
Abstract
Background:
Salmonella enterica serotype Enteritidis is a universally recognized cause of foodborne disease. In South Africa, outbreaks of foodborne disease are generally under reported. We investigated the etiology of acute gastroenteritis in 216 patients who presented to a rural hospital in KwaZulu-Natal, South Africa, after consuming a meal at a school function.
Materials and Methods:
Stool specimens from 37 patients, as well as two food samples, were available for microbiological investigation. Similarity between isolates was investigated using phenotypic and genotypic techniques. Phenotypic investigations included morphological, biochemical, and antibiogram profiling. Genotypic relatedness was determined with pulsed-field gel electrophoresis analysis. The available epidemiological data were also described.
Results:
Salmonella Enteritidis was isolated from 18 patients and 1 food sample. Isolates were phenotypically and genotypically indistinguishable. Epidemiological data suggest a point-source outbreak with a possibility of continued transmission.
Conclusions:
The results suggest a foodborne Salmonella Enteritidis outbreak due to contaminated food served at the school function. Epidemiological investigations continue to be extremely difficult in rural areas.
Introduction
The incidence of foodborne infection with Salmonella Enteritidis has increased significantly in the last 25 years, and this organism is now considered an emerging pathogen (
Although foodborne disease outbreaks are common in South Africa, literature reporting this is scanty (Dickson, 1970; Benade, 1996; Karas et al., 2001; Keddy and Koornhof, 2001; Smith et al., 2007). Recent surveillance reports from South Africa document Salmonella enterica serotypes Typhimurium and Enteritidis as the two most frequently isolated Salmonella serotypes. The reports, however, do not stratify the isolates into those obtained from individual patients and those implicated in outbreaks (GERMS-SA, 2008). The Public Health Laboratory in the KwaZulu-Natal Province (KZN) occasionally receives food samples collected by public health officials, but outbreak investigations are not routinely performed (L. Taylor, pers. comm., December 2008).
On the 3 December 2008, a primary school in the Mpungose tribal area in rural KZN held its year-end function. The function was attended by teachers, pupils, parents, and members of the community. Over a period of 10 days after the function, 216 people presented with gastroenteritis to the local Nkonjeni Hospital. We report on an outbreak of foodborne disease after this school function.
Materials and Methods
Epidemiology
A case was defined as any person who consumed food served at the function or leftover food from the function, and presented to Nkonjeni Hospital with signs and symptoms of gastroenteritis from 3 to 17 December 2008. The infection control nurse at the hospital prepared and updated the case list on a daily basis.
Patient records of the cases were audited and the following details extracted: age, sex, clinical presentation, management, and laboratory results.
Public health and environmental health investigations
The district Environmental Health Department was notified by the hospital infection control nurse of the possibility of a foodborne disease outbreak. The investigation included interviews and collection of available food samples.
Clinical microbiology investigations
Local laboratory at Nkonjeni Hospital
Stool specimens obtained from patients were initially processed at the laboratory at Nkonjeni Hospital for primary isolation of foodborne pathogens (York and Rodrigues-Wong, 2003). Isolates were identified by means of the API 20E kit (bioMérieux, Marcy-I'Etoile, France).
Referral laboratory
All stool specimens collected at Nkonjeni Hospital were transported to the laboratory in Durban. These were again processed for the detection of foodborne pathogens using standard operating procedures (York and Rodrigues-Wong, 2003). Bacterial identification and susceptibility testing was performed with the VITEK 2 instrument (bioMérieux). The microbroth dilution method (CLSI, 2008) was used to determine and interpret the minimum inhibitory concentrations for the following antimicrobials: ampicillin, ciprofloxacin, ceftriaxone, chloramphenicol, and meropenem (Sigma-Aldrich).
Pulsed-field gel electrophoresis (PFGE) was performed to determine genetic relatedness among the isolates according to the standard PulseNet protocol, using the XbaI restriction enzyme (Swaminathan et al., 2001; Ribot et al., 2006). PFGE profiles were interpreted according to criteria recommended by Barrett et al (2006) and Tenover et al. (1995).
