notified to the South Australian Department of Health with a structured questionnaire regarding severity of illness, medical treatment, time lost from work, hospitalization, and other costs. In 2003–2006, we interviewed 46 patients of STEC infection, 2 of whom developed HUS. The median duration of illness was 7 days (range 3–31 days) and 41% (19/46) of patients were admitted to hospital. The estimated total cost for the 46 STEC cases in South Australia was AUD$144,087, equating to a mean cost of AUD$3132 per case. We estimate that the annual total costs of STEC infection in South Australia and Australia are AUD$200,283 and AUD$2,633,181, respectively. We used linear regression to identify that STEC infection costs increase by AUD$608 per day regardless of severity, and that more severe illness is strong predictor of cost. This is the first Australian study to examine costs of STEC infection and highlights the significant impact of this illness.
Introduction
In 1995, one Australian State—South Australia—experienced a serious outbreak of 23 cases of pediatric HUS as a result of mettwurst contaminated with E. coli O111:nm- (Cameron et al., 1995). After this, South Australian pathology laboratories referred all stool specimens containing macroscopic blood to a reference laboratory for screening using polymerase chain reaction tests to identify the presence of STEC toxin genes (Combs et al., 2005). Consequently, surveillance for STEC infection in South Australia is more complete than for other Australian States (The OzFoodNet Working Group, 2007). The incidence of STEC infection in South Australia in 2006 was 2.4 patients per 100,000 population, compared to 0.4 per 100,000 population for all of Australia combined (The OzFoodNet Working Group, 2007). Even with the screening of stool specimens that occur in South Australia, there will still be significant underreporting because people with mild disease are unlikely to seek treatment or be investigated. In South Australia, an estimated 8.15 (95% credible interval 3.30–75.14 cases) STEC infections occur in the community for every case notified to the Department of Health (Hall et al., 2008).
STEC can cause severe illness and long-term sequelae, resulting in social and economic cost to the community and the health system (Tarr et al., 2005; Mead and Griffin, 1998). However, little is known about the costs of STEC infection in Australia. Economic costs are key drivers for public health decision makers to develop strategies for preventing infections and improving surveillance. The aim of this study was to determine costs due to STEC infection in South Australia from a societal perspective using actual patient experience, and extrapolate these costs to all of Australia.
Methods
We conducted interviews with patients of sporadic STEC infection in South Australia from July 2003 to August 2006. Eligible participants were South Australian patients recruited for a national case–control study of STEC who agreed to be contacted again for this study (McPherson et al., 2009). South Australian Department of Health staff conducted telephone interviews of participants using a semistructured questionnaire inquiring about the clinical illness, hospitalization, treatment, and expenses due to the illness.
Cost determinations
The questionnaire captured self-reported costs to STEC patients or their carer for each of several categories (Table 1) within direct costs (medical and medication) and indirect costs (productivity loss, transport, and other consumer costs). We calculated mean costs per category using all cases as the denominator. We also stratified patients into four categories of severity: (1) patients who attended a general practitioner (GP) only, (2) patients who visited hospital emergency but were not admitted, (3) patients admitted to hospital, and (4) HUS patients. Mean costs were calculated for each severity category. For patients admitted to hospital, we used recognized diagnosis-related groups (DRG) for patients with gastroenteritis that assign a total hospital cost (Department of Health and Ageing, 2006a, 2006b, 2006c). A second measure of hospital costs was also derived based on the average daily cost for the DRG multiplied by the number of days each patient reported being in hospital (DRG per day method). This allowed for a more accurate assessment of STEC cases that may be more severe than other gastroenteritis cases that contribute to the DRG and was the preferred measure. Costs were determined for the 2004–2005 financial year in Australian dollars.
DRG, diagnosis-related groups; GP, general practitioner; MBS, Medicare Benefits Scheme; PCR, polymerase chain reaction; STEC, Shiga toxin–producing Escherichia coli.
