
Abstract
The main objective of this study was to develop an understanding of the descriptive epidemiology of foodborne botulism in the context of outbreak detection and food defense. This study used 1993–2008 data from the Centers for Disease Control and Prevention (CDC) Annual Summaries of Notifiable Diseases, 2003–2006 data from the Bacterial Foodborne and Diarrheal Disease National Case Surveillance Annual Reports, and 1993–2008 data from the Annual Listing of Foodborne Disease Outbreaks. Published outbreak investigation reports were identified through a PubMed search of MEDLINE citations for botulism outbreaks. Fifty-eight foodborne botulism outbreaks were reported to CDC between 1993 and 2008. Four hundred sixteen foodborne botulism cases were documented; 205 (49%) were associated with outbreaks. Familial connections and co-hospitalization of initial presenting cases were common in large outbreaks (>5 cases). In these outbreaks, the time from earliest exposure to outbreak recognition varied dramatically (range, 48–216 h). The identification of epidemiologic linkages between foodborne botulism cases is a critical part of diagnostic evaluation and outbreak detection. Investigation of an intentionally contaminated food item with a long shelf life and widespread distribution may be delayed until an astute physician suspects foodborne botulism; suspicion of foodborne botulism occurs more frequently when more than one case is hospitalized concurrently. In an effort to augment national botulism surveillance and antitoxin release systems and to improve food defense and public health preparedness efforts, medical organizations and Homeland Security officials should emphasize the education and training of medical personnel to improve foodborne botulism diagnostic capabilities to recognize single foodborne botulism cases and to look for epidemiologic linkages between suspected cases.
Introduction
C
While there is debate regarding the feasibility of perpetrators to obtain sufficient quantities of the agent, most scenarios that have considered the intentional use of botulinum toxin as a bioterrorism weapon have focused on the aerosolization of toxin in a crowded space, or the release of toxin into a mass-produced, locally distributed food item (Arnon et al., 2001; Wein and Lui, 2005; Institute of Medicine, 2006). Both of these scenarios would produce a large, geographically clustered outbreak of acute paralytic disease that would rapidly overwhelm available health care resources, forcing recognition of the outbreak and an immediate public health response.
In contrast, intentional contamination of a widely distributed and/or long shelf-life food item could cause a large number of illnesses that may lack temporal and spatial clustering. These characteristics could delay recognition of the outbreak and the public health response needed to identify the source. While there are important differences in the surveillance systems for botulism and other foodborne pathogens, recent multi-state outbreaks of E. coli O157:H7 and salmonellosis may serve as models for both this type of distributed outbreak and the public health challenges in outbreak detection, investigation, and remediation (CDC, 2006a, 2007a,b, 2009, 2011a,b). Rapid recognition of foodborne botulism outbreaks is crucial and allows for decreased morbidity and mortality through the prevention of additional cases and early administration of effective treatment and antitoxin (Tacket et al., 1984; Shapiro et al., 1998). The objective of this study is to gain a better understanding of how the descriptive epidemiology of foodborne botulism (i.e., the distribution of cases by person, place and time) may inform the likelihood and timing of outbreak detection in the context of food defense and public health response planning efforts.
Methods
Data on reported cases and outbreaks of botulism in the United States, compiled in CDC's annual Summaries of Notifiable Diseases (1993–2008), Bacterial Foodborne and Diarrheal Disease National Case Surveillance Annual Reports (2003–2006), and Annual Listing of Foodborne Disease Outbreaks (1993–2008), have been reviewed (CDC, 2010b, 2011c–e). Data abstracted from these sources were as follows: year of report, state in which report occurred, and number of affected individuals. An outbreak was defined as two or more cases of botulism caused by consuming a common source-contaminated food. Outbreak detection was defined as clinical suspicion of botulism in two or more cases with a possible link or connection. Locally and regionally distributed foods were defined as food items that were produced and/or distributed within a home, business, neighborhood, or metropolitan area. Widely distributed foods were defined as food items that were produced and/or distributed beyond metropolitan areas.
Published outbreak investigation reports were identified through a PubMed search of MEDLINE citations for botulism outbreaks. Search results were limited to outbreaks occurring in the United States between 1993 and 2008. An in-depth review of large outbreaks (>5 people), with confirmed etiology, informed our analyses related to familial connection of outbreak cases, hospitalization of cases, outbreak recognition methods, median incubation times, outbreak detection time, and distribution characteristics of the contaminated food.
Statistical analysis
SAS® version 9.2 was used for all data analysis, and Microsoft Excel® was used for all graphing purposes.
