
Abstract
Foodborne infections are an important public health problem in China. In 2008, we conducted surveillance for laboratory-confirmed nontyphoidal Salmonella to monitor trends for this infection in China and to build capacity for rapid detection and response to foodborne outbreaks. Salmonella isolates from patients with diarrhea were sent from hospitals to local public health laboratories for confirmation, serotyping, and antimicrobial susceptibility testing. A total of 126 hospitals in 44 cities and counties from 8 provinces provided isolates and epidemiologic data for analysis. Of 23,140 stool specimens submitted to clinical laboratories, 662 (3%) grew Salmonella enterica. Salmonella were most commonly detected between April and October. The median age of infected patients was 27 years; 34% of infections occurred in patients <5 years old. Of the 662 isolates, we found 73 serotypes, of which serotype Enteritidis (31%) and serotype Typhimurium (26%) were the most common. The prevalence of resistance was high for clinically important antimicrobial agents, including ampicillin (41%) and ciprofloxacin (6%). More than 60% of isolates, including 35% of all Typhimurium, were resistant to three or more antimicrobial agents. In this first multiprovince surveillance report of laboratory-confirmed Salmonella infections in China, we found that Enteritidis and Typhimurium are the most common serotypes and that efforts to reduce antimicrobial resistance among Salmonella in China are needed. Although no outbreaks were detected using this system, efforts to improve this system's capacity to do so are underway.
Introduction
B
China has an Internet-based surveillance system for high priority infectious diseases (Wang et al., 2008). This system collects information about some bacterial infections commonly transmitted by food, but the case reporting categories only include cholera, dysentery, and “other infectious diarrhea,” and the data collected for each of these categories is limited. Patients with salmonellosis should be reported in the “other infectious diarrhea” category with the etiology added as a comment. Few such cases are reported, and reported cases are not required to be laboratory-confirmed. This surveillance system does not collect sub-typing data (Zhang et al., 2009). China, therefore, lacks reliable data about the number of illnesses caused by Salmonella nationally and lacks a system to monitor trends and detect widely dispersed outbreaks of Salmonella in real time.
Since 2001, the World Health Organization Global Foodborne Infections Network (WHO GFN) has supported training of Chinese public health staff in epidemiology, isolation, and sub-typing of enteric bacterial infections, including Salmonella. Building on the capacity of this program, China's Center for Disease Control and Prevention (China CDC) initiated sentinel surveillance for laboratory-confirmed Salmonella in eight provinces in China. We report here the epidemiology, serotypes, and antimicrobial susceptibility of Salmonella in these provinces.
Materials and Methods
Study design
The surveillance was conducted among eight Chinese provinces: Beijing, Chongqing, Fujian, Guangdong, Guangxi, Henan, Shanghai, and Sichuan (estimated total population 400 million persons). Provinces were selected based on their interest and their current public health and clinical capacity to conduct surveillance. Each province chose from 6 to 27 sentinel hospitals to participate. In 2008, 126 hospitals from 44 administrative areas (cities or counties) provided isolates and epidemiologic data for analysis.
Physicians submitted stool samples to clinical laboratories from patients who presented with three or more loose stools within 1 day and had other symptoms such as fever, vomiting, or abdominal pain (CDC, 2004). Clinical laboratories were asked to use a standardized procedure to isolate Salmonella from stool (MOH, 2007). Salmonella isolates were forwarded to the laboratories of local public health authorities (each known as a local CDC), which confirmed, serotyped, and antimicrobial susceptibility tested the isolates. Demographic and clinical information for each laboratory-confirmed case, including age, gender, symptoms, date of illness, and date of specimen collection, was collected and electronically transmitted to China CDC.
