
Abstract
Salmonella is one of the most common foodborne pathogens in humans. Laboratory-based surveillance for non-typhoidal Salmonella infection was conducted in Guangdong Province, China to improve understanding about the disease burden and detection of dispersed outbreaks. Salmonella isolated from patients with diarrhea were sent from 16 sentinel hospitals to local public health laboratories for confirmation, serotyping, antimicrobial susceptibility testing, and pulsed-field gel electrophoresis (PFGE). PFGE patterns were analyzed to identify clusters representing potential outbreaks. Between September 2009 and October 2010, 352 (4%) Salmonella isolates were obtained from 9167 stool specimens. Salmonella enterica serotype Typhimurium (45%) and Salmonella enterica serotype Enteritidis (13%) were the most common serotypes, and multidrug resistance was high, especially in Salmonella Typhimurium isolates. PFGE patterns of obtained Salmonella isolates were found to be diverse, but a unique PFGE pattern comprising 53 Salmonella Typhimurium isolates were found to occur almost exclusively in infants. Epidemiologic studies are ongoing to determine whether a common exposure is the source of the Salmonella Typhimurium strain frequently isolated from infants.
Introduction
China has an established internet-based surveillance system for notifiable infectious diseases, but laboratory-confirmed cases of Salmonella are not routinely reported and information collected from these cases are limited (Wang et al., 2008; Zhang et al., 2009). China has also not yet fully deployed a system to “fingerprint” foodborne bacterial isolates and to link “fingerprints” from different isolates to determine whether they arise from a common source (Feng et al., 2011). Outbreaks of foodborne infections that are dispersed widely in time and space are not currently detected in China.
In 2009, one of the most populous provinces in China, Guangdong, initiated enhanced laboratory-based surveillance for non-typhoidal Salmonella in humans. Guangdong is an economically developed province in south China with subtropical weather. It has an estimated population of more than 100 million permanent residents and migrant workers, divided into 21 administrative units known as prefectures. The main purpose of this surveillance system was to characterize Salmonella subtypes isolated from infected humans, according to serotype, antimicrobial resistance, and pulsed-field gel electrophoresis (PFGE) pattern. Furthermore, we sought to monitor trends of Salmonella infections and to improve detection of foodborne outbreaks through analysis and investigation of isolates with indistinguishable PFGE patterns. We report here the epidemiology, serotypes, antimicrobial resistance, and PFGE subtypes of Salmonella obtained as part of this project.
Methods
Study design
A laboratory-based surveillance program for non-typhoidal Salmonella was established in seven large prefectures, located in the western (Maoming and Yangjiang) and central (Guangzhou, Zhuhai, Zhongshan, Jiangmen, and Dongguan) Guangdong; this catchment captured more than 50 million people. Prefectures and hospitals were selected based on their interest and current public health and clinical capacity to conduct this project. Between September 2009 and October 2010, 16 hospitals from the seven administrative areas provided isolates and epidemiologic data for analysis. Of the 16 hospitals, 13 were general hospitals and the remaining three were pediatrics.
Physicians were asked to collect stool samples from patients who presented with three or more loose stools within 1 day and whose diarrhea was associated with other symptoms such as fever, vomiting, or abdominal pain (CDC, 2004). Specimens were submitted to hospital laboratories that were trained to use a standardized procedure to isolate Salmonella from stool (WHO, 2010). Salmonella isolates were forwarded to the laboratories of Guangdong Provincial Center for Disease Control and Prevention (GDCDC), where isolates were serotyped and pulsetyped, and antimicrobial susceptibilities were determined. Demographic and clinical information for each case, including age, gender, symptoms, date of illness onset, and date of specimen collection, was collected and electronically transmitted to GDCDC.
Culture and serotyping
Isolation of Salmonella from stool specimens was conducted by hospital laboratories according to World Health Organization (WHO) guidelines (WHO, 2010). Presumptively identified colonies from diarrheal samples were stored in semi-solid agar and shipped within 48 h to GDCDC, where isolates were confirmed as Salmonella using API 20E test strips (bioMerieux, Marcy-l'Etoile, France). O and H antigens were characterized by slide agglutination with commercial antiserum (S&A Reagents Lab, Bangkok, Thailand), and serotype was assigned according to the Kauffmann-White scheme (Grimont and Weil, 2007).