Results
Epidemiological description of the outbreak
Two hundred and sixteen cases presented to the local hospital with signs and symptoms of gastroenteritis over a 10-day period. Figure 1 illustrates the number of new cases that presented on a daily basis to the hospital. The majority (37%) presented on day 2. Clinical records of 115 (53%) were available for auditing. Record keeping was haphazard and essential information was often omitted. Sex, clinical history, and presentation were not recorded in the majority of cases. Age was available for 95% (109) of patients. The average age was 17.56 years with a mean of 16 years (range: 7 months–73 years). Antimicrobial treatment was administered to 105/115 (91%) cases. Most cases (83%) received a combination of metronidazole and trimethoprim/sulfamethoxazole. Other antibiotics prescribed included ampicillin (18%), ceftriaxone (14%), amoxicillin (3%), erythromycin (1%), and ciprofloxacin (1%).
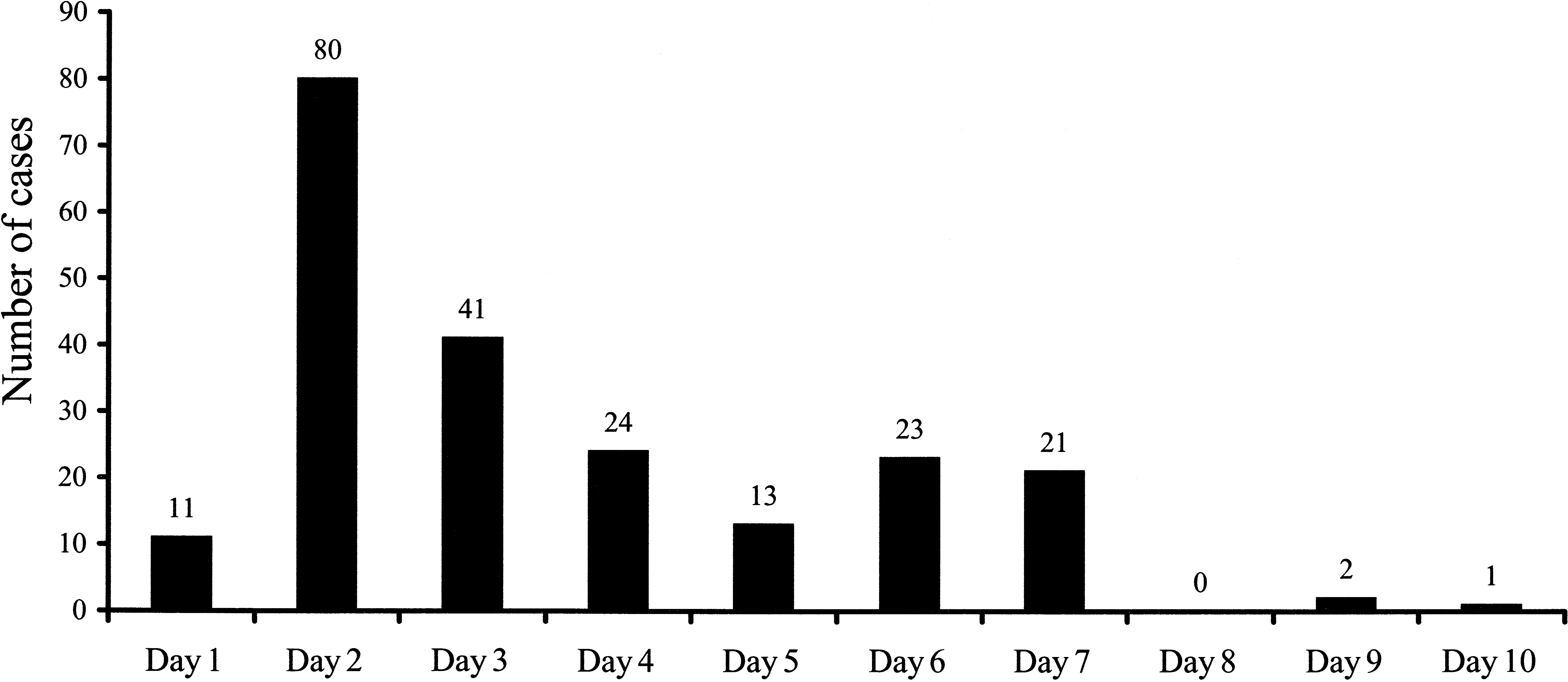
Number of cases that presented each day to Nkonjeni Hospital (meal was served on day 0).