Microbiological testing
Laboratories were asked to use the following protocol. Stool samples were enriched in tetrathionate brilliant-green broth or selenite broth for 6–8 hours at 37°C, followed by sub-cultivation onto Hektoen Enteric agar, Salmonella–Shigella agar, or CHROMagar Salmonella agar. The plates were incubated at 37°C for 18–24 hours. Presumptive colonies were screened by tests in triple-sugar-iron agar, motility indol-urea agar, L-lysine decarboxylase, and L-galactosidase (onitrophenyl-L-D-galactopyranoside [ONPG]). One presumptive colony from each sample was stored in semisolid agar and shipped to local CDC laboratories, where presumptive Salmonella isolates were identified by using API 20E test strips (bioMerieux). O and H antigens were characterized by slide agglutination with commercial antiserum (S&A Reagents Lab), and the serotype was assigned according to the Kauffmann-White scheme. Susceptibilities for 12 antimicrobial agents (ampicillin, chloramphenicol, streptomycin, sulfamethoxazole, tetracycline, nalidixic acid, ciprofloxacin, cefotaxime, ceftazidime, cefepime, gentamicin, and trimethoprim) were evaluated by the disk diffusion method (CLSI, 2009) and classified as resistant, intermediate, and susceptible according to Clinical Laboratory Standards Institute guidelines (CLSI, 2010). An isolate was considered resistant to trimethoprim-sulfamethoxazole if it was resistant to both agents. In analyses, we defined “clinically important resistance” as resistance to one or more of the following agents: ampicillin, cefotaxime, ceftazidime, cefpime, ciprofloxacin, gentamicin, and trimethoprim-sulfamethoxazole (Varma et al., 2005). Escherichia coli ATCC 25922 was used for quality control.
During the project, workshops were held among participating provincial CDCs to standardize protocols, review progress, and discuss results. The national reference laboratory for enteric pathogens at China CDC provided ongoing technical support. Microbiological laboratories from the eight provincial CDCs participated in the External Quality Assurance System for Salmonella serotyping and antimicrobial susceptibility testing organized by WHO GFN (Hendriksen et al., 2009).
Data analysis
Data were analyzed using SAS Version 9.1 (SAS Institute). Chi-squared analysis was performed to compare the percentages of antimicrobial resistance in serotypes Enteritidis and Typhimurium. A p-value <0.01 was regarded as statistically significant.
Results
Salmonella surveillance
In 2008, about 23,140 stool specimens were cultured from patients with diarrhea. Only three provinces (Beijing, Shanghai, and Guangxi) recorded the total number of patients with diarrhea that were evaluated at the sentinel hospitals during this period. Of the 39,172 patients with diarrhea evaluated at sentinel hospitals in these three provinces, 9301 (24%) had stool cultured (Table 1). Guangxi had the highest rate of stool culture (37%), followed by Shanghai (22%) and Beijing (13%).