Costs for South Australia and Australia
To approximate the total cost of STEC infection in South Australia, the total number of notifications of STEC was distributed across the four severity categories from this costing study. We assumed that for every STEC infection reported to a health department there were 8.15 non-notified cases occurring in the community (Hall et al., 2008). Costs for non-notified cases were estimated as 70% of the mildest severity category—those who only visited a GP because we assumed that the majority of these would have visited a GP but not had a specimen taken. The 70% is an approximation based on the probability of visiting a doctor for gastroenteritis (Hall et al., 2008) and the high proportion of STEC cases that report blood in the stool (McPherson et al., 2009). These were then totaled and added to costs for notified cases to arrive at an annual cost of STEC infections in South Australia. To calculate the cost of STEC infections in Australia, we applied the rate of notified and estimated rate of non-notified cases in South Australia to the Australian population (Australian Bureau of Statistics, 2006). A sensitivity analysis was conducted for total South Australian and Australian costs to allow for both DRG methods, direct costs only, the non-notifiable fraction credible intervals, and costing assumptions.
Data management and analysis
Completed questionnaires were entered onto a Microsoft Access™ database and Microsoft Excel ™ was used to analyze basic costs of STEC infection. We used STATA Intercooled version 8.2 (Stata Corp., College Station, TX) to generate 95% confidence intervals (95% CI) of costs using bootstrapping with 100 iterations, with correction for any resulting bias. We used STATA to conduct linear regression to examine the significance of duration of diarrhea and severity of illness in predicting cost. Where cases had missing values, we applied the mean value for the appropriate category.
The South Australian Department of Health ethics committee approved the conduct of the study.
Results
There were 46 STEC patients recruited into the study, comprising 73% of those from South Australia recruited into the national case–control study during the costing study period. Of these, 19 were O157, 12 were non-O157, and 14 were unable to be further serogrouped. Study participants comprised 29 males and 17 females, ranging in age from 1 to 94 years. The median duration of illness for all patients was 7 days (mean 11 days; range 3–31 days). Two female patients aged 3 and 4 years old were found to have HUS.
Direct costs
STEC patients visited a range of facilities for medical treatment, with some patients visiting multiple facilities. Figure 1 shows a flow chart of GP, emergency, and hospital utilization for all cases that contribute to direct cost calculations shown in Table 2. Direct costs were estimated as $1860 (95% CI $1042–$2664) per case and comprised 74% of total costs when using the DRG method. In contrast, the direct cost per case was estimated as $2501 (95% CI $1429–$3395) when using the DRG per day method, comprising 79% of costs.