Antimicrobial susceptibility testing
Antibiotic susceptibility was evaluated using the Kirby-Bauer disk diffusion method for 12 antimicrobial agents, including ampicillin (AMP), cefotaxime (CTX), ceftazidime (CAZ), cefepime (FEP), chloramphenicol (CHL), tetracycline (TET), nalidixic acid (NAL), ciprofloxacin (CIP),streptomycin (STR), gentamicin (GEN, sulfamethoxazole (SMX), and trimethoprim (TMP) (Oxoid, Basingstoke, UK) (see Table 2 below). Isolates were classified as resistant, intermediate, or susceptible according to the Clinical Laboratory Standards Institute (CLSI) guidelines (CLSI, 2011). We defined an isolate as multidrug resistant (MDR) if it was resistant to three or more classes of antimicrobial agents, and we defined an isolate as having “clinically important resistance” if it was resistant to one or more of the following agents: AMP, CTX, CAZ, FEP, CIP, GEN, TMP, and SMX (Varma et al., 2005). The multidrug-resistance pattern (ACSSuT) was defined as resistance to at least AMP, CHL, STR, SMX, and TET, which is equivalent to the classical Salmonella Typhimurium DT104 resistance phenotype. Escherichia coli ATCC 25922 was used for quality control in each disk diffusion test in accordance with CLSI guidelines.
DNA sub-typing
GDCDC determined the pulsetypes for the five most common Salmonella serotypes within 1 week of receiving isolates. DNA patterns representative of each isolate were analyzed for genetic relatedness according to a validated protocol (Ribot et al., 2006). Briefly, agarose-embedded DNA was digested with enzyme XbaI (Promega, Madison, WI) overnight in a water bath at 37°C. Fragments of digested DNA were separated by electrophoresis in 0.5×Tris-borate-EDTA at 14°C for 18 h using a CHEF-DR III system (Bio-Rad Laboratories, Hercules, CA). Comparison of the PFGE patterns was performed using Bionumerics software version 6.0 (Applied Maths, Sint-Martens-Latem, Belgium), and patterns were compared using Dice coefficients with a 1.5% band position tolerance and 1% band optimization. Isolate relatedness was determined using the unweighted pair group method with averages (UPGMA). PFGE patterns were identified as “clusters” according to existing guidelines (Barrett et al., 2006).
Microbiological and PFGE data were reviewed weekly to detect clusters representing potential outbreaks. PFGE patterns associated with case clusters in Guangdong were compared with patterns uploaded to the PulseNet China database as well to strains observed in other countries through the PulseNet International network. Hospital microbiology laboratories participated in an external quality assurance system for Salmonella isolation conducted by GDCDC. Workshops were held among participating hospitals to standardize protocols, review progress, and discuss results. The national reference laboratory for enteric pathogens at China CDC provided technical support on an ongoing basis. Since 2007, GDCDC has participated annually in the External Quality Assurance System (EQAS) of the WHO Global Foodborne Infections Network (WHO GFN) (Hendriksen et al., 2009a,b).
Statistical analysis
Serotype and antimicrobial resistance data were analyzed using SAS Version 9.1 (SAS Institute, Cary, NC). A p-value of <0.05 was regarded as statistically significant.
Results
Epidemiology
Between September 2009 and October 2010, a total of 9,167 stool specimens were cultured from patients with diarrhea in Guangdong, resulting in 352 Salmonella isolates (3.8%). The isolation rate ranged from 0.8% to 7.4%, varying by month (Fig. 1).

Overall isolation rate for Salmonella by month in Guangdong province.
Patients with diarrhea ranged in age from 20 days to 90 years old; the median age was 1 year (inter-quartile range, 8 months to 7 years). More than half (51.7%) of the patients were aged less than 1 year. Children aged 1–5 years accounted for 12.2% of all cases, young people aged 6–19 years accounted for 4.4%, adults 20–60 years accounted for 15.3%, and adults older than 60 years accounted for 3.7% of all the patients; 12.7% of cases were of unknown age. The overall male-to-female ratio was 1.25:1.
Serotype distribution
We found 66 serotypes among the 352 Salmonella isolates, with 11 serotypes accounting for 82.1% (289/352) of all isolates (Table 1). Salmonella enterica serotype Typhimurium (45.2%) was the most common serotype, followed by Salmonella enterica serotype Enteritidis (12.2%), Salmonella enterica serotype Stanley (7.1%), Salmonella enterica serotype 4,5,12:i:- (4.5%), and Salmonella enterica serotype Weltevreden (3.1%). A wide variety of serotypes were detected among the remaining 63 isolates, including seven untypable isolates. Among the 159 Salmonella Typhimurium isolates, 69.8% (111/159) were isolated from children aged less than 1 year; 83.6% (133/159) were isolated from children less than 5 years. Fifteen (93.8%) out of the 16 Salmonella 4,[5],12:i:- isolates were obtained from children aged less than 1 year. In comparison, Salmonella Enteritidis, Salmonella Stanley, and Salmonella Weltevreden were more often isolated from adults (p<0.05).
