
Abstract
Objectives:
The main objectives of this study were to establish baseline characteristics for milkborne outbreaks, establish an expected milkborne outbreak profile, and identify potential indicators of food terrorism.
Materials:
This study used 1990–2006 data from the Centers for Disease Control and Prevention Annual Listings of Disease Outbreaks and the Foodborne Outbreak Database (FOOD) to establish epidemiologic baseline characteristics for disease outbreaks associated with fluid milk. FOOD data from 2007 were used to qualitatively validate the potential of the baseline characteristics and the expected outbreak profile.
Results:
Eighty-three fluid milkborne outbreaks were reported between 1990 and 2006, resulting in 3621 illnesses. The mean number of illnesses per outbreak was 43.6 (illness range: 2–1644). Consumption of unpasteurized milk was associated with 55.4% of reported outbreaks. Campylobacter spp., Escherichia coli, and Salmonella spp. caused 51.2%, 10.8%, and 9.6% of reported outbreaks, respectively. Private homes accounted for 41.0% of outbreak locations. Number ill, outbreak location, and etiology were the primary characteristics which could signal a potential intentional contamination event. In 2007, one pasteurized milk outbreak caused by Listeria was flagged as aberrative compared with the expected outbreak profile.
Conclusions:
The creation and dissemination of expected outbreak profiles and epidemiologic baseline characteristics allow public health and Homeland Security officials to quickly assess the potential of intentional food contamination. A faster public health and medical system response can result in decreased morbidity and mortality.
Introduction
Unintentional and intentional outbreaks can be detected through multiple routes, including healthcare provider report, laboratory-based surveillance, active and passive public health surveillance, consumer complaint, and epidemiologic analysis of public health surveillance data (Sobel et al., 2002a; CIFOR, 2009). Initial outbreak investigation and epidemiologic response activities are similar, regardless of outbreak intentionality. However, epidemiological characteristics of intentional contamination events may quickly fall outside expected, or normal, outbreak profiles because of contaminant lethality, food system contamination location, and degree of product distribution.
Early detection of intentional contamination events can mitigate negative public health and economic consequences (Khan et al., 2001; Sobel et al., 2002b; Ashford et al., 2003; Danzig, 2003; CIFOR, 2009). Rapid detection of these events can reduce the number of exposed individuals via contaminated product removal from retail and food service outlets, public notification and education, and a more timely dissemination of preventative and therapeutic measures to exposed individuals (Halliday et al., 1991; Hedberg, 2005; CIFOR, 2009). Reduced exposures to foodborne pathogens/contaminants and enhanced therapeutic efficacy directly translate into decreased morbidity/mortality and associated economic losses (Wein and Lui, 2005; CIFOR, 2009; Hartnet et al., 2009). Aberrative foodborne outbreak characteristics potentially signal an intentional contamination event. Identifying and characterizing these signals constitutes one approach for an early event detection methodology. Unfortunately, research concerning such signals or indicators is lacking, especially in the context of food defense.
In the absence of prior intelligence, differentiating outbreak intentionality requires the establishment of epidemiologic baseline characteristics related to particular food vehicles, such as fluid milk. Once established, these characteristics can be utilized in three ways. First, epidemiologists can use baseline outbreak characteristics as outbreak detection thresholds to facilitate early outbreak recognition. Second, the identification of the most common aggregated outbreak characteristics can provide an expected outbreak profile, thus providing a reference from which to identify anomalous outbreak behavior. Third, infectious disease and bioterrorism preparedness modeling can incorporate these outbreak characteristics, and subsequent outbreak detection signals, into prediction modeling and risk mitigation studies.
These efforts will build upon previous milkborne outbreak reports and research (Ryan et al., 1987; Hennessy et al., 1996; Headrick et al., 1998; Wein and Lui, 2005; CDC, 2009; LeJeune and Rajala-Schultz, 2009). The inclusion of both pasteurized and unpasteurized milkborne outbreaks, given the differences in processing requirements, distribution networks, and consumption patterns, is required to establish adequate epidemiologic baselines for food defense purposes. The main objectives of this study are to establish baseline characteristics for all milkborne outbreaks, establish an expected profile of milkborne outbreaks, and identify potential indicators of a food terrorism incident.
Materials and Methods
State, local, territorial, and tribal health departments voluntarily report outbreak data to the Centers for Disease Control and Prevention (CDC, 2010). Outbreak data reported to CDC for 1990–1997 are available in the Annual Listings of Disease Outbreaks and 1998–2007 data are available in the Foodborne Outbreak Database (FOOD) (CDC, 2009).