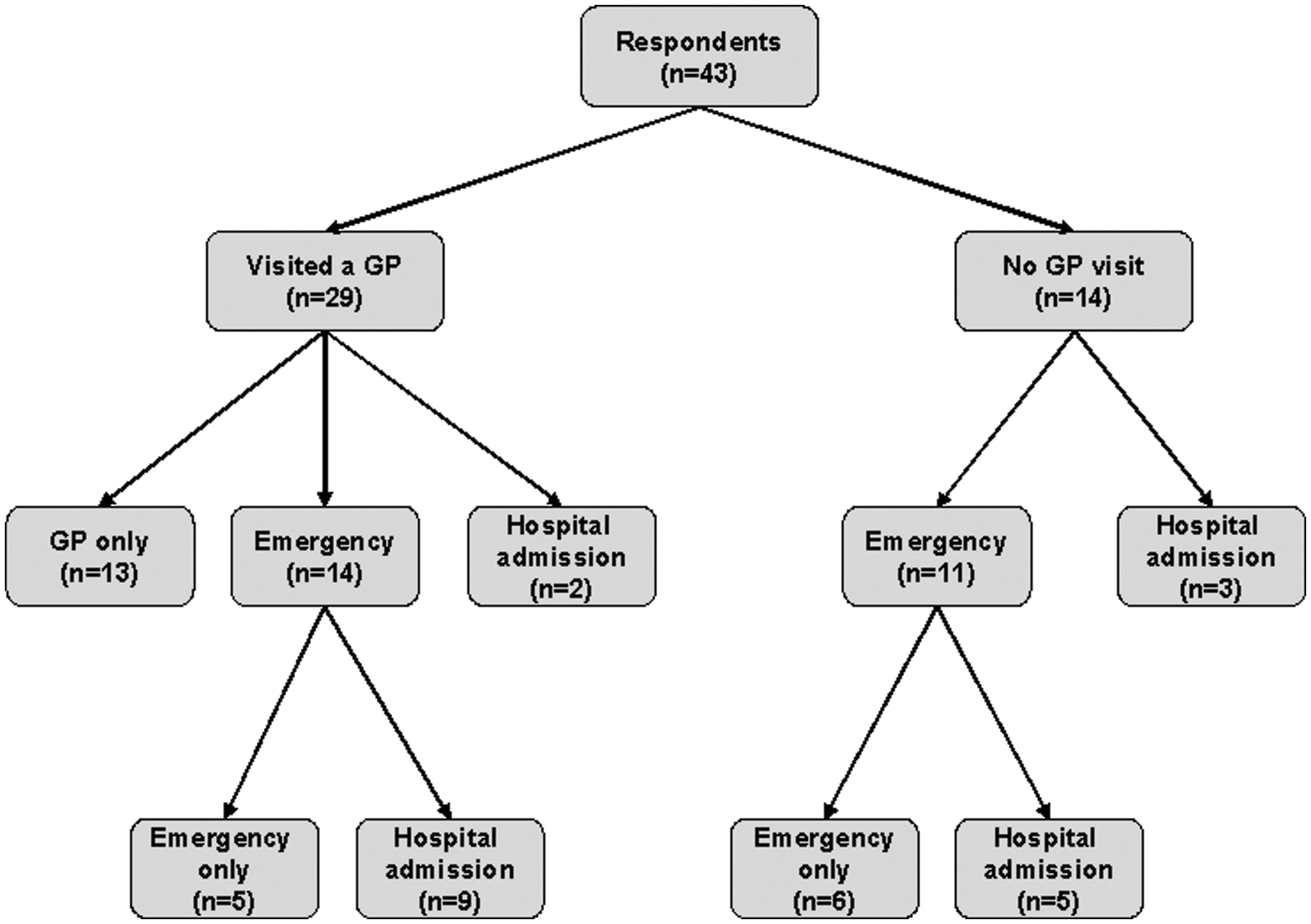
Flow chart of GP and emergency department visits and hospital admission for respondents in Shiga toxin–producing Escherichia coli costing study, South Australia, 2003–2006.
All cases were costed an additional $35 for PCR testing.
CI, confidence interval.
Medical costs
Two-thirds of patients (n = 29) attended a GP for their illness for a total of 68 visits (mean 1.5; range 1–10). Of these patients, 13 were treated by the GP only, 14 also visited an emergency department with 9 being admitted to hospital, and 2 patients were admitted to hospital without an emergency visit. Of the 29 patients who reported visiting a GP, 17 were bulk billed with the remainder paying some out of pocket expense. The mean of the reported cost per case was $52 (95% CI $41–$67) (Table 2).
Sixteen patients reported having a pathology test as a result of their GP visit. Seven reported a blood test (one case reported having three), six reported a stool test (one case reported having two), and three reported both a blood and stool test. Of the patients who reported a stool test, one also reported having an X-ray; of those that reported a blood test, one also reported urine test. As well as these 25 tests, all cases were costed an additional $35 for polymerase chain reaction testing for STEC. The mean cost for pathology tests per case was estimated as $66 (95% CI $53–$79).
Hospital emergency
Twenty-five patients visited emergency departments and as one case visited 3 times, the total number of emergency visits was 27. The mean cost of emergency visits per case was $214 (95% CI $162–$273).
Hospital admissions
Nineteen patients reported admission to hospital for a total 109 nights in hospital, with a median stay of 4 nights (range 1–12 nights). The two HUS patients were both admitted to intensive care.
Using the DRG costing method, the mean hospital cost per case was estimated as $1492 (95% CI $800–$2454), which represented 59% of the total cost when this method was used (Table 2). Using the DRG per day costing method, the mean hospital admission cost was estimated as $2132 (95% CI $1142–$3386) and this represented 68% of the total cost of STEC illness when this method was used.
Medications
Fourteen patients reported that they received 17 prescriptions of antibiotics; one reported being prescribed two different antibiotics and another three. The mean cost was estimated as $10 per case for antibiotics (95% CI $5–$17). Twenty-five patients reported using other prescription medication, including 18 taking antidiarrheal medication, 3 antinausea, and 13 anticramp medications, giving an estimated mean cost of $16 per case (95% CI $12–$20). Thirty-two patients reported taking over-the-counter medications, with an estimated mean cost of $11 per case (95% CI $8–$14).
Indirect and other costs
Indirect costs, comprising productivity loss, transport, and other reported costs, represented 11% of the estimated total cost of STEC illness based on DRG per day method, with a mean cost of $349 (95% CI $259–$492) per case (Table 2).