Results
From 1993 to 2008, 416 cases of foodborne botulism and 58 foodborne outbreaks of botulism were reported in the United States. The number of foodborne botulism cases per year was 16–50, with a median of 24. The number of outbreaks per year ranged from 1 to 8, with a median of 4. The size of the foodborne outbreaks ranged from 2 to 23 persons, with a median of 2. Only six large outbreaks (10%) occurred, with Clostridium botulinum being the confirmed etiologic agent in five of these outbreaks. Altogether, 205 cases (49%) were associated with outbreaks. The number of sporadic botulism cases per year ranged from 5 to 22, with a median of 15. Table 1 provides an aggregated cross tabulation for the number of reported foodborne botulism cases in a state during a year and the status of outbreak reporting in a state during a year. The occurrence of >10 foodborne botulism cases reported in a given state in the absence of a recognized outbreak was rare and occurred only once.
Two multistate outbreaks were not included.
An in-depth analysis of large outbreaks (representing 31% of all cases associated with outbreaks) revealed three potential signals, or trends, for outbreak detection (Table 2). First, the majority of these outbreaks (n=3; 60%) included familial connections within the initial presenting cases. Second, 60% of the outbreaks were recognized when the initial cases were co-hospitalized. Third, the time from earliest botulism exposure to outbreak detection was dramatically longer for widely distributed foods in this sample of botulism outbreaks (Fig. 1).
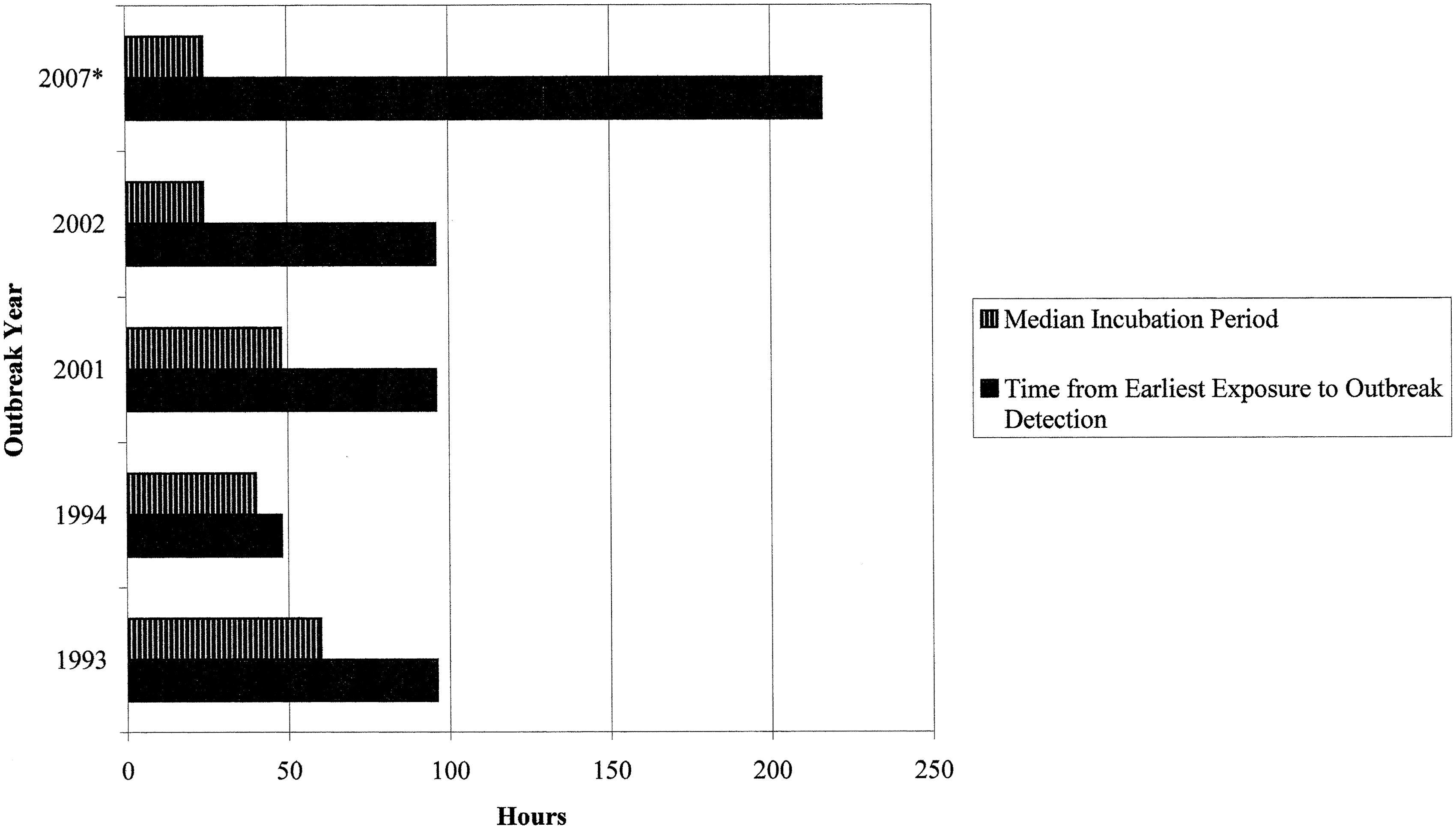
Time characteristics for foodborne botulism outbreaks (>5 people), United States 1993–2008. *Widely distributed food item.