A combination of data from the 1990–1997 Annual Listing of Disease Outbreaks and the 1998–2006 FOOD data was used in this analysis. These data consist of the following variables: year, month, number ill, etiology (Salmonella, Escherichia coli, Norovirus, etc.), location (house, school, camp, etc.), state, and vehicle (milk, chicken, spinach, etc). Fluid milk outbreaks were identified by analyzing the vehicle variable for any indication of being solely caused by fluid milk. If such indication was identified, outbreak vehicles were deemed to be fluid milk. These outbreaks were then stratified according to the following categories: pasteurized milk, unpasteurized milk, chocolate-pasteurized milk, chocolate-unpasteurized milk, and unpasteurized goat milk. Nonmammalian fluid milk products, such as rice milk, were excluded from the analysis. Bacterial etiologies were categorized based on genus. If an outbreak was determined to have >1 etiology, it was recoded as “multiple etiologies” and was excluded from etiology-specific analyses. For outbreak location, all variations of home or private residence were recoded in the “private home” category. All variations of restaurant or delicatessen were recoded into one category. Outbreaks were recoded as “multiple locations” if more than one location was indicated.
Descriptive statistics were calculated for all variables. Frequencies were calculated for categorical variables; means and standard deviation (SDs) were calculated for continuous variables. t-Tests were used to compare differences between continuous variables and χ 2 tests were used to compare differences between categorical variables. Analysis of variance methods were used to assess the relationships between continuous dependent variables and categorical independent variables. The expected outbreak profile was created using the most common values for location, etiology, pasteurization status of the implicated milk, and the 17-year aggregate morbidity estimates. The potential indicators of an intentional contamination event were created using the least common values for location, etiology, and pasteurization status. A derivation of the CDC Early Aberration Reporting System C1-3 algorithm test statistic, and its traditional cutoff value of 3, was used to calculate an outbreak trigger based on outbreak size (Zhu et al., 2005).
FOOD milkborne outbreaks from 2007 were used to qualitatively validate the potential of the expected outbreak profile to indicate aberrative outbreak values. SAS® version 9.2 was used for all data analyses and Microsoft Excel® was used for all graphical purposes.
Results
Between 1990 and 2006 there were 83 reported fluid milkborne outbreaks, representing 0.5% of all reported foodborne outbreaks (n = 15,720) during this period. The total number of reported annual foodborne outbreaks ranged from 413 to 1413 during the study period. The majority of all milkborne outbreaks (n = 50; 60%) during 1990–2006 have occurred since 2000. Outbreaks due to unpasteurized milk account for 55% (n = 46) of total milkborne outbreaks during this period.