Productivity loss
Fifteen patients reported productivity loss as a result of their STEC illness, with a total of 230 days missed from paid work (mean 5 days). The mean productivity loss per case was $164 (95% CI $89–$291) (Table 2). Twenty patients reported that a carer or another family member missed work as a result of a caring for a case with STEC infection, giving a total of 108 days missed from work (mean 2 days). The mean productivity loss for carers per case was $185 (95% CI $93–$317). Seven respondents reported that both the case and a carer or family member missed work during the patients' illness.
Transport
Thirty-seven patients reported using a private car, two public transport, and three a taxi to travel to medical appointments. Estimated distance traveled in private cars totaled 7360 km (mean 165; range 1–3600 km) and the estimated mean cost was $99 (95% CI $32–$166). A total of $208 miscellaneous other transport costs (excluding ambulance) were also reported.
Nine patients reported transport by ambulance for an estimated total of 1238 km, giving a mean of 27 km/case (range 3–159 km). This included two patients who required transportation by flight, for 155 and 772 km, respectively. The mean ambulance cost was estimated as $117 (95% CI $48–$296).
Other costs
Respondents reported other consumer costs, such as accommodation and travel of visitors, extra food, nappies and drinks, telephone calls, car park fees, and costs associated with delaying holidays. The mean cost per case was reported to be $67 (95% CI $34–$163).
Total costs
The total cost for the 46 STEC cases in South Australia was estimated as $114,611 using the DRG method for hospitalizations, and $144,087 using the DRG per day method. This equates to a mean cost of $2492 (95% CI $1,718–$4,270) and $3132 (95% CI $1827–$4149) per case, respectively (Table 2).
Costs by severity of illness
The mean costs per severity category are shown in Table 3. Hospital costs comprised the majority of total estimated costs in the two HUS cases. The two HUS cases (category 4) had higher estimated GP and hospital costs, but lower estimated GP tests and medication costs, the latter probably due to these being provided (and costed) in the hospital setting. HUS cases also reported higher productivity losses, transport, and other costs.
Severity categories: 1, patients who attended a GP only; 2, patients who visited hospital emergency but were not admitted; 3, patients admitted to hospital; 4, HUS patients.
HUS, hemolytic uremic syndrome.
Total costs for South Australia and Australia
During 2003–2006, there were 141 notified cases of STEC infections in South Australia. We estimate that a further 1149 cases may have occurred in the community but were not reported. This gives an estimated incidence rate of STEC in South Australia of 21 patients per 100,000 population per year, which includes non-notified patients. Extrapolating this incidence rate to the Australian population gives a total 4240 estimated patients for the same period. Annually, STEC infections in South Australia and Australia cost the community an estimated $200,283 (95% CI 154,500–264,545) and $2,633,181 (95% CI 2,031,263–3,478,060), respectively, with direct costs for STEC infections costing $137,761 (95% CI 101,312–177,247) in South Australia and $1,811,183 (95% CI 1,331,986–2,330,318) in Australia (Table 4).
Lower and upper bound from credible interval of notifiable fraction of 8.15 (3.3–75.1).
Lower bound assumed that 20% of non-notifiable patients attended doctors as per national gastroenteritis study for all pathogens (Hall et al., 2008) and upper bound assumed that 90% of non-notifiable patients attended doctors.
When adjusting these costing estimates for the credible intervals around the non-notifiable fraction, the total cost of STEC in South Australia ranged from $153,453 to $860,894 and for Australia from $2,017,256 to $11,317,126. When the cost for non-notifiable cases is taken as 20% of severity category 1, then the overall costs of STEC in South Australia becomes $141,354 and for Australia becomes $1,858,418.
Multivariate modeling of cost
Age, sex, location, duration of illness, and severity category were included in a linear regression model with DRG costs per day as the outcome (Table 5). We imput the mean severity category of two for four patients where severity of illness was not recorded, along with a mean duration of 4.9 days illness for four patients where information was missing. Age, sex, and location of patients had no effect on the cost of illness. Costs of illness for patients with categories 3 and 4 severity of illness were significantly different from the reference category. Treatment costs for patients increased by $608 per day, regardless of severity. The constant term in the model was large and negative, and including interaction terms did not improve model performance.
Interaction terms were included in several other models without changing the results and therefore are not shown.