Public health investigation
Cases and other function attendees were interviewed. The lunch that was served at the school function comprised of the following dishes: beef stew, fried chicken, rice, beetroot salad, coleslaw, kidney bean salad, baked beans, pumpkin, chakalaka (a traditional relish consisting of spiced tomato, onion, and beans), fruit juice, sliced tinned tomatoes, pineapple, canned peaches, and ice cream. The fried chicken and beetroot salad were prepared on the previous day at the house of one of the teachers. All other food was prepared on the school premises on the day of the function. Left-over food was distributed to members of the community, and two food samples were obtained from the home freezer of a teacher. The food was stored in two containers: one was a composite sample of the main meal containing a mixture of cabbage, rice, beans, butternut, and some form of meat; the second contained a mixture of dessert. Salmonella species was isolated from the composite main meal food sample. The dessert sample yielded no pathogens.
Microbiological investigations
Stool specimens were only available for 37 cases. During primary investigations at the Nkonjeni Hospital laboratory, Salmonella species was isolated from the stool of four cases. However, at the referral laboratory Salmonella species was isolated from the stool of 18 patients.
The 18 clinical isolates and the 1 isolate from the composite food sample were fully susceptible to all antimicrobials tested. Extended-spectrum β-lactamases were not detected. Isolates were serotyped (Remel, Kent, United Kingdom) according to the Kauffmann-White scheme as Salmonella Enteritidis (O:1,9,12 H:g,m;1). PFGE analysis showed that the DNA banding patterns for 17 of the clinical isolates and the one food isolate were indistinguishable. However, the banding pattern of one of the clinical isolates differed by more than six bands from the other isolates and is therefore not considered to be part of this outbreak cohort (Fig. 2). PFGE analysis was repeated, which confirmed this result.
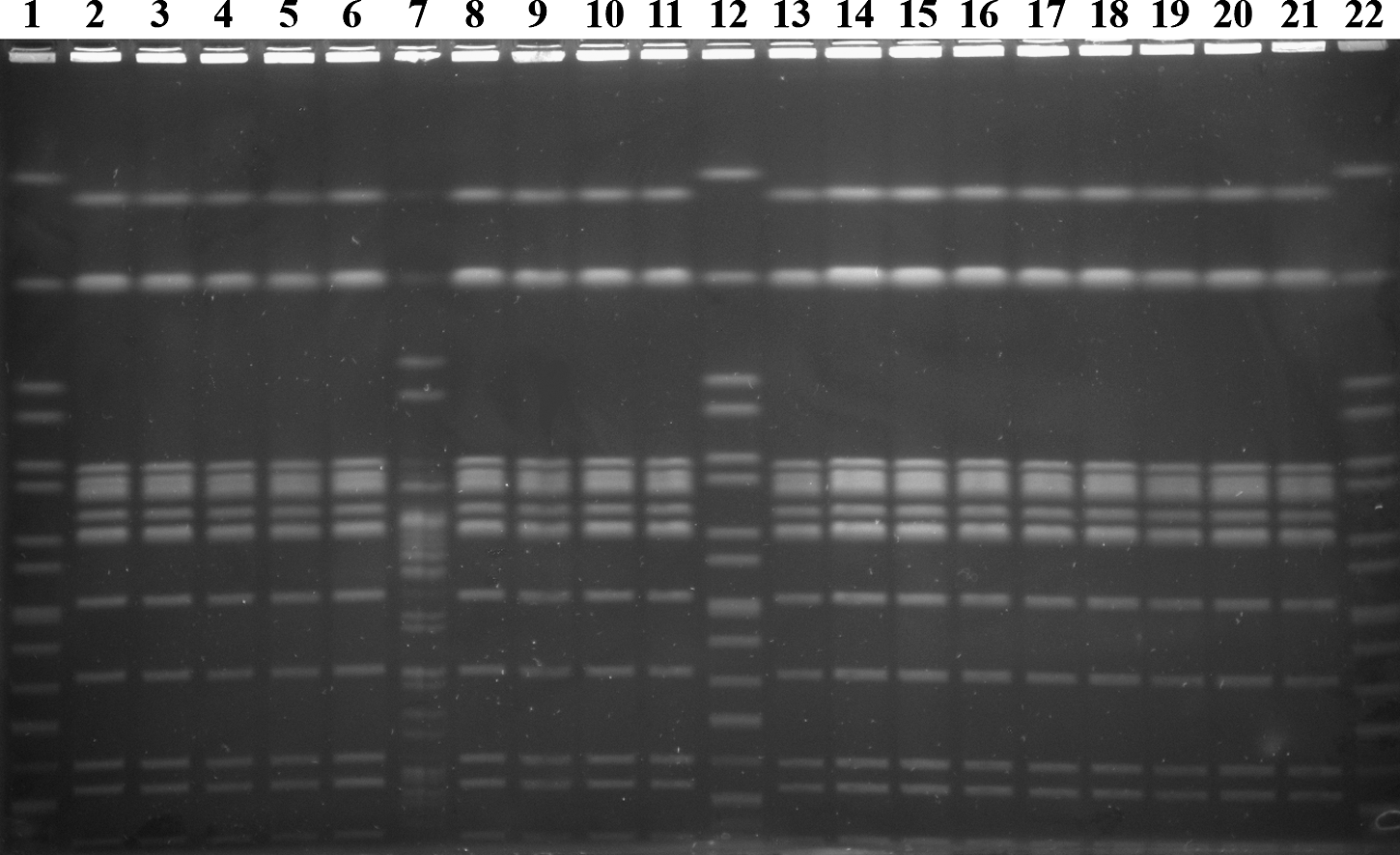
Pulsed-field gel electrophoresis patterns (from left to right) of Salmonella Braenderup (strain H9812) reference standard in lane 1, Salmonella Enteritidis clinical isolates in lanes 2–11, Salmonella Braenderup reference standard in lane 12, Salmonella Enteritidis clinical isolates in lanes 13–20, Salmonella Enteritidis food isolate in lane 21, and Salmonella Braenderup reference standard in lane 22. The banding pattern of clinical isolate in lane 7 differed by more than six bands from the other isolates and is therefore not considered to be part of this outbreak cohort.