The number of unpasteurized milkborne outbreaks has increased in recent years (Fig. 1). When comparing the pasteurization status of outbreaks during the periods of 1990–1998 and 1999–2006, there were significantly more unpasteurized milk outbreaks in the latter period (p-value < 0.01). Outbreak stratification by month did not reveal seasonal patterns.
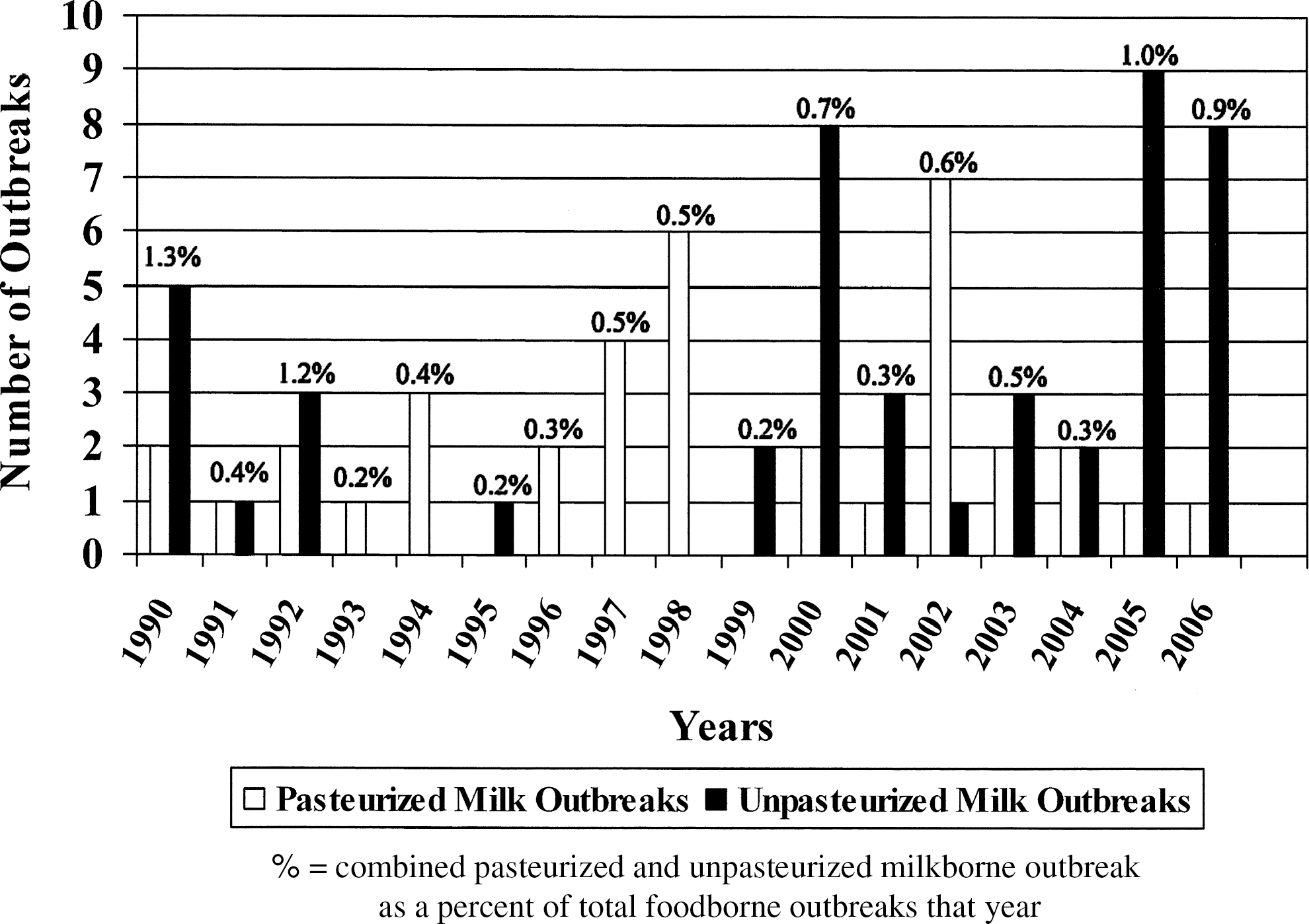
Pasteurization status of milkborne outbreaks from 1990 to 2006.
Few organisms account for reported milkborne outbreak etiology. Campylobacter was the most common etiologic agent, causing 51.2% of all milkborne outbreaks and 69.0% of all milkborne illnesses (Table 1). When assessing outbreaks with known etiologies (n = 63), Campylobacter caused 66.7% of milkborne outbreaks. E. coli and Salmonella caused 10.8% and 9.6% of all milkborne outbreaks, respectively. Campylobacter caused significantly more unpasteurized milk outbreaks compared with pasteurized milk outbreaks (67.4% vs. 29.7%, respectively; p < 0.01).
Multiple locations.
Milkborne outbreaks occurred in relatively few settings. Private homes accounted for the largest location category, representing 41.0% of all reported outbreak locations (Table 2). Stratifications of milk type and location category identified differing patterns in milk outbreak locations. The most common locations for pasteurized milk outbreaks were private homes (27.6%) and restaurants (17.2%). The most common location category for unpasteurized milk outbreaks was private homes (60.5%). Of note, the majority of pasteurized chocolate milk outbreaks (75%) occurred in schools. There were significantly more unpasteurized milk outbreaks (compared with pasteurized milk outbreaks) in private homes compared with other outbreak locations (p-value < 0.01). The “private home” category was also the most common location of milkborne outbreaks for the majority of pasteurization status/etiology combinations (Table 1).
Does not sum to 100 because of rounding.
In total, the 83 reported milkborne outbreaks resulted in 3621 illnesses. The mean number of illnesses per outbreak was 43.6 with a SD of 181.6. The median number of illnesses per outbreak was 11.0, and the mode was 2.0. Mean illnesses per milkborne outbreak were not statistically different from nonmilk foodborne outbreaks (mean = 24.7). The mean number of illnesses per pasteurized milk outbreak (71.5) was not statistically different from unpasteurized milk outbreaks (21.2). Of note, the large morbidity (n = 1644) associated with one pasteurized milk outbreak contributed 45.4% of all illnesses associated with outbreaks included in this study. Excluding this outbreak reduces the mean number of illnesses per milkborne outbreak (24.1) and the mean number of illnesses per pasteurized milk outbreak (27.2).