Due to lack of detailed reporting, values are rounded to the next 24 h.
Toxin Type E. All other outbreaks were caused by Toxin Type A.
Further description of outbreaks involving locally and/or regionally distributed food items
Approximately one-third of foodborne botulism cases (125 cases; 30% of total) and one-half of foodborne botulism outbreaks (28 outbreaks; 48% of total) occurred among residents of Alaska. The median size for Alaskan outbreaks was two persons (range, 2–8). These outbreaks primarily occurred among Alaska Natives living in small villages and eating fermented foods (CDC, 2001; McLaughlin et al., 2004; Fagan et al., 2011). These outbreaks are typically recognized because of the occurrence of multiple illnesses among persons with a common exposure. For example, from July 13 to 15, 2002, 14 persons ate raw blubber and skin from the carcass of a beached whale that had been discovered on July 12. The outbreak was reported to public health officials on July 17 by a physician who linked three suspected clinical illnesses with the common exposure. Upon outbreak notification, the Alaska Department of Health and Social Services initiated active case-finding. Of the 14 individuals, eight were confirmed cases, five were hospitalized, four received antitoxin, and two required mechanical ventilation. Four individuals had mild illness and were not treated with antitoxin. The median incubation period was 24 h (McLaughlin et al., 2004).
Outside of Alaska, detection of botulism outbreaks has also been facilitated by linking multiple suspected clinical illnesses to a common exposure. The facilitation of outbreak detection via these epidemiologic linkages is highlighted by the other four large confirmed botulism outbreaks (Townes et al., 1996; Kalluri et al., 2003; Angulo et al., 1998; CDC, 2007c). An outbreak associated with commercial cheese sauce served in a delicatessen in Georgia was identified after the occurrence of multiple symptoms, including difficulty swallowing, in a mother and daughter led to the suspicion of botulism on October 5, 1993. As a result of this initial suspicion, two other cases were identified the next day in patients who had initially received other diagnoses (Townes et al., 1996). Through active case finding and a media campaign, eight people were identified and met the foodborne botulism case definition. Five people were hospitalized and 1 person died. Four hospitalized cases received initial diagnoses other than botulism. All of the cases ate at the delicatessen on October 1. The median incubation period was 2.5 days.
On April 10, 1994, a father and teen-aged son presented at a Texas hospital with acute signs and symptoms of botulism (Angulo et al., 1998). The physician notified public health officials that the only recent meal they had in common was at a local restaurant. Within hours, the local public health agency surveyed other hospitals and identified four other patients with compatible illnesses who had eaten at the same restaurant. Ultimately, 23 confirmed and probable cases were linked to potato-based and eggplant-based dips served by the restaurant on April 8 or 9. Two cases were asymptomatic, 21 cases were hospitalized, and four cases required mechanical ventilation. Twenty-one persons received antitoxin.
The third large botulism outbreak occurred in 2001. On August 29, four men were hospitalized in the same Texas hospital with similar neurologic signs and symptoms (Kalluri et al., 2003). All four had eaten a chili dish served at a church supper on August 25. State health officials subsequently learned that two children who attended the church supper had been admitted to a different hospital on August 28 and 29. Ultimately physician reports and public health case finding identified 16 cases of botulism with onset of symptoms between August 25 and September 1. Ten cases were hospitalized, nine cases received antitoxin, and six cases required mechanical ventilation. Five cases were identified through active case-finding. The diagnosis of botulism was delayed from 1 to 5 days among four patients with typical symptoms who were not part of the original group hospitalized on August 29.
Further description of an outbreak involving a widely distributed food item
The last large botulism outbreak was linked to a widely distributed, commercially canned chili sauce. Two Texas siblings experienced onset of symptoms on June 29, 2007, and initially presented at separate hospitals. Eventually, the siblings were admitted to the same hospital, botulism was diagnosed, and antitoxin was requested on July 7 (CDC, 2007c). An Indiana couple experienced onset of symptoms on July 7 and presented at separate hospitals. After being admitted to the same hospital on July 9, botulism was diagnosed in both cases. Ultimately, eight cases of botulism were identified with the onset of symptoms between June 29 and August 7 (CDC, 2007d).