Of the 23,140 specimens cultured in all 8 provinces, 662 (2.7%) grew nontyphoidal Salmonella. The isolation rate ranged from 4.5% (Guangdong) to 0.7% (Chongqing). In general, Salmonella isolation rate was high from April to October (Fig. 1). The absence of isolates from February likely reflects the impact of the Chinese New Year celebration on healthcare utilization and project participation. Obvious increases in Salmonella isolation were noted between April and July in Beijing, Henan, and Guangdong (data not shown). The median age of all patients was 27 years (ranging between 0 and 88 years). Children <5 years accounted for 33.5% (222/662) of the total isolated cases. The overall male/female ratio was 1.22:1.
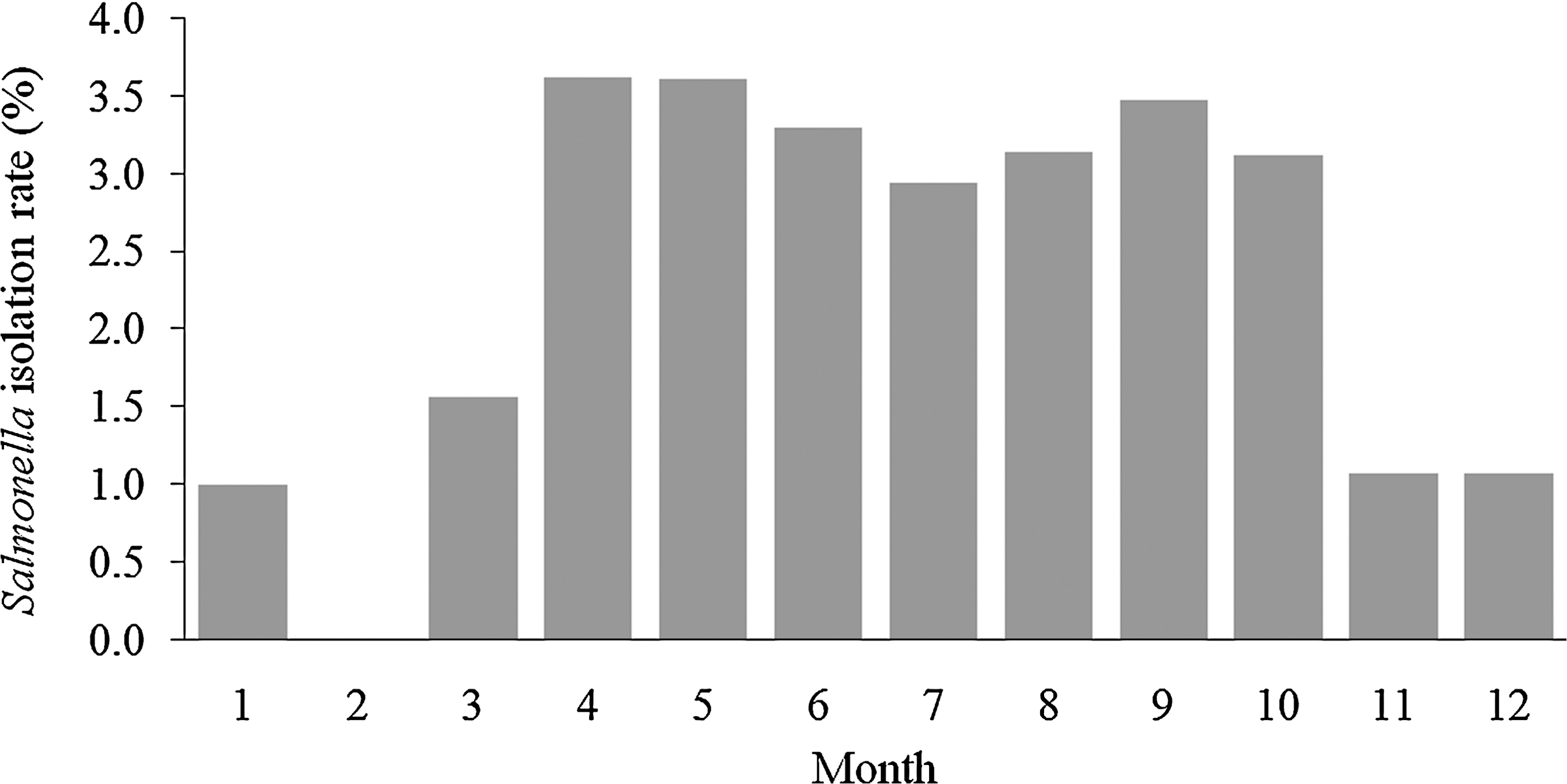
Overall isolation rate for nontyphoidal Salmonella by month in eight provinces in China, 2008.
Serotypes of Salmonella isolates
We found 73 serotypes among the 662 Salmonella isolates, with 10 serotypes accounting for 76.1% (504/662) of all isolates (Table 2). Enteritidis (31.4%) was the most prevalent serotype, followed by Typhimurium (27.3%). A wide variety of serotypes were detected among the remaining 158 isolates. The only province in which serotypes Enteritidis and Typhimurium did not account for more than 50% of isolates was Guangxi. In Guangxi, the 46 Salmonella isolates were distributed among 25 serotypes; Typhimurium (19.2%) and Derby (8.5%) were the most common, and only one Enteritidis was isolated.
Antimicrobial susceptibility
A total of 202 isolates (30.5%) were susceptible to all tested agents. The overall prevalence of resistance to individual antimicrobial agent is summarized in Table 3. Resistance to at least one clinically important antimicrobial agent was found in 66.2% (438/662) of isolates; resistance to three or more clinically important agents was found in 31.9% (211/662) of isolates. A high prevalence of resistance was observed for nalidixic acid (67.8%), sulfamethoxazole (50.4%), tetracycline (42.7%), ampicillin (41.4%), and streptomicin (39.6%). Few isolates were resistant to broad-spectrum cephalosporins, including cefotaxime (4.1%), ceftazidime (2.9%), and cefepime (2.7%). Resistance to ciprofloxacin was observed in 5.6% (37/662) of all isolates. Among 449 nalidixic acid-resistant Salmonella isolates, 30 (6.7%) were also resistant to ciprofloxacin and 73 (16.3%) had intermediate ciprofloxacin resistance.
Clinically important antimicrobials include the following agents: ampicillin, cefotaxime, ceftazidime, cefpime, ciprofloxacin, gentamicin, sulfamethoxazole, and trimethoprim.
Resistance to at least ampicillin, chloramphenicol, streptomycin, sulfamethoxazole, and tetracycline.
We also examined the resistance proportion of Enteritidis and Typhimurium strains, as these were the most prevalent serotypes The proportion of strains with the ACSSuT resistance pattern (defined as resistance to at least ampicillin, chloramphenicol, streptomycin, sulfamethoxazole, and tetracycline) was significantly higher in Typhimurium (35.4%) than in Enteritidis (1.0%) (p < 0.01). Compared with Enteritidis, the proportion of Typhimurium strains that were resistant was also higher for cefotaxime, cefepime, chloramphenicol, tetracycline, streptomycin, gentamicin, and trimethoprim (p < 0.01).