Outbreak triggers, based on morbidity values, are derived by solving an adaptation of the CDC Early Aberration Reporting System C1-3 algorithms. Substituting the values from the 17-year baseline characteristic analysis (mean = 43.6 illnesses and SD = 181.6) and using the test statistic cutoff value of 2, an outbreak consisting of ≥588 illnesses would trigger an outbreak alert. Exclusion of the large outbreak, mentioned in the preceding paragraph, yields a smaller outbreak trigger (>135 illnesses). These values, along with the least common location and etiology categories, contribute to potential intentional contamination event indicators in Table 3. The most common etiology, location, and pasteurization status categories contributed to the expected milkborne outbreak profile (Table 3).
Excludes morbidity from one large outbreak (n = 1644).
Mean + 1 standard deviation.
Mean + 2 standard deviations.
Potentially indicates multiple, temporally linked contamination events.
In 2007, six fluid milk outbreaks were reported and are used here for qualitative validation purposes. Campylobacter was the sole etiologic agent in four of these outbreaks and was identified as one of two etiologic agents in a fifth outbreak. The average number of illnesses per outbreak was 6.5 (SD = 5.83), with no outbreak reporting >18 cases. Five of these outbreaks were due to unpasteurized milk, and the majority (83.3%) occurred in private homes. One pasteurized milk outbreak would be identified as aberrative when compared with the expected outbreak profile. The etiologic agent was Listeria, which falls within the “outbreak etiology” potential indicator category.
Discussion
A deeper understanding of milkborne outbreak epidemiology, the establishment of outbreak baseline characteristics, and the creation of an expected milkborne outbreak profile are important efforts to bolster both food safety and defense. Milkborne outbreaks are relatively uncommon events, with the majority being caused by three etiologic agents and occurring in a limited number of location categories. As with all foodborne outbreaks, the morbidity related to milkborne outbreaks exhibits large variability.
The main limitation of this study is imperfect surveillance system completeness of detection, reporting, and attribution of foodborne diseases. Foodborne illness surveillance systems capture a small percentage of the true foodborne illness incidence (CIFOR, 2009). Of note, Oliver et al. (2009) identified milkborne outbreaks, which occurred during the study period and were not included in the FOOD database. Attribution of foodborne illness to particular food vehicles can be problematic (Batz et al., 2005). Although attribution issues and underreporting may lead to a less-detailed analysis of the expected outbreak profile and baseline characteristics, the use of 17 years of foodborne outbreak data may mitigate this limitation. As food safety and food defense research continues, better attribution methods and practices, combined with the utilization of multiple outbreak data sources, are warranted.
When qualitatively validating the expected outbreak profile, most of the fluid milk outbreaks occurring in 2007 exhibited expected values. The majority of these outbreaks were due to the consumption of unpasteurized milk, caused by Campylobacter, occurred in private homes, and resulted in relatively few illnesses. One pasteurized milkborne outbreak caused by Listeria, which resulted in three deaths, would have been identified as aberrative.
Public health officials will be able to compare newly identified outbreaks with the expected outbreak profile and the baseline characteristics. Although values and occurrences outside the expected profile may not be pathognomonic for an intentional contamination event, public health officials should note the unusual circumstance. Milkborne outbreaks with etiologic agents that are not Campylobacter, Salmonella, or E. coli are indicative of outbreak characteristics outside of the norm; however, outbreak etiologies of Listeria monocytogenes, Staphylococcus aureus, and Yersinia enterocolitica, although rare, have been reported (Dalton et al., 1997; Oliver et al., 2005).
Conclusions
In the context of food defense, these results are beneficial in terms of public health preparedness and response. The preparedness aspect is informed by providing important epidemiologic information to public health and intentional contamination prediction modeling. The response aspect is informed by allowing public health officials to quickly compare newly identified outbreaks with the expected outbreak profile. The application of this methodology to other common food vehicles, and the subsequent creation of a library of expected outbreak profiles and potential intentional contamination indicators, would benefit food defense efforts. The further quantification and combination of these outbreak profile characteristics may inform future intentional contamination detection algorithms.
Footnotes
Acknowledgments
This research was supported in part by the National Center for Food Protection and Defense, University of Minnesota, and DHS (Grant No. 2007-ST-061-000003).
Disclosure Statement
No competing financial interests exist.