Discussion
Epidemiological and laboratory evidence points to Salmonella Enteritidis as the cause of gastroenteritis following the consumption of food at a school function. The exact vehicle of transmission of the organism could not be elucidated as the food sample sent to the laboratory consisted of a mixture of the main course.
As in most areas in rural South Africa, the people of the Mpungose tribal area live under socio-economically deprived conditions. Basic infrastructure, including sanitation, clean water, and electricity, is largely unavailable or unaffordable. This is compounded by the paucity of public health awareness regarding food safety practices. Food is often prepared well in advance of a function and stored inappropriately due to lack of refrigeration facilities. Sharing of leftover food occurs frequently after functions. Here again, leftover food is not stored under optimal conditions and may not be adequately reheated before consumption.
The reported incubation period for Salmonella Enteritidis is 6 to 48 h, and occasionally up to 4 days (WHO, 2008). Here we report that patients presented to the hospital with gastroenteritis between 1 and 10 days after the school function (Fig. 1). This may not necessarily reflect a longer incubation period of the disease, but may be attributed to the continued transmission from left-over food that was consumed after the school function. Since the clinical records did not contain details regarding the timing of the onset of symptoms, the average incubation period could not be determined. Earlier reporting with appropriate intervention could have altered the course of this outbreak and decreased morbidity.
Although foodborne disease outbreaks are common in South Africa, they are under-reported. Health-care authorities are often alerted late in the course of an outbreak, negating the impact of timely, comprehensive, epidemiological investigations (Dickson, 1970; Benade, 1996; Karas et al., 2001; Keddy and Koornhof, 2001; Smith et al., 2007). Three outbreaks of foodborne gastroenteritis that occurred in 2008 in the Ulundi Municipality were not further investigated. One of these outbreaks involved 38 high school children who consumed beef soup and porridge that was left at room temperature for 24 h (C. Mbatha, pers. comm., December 2008).