Serotype Typhimurium accounted for 18 (48.7%) of the 37 ciprofloxacin-resistant Salmonella isolates. All ciprofloxacin-resistant Typhimurium isolates were resistant to at least two and up to eight additional antimicrobial agents. Of 18 ciprofloxacin-resistant Typhimurium strains, 12 (66.7%) were isolated in Henan Province. Of 156 Typhimurium strains from provinces other than Henan, 6 (3.8%) were ciprofloxacin-resistant compared with 12 (48.0%) of 25 Typhimurium in Henan Province (p < 0.01). A higher prevalence of multidrug resistance was also observed in isolates from Henan compared with other provinces (data not shown).
Discussion
In this first multiprovince summary of laboratory-confirmed nontyphoidal Salmonella infections in China, we found that the isolation rate was low and variable by season, that the serotype distribution was similar to other countries, and that resistance to clinically important antimicrobial agents was high, particularly for serotype Typhimurium.
In the three provinces that collected data regarding stool culturing practices, only a minority of patients with diarrhea had stool specimens collected and cultured for enteric bacteria. Because physicians in sentinel hospitals were encouraged to collect specimens for this surveillance project, we assume that the rate of stool collection and culturing is even lower in other hospitals. Public health officials overseeing this project have been told by physicians that microbial culture results will not change clinical management for most patients and that patients are unwilling to pay for the cost of testing, factors that have been noted in other countries (Scallan et al., 2006). Physician reluctance to order stool testing may also be related to the low overall yield of cultures for pathogens such as Salmonella.
In this project, the overall isolation rate (2.7%) of Salmonella in diarrhea patients was low when compared with data from studies (Brooks et al., 2006) but similar to what has been seen in routine clinical practice (Slutsker et al., 1997). Many factors can impact the isolation rate, including the severity of clinical illness, antibiotic use before specimen collection, and specimen collection and processing. Low Salmonella isolation rates have also been noted in three other studies reported in China (Qu et al., 2005; Zhang et al., 2008; Zhu et al., 2009). Of note, the marked seasonal variation in isolation, with increases in warmer months, has been observed in other settings (van Pelt et al., 2003; Xia et al., 2009). Although stool culture may not change clinical management for some patients with diarrhea, culture is critically important for public health professionals to monitor the incidence of enteric infections commonly transmitted by food. Further studies are needed to understand factors that can increase physician testing practices and to determine whether the low isolation rates represent true rates of infection or problems in the preanalytic or analytic phases of laboratory testing.
The high proportion of isolates that were Enteritidis and Typhimurium is similar to data from other countries in Asia, Africa, Europe, and Latin America (Humphrey, 2000; Olsen et al., 2001; Herikstad et al., 2002; Bangtrakulnonth et al., 2004; Galanis et al., 2006). Derby is also commonly found in other regions of the world (Galanis et al., 2006; Boyen et al., 2008; Xia et al., 2009), though not as commonly as in Guangxi province. Eggs and chickens are believed to be the major reservoir of Enteritidis (Humphrey, 2000; Guard-Petter, 2001). The large proportion of infections caused by Enteriditis suggests that these food sources should be rigorously investigated when outbreaks of Salmonella occur. Interestingly, data from Salmonella surveillance in foods in China indicate that Derby and Agona are more frequently isolated than Enteritidis and Typhimurium from seven foods: raw pork, raw beef, raw lamb, raw milk, raw seafood, ice cream, and raw vegetables (Wang et al., 2004). Differences in Salmonella serotype distribution between human infection and foods not linked to human illness has also been noted in other studies, indicating that factors other than contamination are important in determining whether humans become ill (Bangtrakulnonth et al., 2004; Galanis et al., 2006). Virulence of Salmonella serotypes is one of these factors, as is food handling and preparation (Jones et al., 2008). Weltevreden only accounted for 2% of Salmonella cases in our study, which contrasts with what is seen in southern Asian countries, such as Thailand, where Weltevreden is one of the most prevalent Salmonella serotypes (Bangtrakulnonth et al., 2004).