Severity categories: 1, patients who attended a GP only; 2, patients who visited hospital emergency but were not admitted; 3, patients admitted to hospital; 4, HUS patients.
p ≤ 0.05.
Discussion
This is the first study to estimate the costs of STEC infections in Australia, which found that this illness cost approximately AUD$2.6 million each year. In South Australia alone, the annual cost was estimated at AUD$200,283. Cost for STEC in Australia could be as high as AUD$11.3 million when the upper bound of the credible interval for the non-notifiable fraction for STEC is used. Direct costs, comprising medical and medication costs, for STEC illness were estimated as AUD$1.8 million each year. These costs are high given that STEC infection is uncommon in Australia, with 73 cases reported in 2006 (The OzFoodNet Working Group, 2007). Also, that the DRG per day method was AUD$29,476 higher than the DRG method suggests that STEC is a more serious disease requiring higher hospital costs than other gastrointestinal infections included in this DRG, such as campylobacteriosis. In our study of 46 cases, STEC infection resulted in very mild symptoms requiring one GP visit, through to a severe illness leading to admission to intensive care. The median duration of illness for STEC patients was 7 days and two patients developed HUS.
The cost item that contributed most to the total cost using both the DRG and DRG per day method for hospitalizations was that for hospital admissions, at 66% and 72%, respectively. Other costs comprised <8% of total costs each. Cases of HUS cost significantly more than non-HUS cases. Despite this, the costs measured in our study are likely an underestimate due to the fact that there were only two case patients with HUS both of whom had not required dialysis, developed end-stage renal disease (ESRD), or required a kidney transplant at the time of interview, all which can occur following STEC infection (Tarr et al., 2005).
It is difficult to make international comparisons for cost of illness studies because of variations in definitions of costs and their measurements and the differences in the level and distribution of income across countries. A costing study completed in the United States for E. coli O157 infections in USD$ from 2003 used a similar methodology to this study, although a final severity category was included that costed reduced lifetime employment losses, lifetime medical costs, and premature deaths as a result of ESRD. However, for those severity categories where ESRD was not relevant, the costs were comparable, bearing in mind the differences between the two countries in terms of health systems and exchange rates. Of the 73,480 annual cases in the United States, 78% did not visit a doctor and were costed at $26 per case, 19% visited a doctor but did not go to hospital and these were costed at $441 per case, and 3% were admitted to hospital and those that did not get HUS were costed at $5599 per case for those with HUS the cost was $30998 per case (Frenzen et al., 2005). Like this study, the conclusion was that the principal cost of illness was related to the severity of patients' illness.
This study estimated the costs of STEC illness in Australia from a societal perspective. It included costs to all parties combined and did not split them into payees. It is likely our study provides an underestimate of total cost due to STEC in Australia, as the study design did not allow for reporting of long-term sequelae such as complications as a result of HUS, permanent disability, premature death, lost leisure time, and pain and suffering. An Australia study estimated that the cost of illness and premature mortality due to HUS alone was AUD$2.5 million a year (Abelson et al., 2006) and an American study estimates monetized quality of life costs including pain and suffering and reduced life expectancy at US$1399 per case of E. coli O157:H7 (Scharff, 2010). This study did not attempt to estimate these costs as the study design focused on patient report at time of diagnosis. In addition, we have not estimated government and industry costs, such as product recalls, regulatory and public health surveillance costs, outbreak control and prevention, and research. However, as our assumptions were based on reported experiences from patient interview, and not from assumed experiences, the costs we derived were indicative for the categories we were able to assess.
There were several limitations to this study. All data were self-reported and subject to recall bias, including the number of GP visits and medication taken, and some data were missing or poorly recorded. Nonhospital medical, laboratory, and medication costs were inferred from self-report by the case or carer and not from medical records. The hospital, GP, laboratory, and medication costs were estimated from information provided by commonwealth health data and may not represent real costs. As there is no specific DRG for STEC infection, we attempted to account for this by calculating DRG per day. Despite these limitations, this study was based on actual costs experienced by STEC cases and suggests that this uncommon illness bears significant costs in Australia.
Footnotes
Acknowledgments
We thank the study participants and their families for participating in this study. The Australian Government Department of Health and Ageing funded this study under the OzFoodNet program of work.
Disclosure Statement
No competing financial interests exist.