In first-world settings, molecular subtyping is an essential part of the investigation of infectious diseases outbreaks (Swaminathan et al., 2001; Sodha et al., 2009). To offer value in the early identification and management of an outbreak, molecular subtyping has to be rapid with comparable results between laboratories. PulseNet, the national molecular subtyping network for foodborne bacterial disease surveillance in the United States, developed and standardized a PFGE protocol to be used for the rapid subtyping of common foodborne pathogens (Ribot et al., 2006). In this report, PFGE analysis of isolates was performed in retrospect and did not impact on outcome. PFGE revealed a unique banding pattern for one of the clinical isolates, suggesting that this patient may not have been linked to the outbreak cohort. Although this result was confirmed, it was not further investigated using other restriction enzymes due to cost constraints. In addition, from an outbreak investigation perspective, the causative organism was already identified.
Antibiotic resistance among Salmonella species has been described in KZN previously (Govinden et al., 2008). Our laboratories therefore routinely perform antimicrobial susceptibility tests on clinically significant Salmonella isolates. The outbreak strain was susceptible to all antimicrobials tested. Foodborne salmonellosis is often self-limiting, and it is therefore debatable whether the administration of antibiotics to patients during this outbreak was indicated. The paucity of clinical information available in this study unfortunately prevents further evaluation regarding the use of antimicrobial agents. However, 105/115 (91%) of cases received antibiotics and this underscores the importance of educating the local medical community regarding the appropriate use of antimicrobials in the management of diarrhea.
The epidemiological investigation of this outbreak was hindered by a multitude of factors, including a delay in reporting. The school function heralded the close of school for the Christmas holidays. Since the first case presented 24 h after this, many children and teachers had already left the area and were unavailable for interviews. Local culture dictates that school functions are not restricted and anyone from the community may attend. There was therefore no formal guest list, and this, coupled with the fact that leftover food was taken away and consumed by others in the community, made case finding difficult.
Requests for laboratory investigations were at the discretion of the attending physicians. In addition, an undetermined number of stool specimens were thrown out by the Nkonjeni Hospital laboratory. We were therefore only able to locate 37 refrigerated stool specimens for further investigation at the referral laboratory. Laboratory investigations at the local laboratory were restricted due to the lack of essential media and reagents, including selenite F broth and xylose-lysine-desoxycholate agar plates. The technologists therefore omitted the usual stool enrichment step, and directly inoculated normal MacConkey agar plates. This is most likely why the yield of the outbreak strain from the referral laboratory was significantly higher than the local laboratory.
The Environmental Health and Public Health investigation was also hindered. Although the food specimens were collected 2 days after the school function, it only arrived at the KZN Public Health Laboratory 6 days after collection. The food samples were not flagged as being part of an outbreak investigation and were not prioritized but processed as routine.
Investigations of outbreaks are extremely difficult in rural KZN. Health-care workers are heavily reliant on the microbiology laboratory for guidance. There are no efficient lines of reporting of outbreaks resulting in delays in investigation. A rapid and efficient molecular approach to outbreak detection and investigation might have important practical relevance, especially in rural South Africa, where foodborne disease outbreaks frequently occur. Community health education campaigns targeting the handling, preparation, and storage of food is also essential to help curb these outbreaks.
Authors' Contributions
Abraham J. Niehaus was responsible for conducting laboratory investigations, data collection, data analysis, and the writing of the article. Prashini Moodley was in charge of the outbreak investigation and assisted with the writing of the article. Teke Apalata assisted with the initial outbreak investigation. Yacoob M. Coovadia assisted with the initial laboratory investigations. Anthony M. Smith carried out the PFGE and helped with the preparation of the article. All authors have read and approved the final article.
Footnotes
Acknowledgments
The authors would like to thank Sis Cynthia Mbatha from Nkonjeni District Hospital for her invaluable assistance during the initial outbreak investigation. The authors would also like to thank Rita Balakistan from the Microbiology Laboratory, Inkosi Albert Luthuli Central Hospital, Durban, for her help with the initial investigation of the stool specimens. The authors would also like to thank Logan Pillay for his assistance with the microbroth dilution MIC assay and the staff from the Public Health Laboratory in Durban for their help with the investigation of the food specimens and the serotyping of isolates.
Disclosure Statement
No competing financial interests exist.