We found high rates of resistance to clinically important antimicrobial agents, including multidrug resistance. We found that >2% of isolates were resistant to a broad-spectrum cephalosporin and >5% were resistant to ciprofloxacin, higher than those reported in industrialized countries, but similar to other places in Asia (Su et al., 2004; Weill et al., 2006; Ong et al., 2007; Lee et al., 2009). The worldwide emergence of resistance to antimicrobial agents in Salmonella is an important public health problem (Davis et al., 1999; Su et al., 2004; Wang et al., 2006; Cui et al., 2008; Xia et al., 2009). Resistant Salmonella infections, particularly those with the ACSSuT pattern, have been associated with more severe clinical illness in humans, including a higher rate of bloodstream infections (Helms et al., 2002; Martin et al., 2004). Previous studies have reported that Salmonella isolates resistant to nalidixic acid often have reduced susceptibility to ciprofloxacin, even when these isolates are found to be ciprofloxacin susceptible using the disk diffusion method. Further, fluoroquinolone-susceptible strains of Salmonella that test resistant to nalidixic acid may be associated with clinical failure or delayed response in fluoroquinolone-treated patients with extra-intestinal salmonellosis (Lewin et al., 1991; Hakanen et al., 1999; Szych et al., 2001). In the present study, 6.7% of nalidixic acid-resistant isolates were also resistant to ciprofloxacin and 16.3% showed intermediate resistance to ciprofloxacin, indicating the potential for treatment failure in patients treated with fluoroquinolones. Physicians in China may need to consider the local distribution of antimicrobial resistance when prescribing antimicrobial treatment for patients with Salmonella infection.
The high prevalence of antimicrobial resistance in Salmonella isolates from human infections in China may be associated with many factors. Inappropriate usage of antimicrobial agents to treat humans is a major problem in China (Cao et al., 2004; Liu, 2009; Tacconelli, 2009). A field investigation conducted in Henan Province as part of this project revealed that physicians provide antimicrobial treatment to virtually all patients that complain of diarrhea. Antimicrobial agent usage in food animals is also an important source of drug-resistant Salmonella infection in humans (Hald et al., 2007). Although no published data are available regarding the use of antimicrobial agents in animals in China, the widespread overuse of these drugs in humans suggests a similar problem could be occurring in animals. Data from other countries have shown that usage of fluoroquinolones and other antimicrobial agents in food animal production imposes selective pressure on Salmonella in animals and facilitates transmission of resistant Salmonella to humans through food chain (Cavaco et al., 2007; Cui et al., 2008). Efforts to promote appropriate usage of antimicrobials in both humans and animals and enhance surveillance are essential in China.
Our study is subject to important limitations. First, we did not control the selection of patients, the frequency of testing, or the quality control procedures used in each laboratory. Although efforts were made to standardize all of these, it is likely that some variability across sites can be explained by factors other than disease incidence. Second, we were unable to detect any outbreaks using only laboratory data, and we are unable to use the summary data to calculate incidence. Reasons for this include that we only included a small number of hospitals in each province, and few sites conducted detailed epidemiologic investigation of cases or performed timely molecular sub-typing (e.g., pulsed field gel electrophoresis) to identify case clusters. In the future, expanding surveillance to more health facilities and to more provinces, incorporating rapid molecular sub-typing, and integrating with the international molecular sub-typing network (PulseNet-International) will help to measure incidence and detect outbreaks of human Salmonella infections in China.
Conclusion
This is the first report about the distribution of Salmonella serotypes and antimicrobial resistance collected from health facilities across multiple provinces in China. This surveillance system has highlighted important areas for further public health action in China, including working to increase stool culture and isolation rates, conducting further study into animal reservoirs of Salmonella, and promoting judicious use of antimicrobial agents in humans and animals. More work is needed in the future to determine how this demonstration project can be extended to other parts of China and to enhance the quality, representativeness, and completeness of data.
Footnotes
Acknowledgments
This study was supported by WHO Global Foodborne Infections Network (GFN) and the China–U.S. Collaborative Program on Emerging and Re-Emerging Infectious Diseases, U.S. CDC (5U2GGH000018-02). We are grateful for the participation and excellent work of local CDCs and sentinel hospitals in Beijing, Chongqing, Fujian, Guangdong, Guangxi, Henan, Shanghai, and Sichuan. In addition, we thank the technical experts from WHO GFN, including Jaap Wagenaar (Utrecht University, The Netherlands), Rene Hendriksen (National Food Institute, Denmark), Shaohua Zhao (Food and Drug Administration, USA), Lai-king Ng (Public Health Agency of Canada, Canada), and Matthew Mikoleit and Xin Liu (CDC, USA).
Disclosure Statement
No competing financial interests exist.