Discussion
Foodborne botulism is a rare disease in the United States outside of Alaska, where small hunting groups and families consume improperly fermented meat and fish products. Isolated cases and small outbreaks also continue to occur as a result of improper home canning. Against this background of sporadic illness, the intentional contamination of a susceptible food item would be recognized if an unusually large number of botulism cases occurred in a temporal-spatial cluster. Based on the results of the outbreaks described above, clustering patterns and outbreak recognition time may differ according to the food distribution type (local/regional vs. wide). In each of the outbreaks associated with a locally/regionally distributed food item, the event was recognized within 4 days following exposure because of the occurrence of multiple cases with identifiable linkages being recognized by a physician and/or by cases presenting at a common health care center. Also, in each of these outbreaks, multiple other cases occurred for which the diagnosis was delayed because the individual cases were not epidemiologically linked to other suspected cases or were misdiagnosed by a physician. It seems likely that a locally or regionally distributed food item would produce clusters of cases who would be hospitalized together, leading to the recognition of the event within 4 days following exposure.
For a widely distributed food item, recognition of the outbreak and a rapid identification of its source would depend in part on the likelihood of cases clustering in households or among friends. For example, three persons from Georgia shared meals on September 7, 2006, and were hospitalized on September 8. Suspicion of botulism initiated a public health investigation that ultimately led to the identification of the contaminated food vehicle on September 15 (CDC, 2006b; Brown et al., 2010). However, a single patient in Florida was hospitalized for 9 days before botulism was suspected and the illness linked to the same product. Similarly, the diagnoses of botulism in siblings in Texas and a married couple in Indiana led to the identification of a contaminated commercially canned chili sauce in 2007. In both instances, each member of the pair was initially evaluated at a separate hospital. However, the diagnosis of botulism was not made until both members of the pair were admitted to the same hospital.
The treatment for botulism involves administration of antitoxin that must be released by public health officials (Sobel et al., 2004; Shaprio et al., 1998). This creates a rapid and sensitive surveillance system for the occurrence of clinically suspected illnesses. An increase in antitoxin above the normal rate, or simultaneous requests for antitoxin release from multiple states would suggest the occurrence of a widespread outbreak. While the occurrence of one suspect case of foodborne botulism warrants immediate investigation, the outbreaks reviewed above clearly suggest that physicians are more likely to recognize/suspect botulism in a more timely manner if >1 case is concurrently hospitalized with symptoms consistent with botulism. Therefore, the identification of epidemiologic linkages between cases is a critical part of the diagnostic evaluation. Thus, the sensitivity of surveillance based on requests for release of antitoxin is also dependent on the occurrence of epidemiologically linked cases. Scallan et al. (2011) suggest that the severity of botulism would lead to its diagnosis and reporting in approximately half of all cases. In the outbreaks reviewed above, fewer than half of the cases with botulism were correctly diagnosed prior to recognition of the outbreak. Thus, an intentionally contaminated food item with a long shelf life and widespread distribution may cause a delay in outbreak recognition until multiple cases or family members with botulism-like symptoms are hospitalized together. The degree to which the food item was intended for individual consumption, rather than sharing, could further prolong detection of the event. Given these findings, the characteristics of product distribution and use should be factored into assessments of the potential impact of intentional contamination events and public health response.
Potential limitations in surveillance system detection coupled with the rarity of large foodborne botulism outbreaks (those >5 people) limited this study to an exploratory and descriptive analysis. Future research involving simulations, predictive modeling, and pattern recognition methodologies may provide a more informed understanding of the importance of epidemiological linkages in foodborne outbreak detection.
Conclusion
Rapid identification of foodborne botulism outbreaks is facilitated by the epidemiological linkage of cases, especially when medical professionals link cases that present together. However, outbreak detection may be delayed when single cases present, or cases are misdiagnosed. For the outbreaks described in detail, a number of the cases had mild symptoms and may have been more difficult to correctly diagnose without the context of an outbreak. Additionally, cases with mild symptoms may not have been identified or presented for care without active case finding and press releases.
In an effort to augment national botulism surveillance and antitoxin release systems and to improve food defense and public health preparedness efforts, medical organizations and Homeland Security officials should emphasize the education and training of medical personnel to improve foodborne botulism diagnostic capabilities to recognize single foodborne botulism cases and to look for epidemiologic linkages between suspected cases. Strengthening the capacity of the medical system to recognize outbreaks can mitigate the public health consequences of unintentional foodborne outbreaks and intentional contamination events.
Footnotes
Acknowledgments
We would like to thank Dr. Jeff Bender, Director of the Center for Animal Health and Food Safety, for his thoughtful review of the manuscript. This work was supported by the National Center for Food Protection and Defense (U.S. Department of Homeland Security Science and Technology Assistance agreement no. 2007-ST-061-000003).
Disclosure Statement
No competing financial interests exist.