Antimicrobial susceptibility
A total of 305 (86.7%) isolates were resistant to at least one antimicrobial agent. Resistance to at least one clinically important antimicrobial agent was found in 67.6% (238/352) of all isolates; resistance to three or more clinically important agents was found in 51.1% (180/352). A high prevalence of resistance was observed for NAL (65.1%), SMX (63.1%), TET (61.1%), and AMP (60.5%) (Table 2). Some isolates were resistant to extended-spectrum cephalosporins, including CTX (11.4%), FEP (7.7%), and CAZ (7.1%). Only 2.8% (10/352) of the isolates were resistant to CIP; however, a high proportion of isolates (29.3% [103/352]) showed intermediate resistant to CIP, and 17.5% (18/103) of which were also resistant to at least one extended-spectrum cephalosporin.
Clinically important antimicrobials include the following agents: ampicillin, cefotaxime, ceftazidime, cefpime, ciprofloxacin, gentamicin, sulfamethoxazole, and trimethoprim.
Resistance to at least ampicillin, chloramphenicol, streptomycin, sulfamethoxazole, and tetracycline.
Antimicrobial resistance profiles for the five most common serotypes of Salmonella in Guangdong are listed in Table 3. Compared to the other four serotypes, Salmonella Typhimurium isolates were more frequently resistant to antimicrobial agents. More than 80% of the Salmonella Typhimurium isolates were resistant to AMP (89.9%), SMX (89.3%), TET (89.9%), and NAL (86.2%). For CIP, 5.0% of Salmonella Typhimurium isolates were resistant, while 51.6% showed intermediate resistance. Resistance to extended-spectrum cephalosporins (CTX, CAZ, and FEP) was observed in more than 10% of the Salmonella Typhimurium isolates. Two Salmonella Typhimurium isolates showed resistance to both ciprofloxacin and extended-spectrum cephalosporins. The proportion of Salmonella Typhimurium isolates with the ACSSuT resistance pattern was 62.3%. Salmonella 4,5,12:i:- isolates showed a similar prevalence of resistance for most tested antimicrobial agents. Multidrug resistance and ACSSuT resistance pattern were observed in 93.8% and 31.3% of the Salmonella 4,5,12:i:- isolates, respectively. Most Salmonella Enteritidis isolates were resistant to NAL (74.4%), but only one was resistant to CIP.
Salmonella Stanley and Salmonella Weltevreden isolates were highly susceptible to all agents tested with the exception of one Salmonella Stanley (resistant to SMX) and two Salmonella Weltevreden isolates (resistant to AMP and SMX, respectively).
PFGE patterns
For this article, we restricted PFGE analysis to isolates belonging to the most common Salmonella serotypes. A total of 253 Salmonella Typhimurium, Salmonella Enteritidis, Salmonella 4,5,12:i:-, Salmonella Stanley, and Salmonella Weltevreden were analyzed for genetic relatedness by PFGE using enzyme XbaI. Seventy-seven distinctive XbaI patterns were observed among the 159 Salmonella Typhimurium isolates. Using a cut-off value of 85% similarity, four clusters and a few individual types were observed among the Salmonella Typhimurium isolates. Cluster 1 was the most common cluster, containing 116 isolates (Fig. 2). Within Cluster 1, the largest indistinguishable XbaI-PFGE pattern (JPXX01.GD0004) contained 53 (33.3%) Salmonella Typhimurium isolates. Notably, all of these isolates were recovered from children, of which 81.1% (43/53) were from infants aged less than 1 year. This PFGE pattern was first observed in September 2009 and then reappeared almost every month among all of the seven prefectures in Guangdong throughout the sampling period. Most isolates with this pattern had the ACSSuT resistance pattern and intermediate resistance to CIP. When searching in the newly created PulseNet China database, we obtained 580 historical Salmonella Typhimurium isolates from Chinese provinces other than Guangdong; 73 (12.6%) had the JPXX01.GD0004 pattern. Using the PulseNet International network, we were also able to survey the distribution of this pattern in other countries. Comparative analysis showed that this pattern was uncommon and not associated with any known outbreaks in the United States, Canada, Denmark, or Hong Kong.
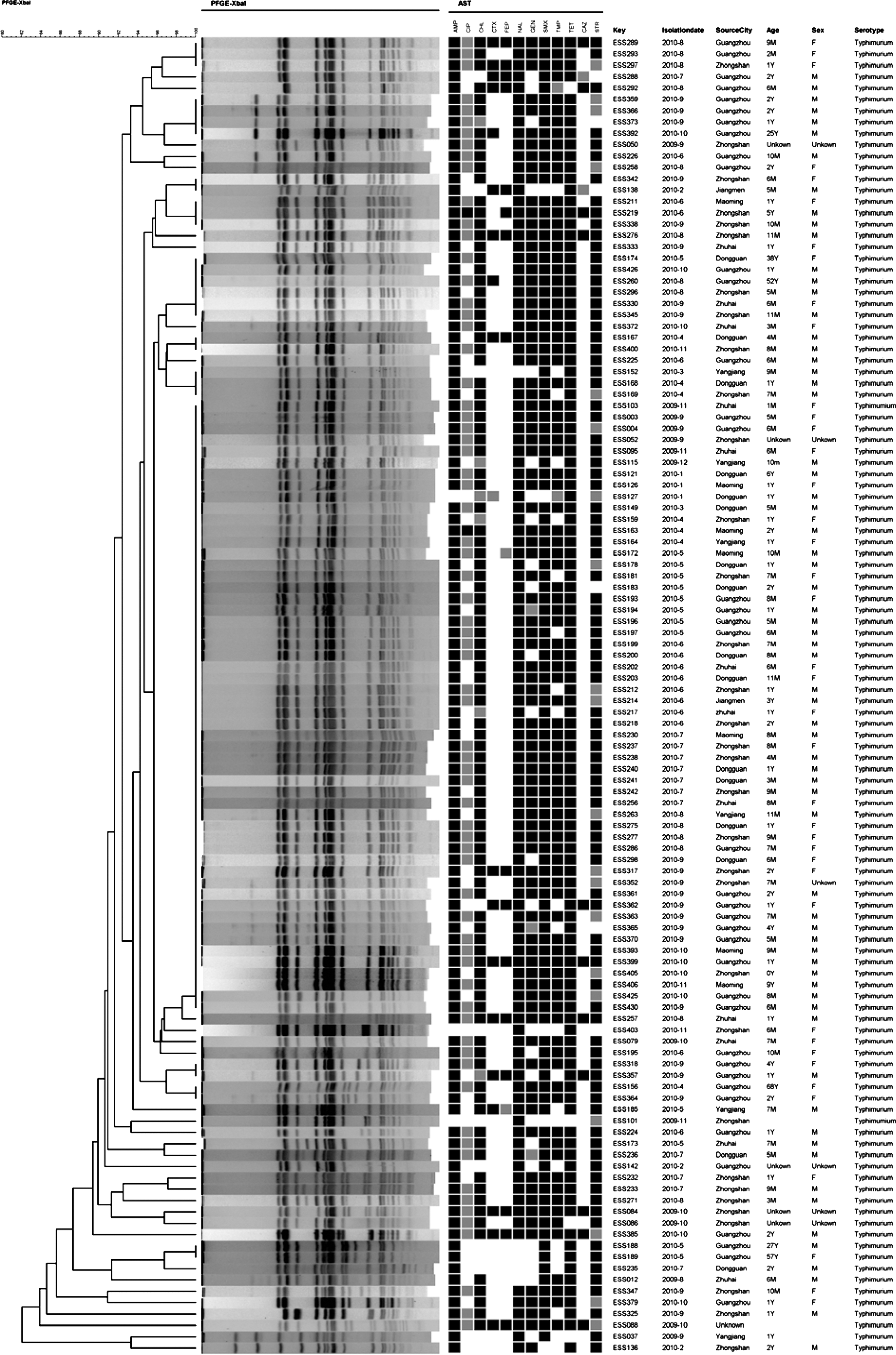
Unweighted pair group method with averages (UPGMA) analysis of pulsed-field gel electrophoresis (PFGE) profiles of 116 Salmonella enterica serotype Typhimurium in Guangdong from September 2009 to October 2010. A black box indicates resistance to the particular antimicrobial agent; a gray box indicates intermediate resistance to the particular antimicrobial agent. AMP, ampicillin; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefpime; CHL, chloramphenicol; CIP, ciprofloxacin; GEN, gentamicin; SMX, sulfamethoxazolel; TMP, trimethoprim; TET, tetracycline; STR, streptomycin.
The 16 Salmonella 4,5,12:i:- isolates showed 11 different XbaI PFGE patterns; five of the isolates had an identical XbaI pattern (JPXX01.GD0004, noted above). The 53 Salmonella Typhimurium and five Salmonella 4,5,12:i:- isolates that had indistinguishable XbaI pattern were further analyzed using the enzyme BlnI to confirm similarity; 30 of 53 Salmonella Typhimurium remained undistinguished after comparison of BlnI digestion patterns. The five Salmonella 4,5,12:i:- isolates could be distinguished from the Salmonella Typhimurium isolates by their BlnI patterns.
The 43 Salmonella Enteritidis isolates were assigned to 17 different XbaI patterns. Sixteen isolates (35%) were assigned to one indistinguishable XbaI cluster, and nine were assigned to a second indistinguishable cluster (Fig. 3). The Salmonella Enteritidis isolates were found across all prefectures and from diverse age groups. The 25 Salmonella Stanley isolates were assigned to eight different XbaI patterns, with 10 (40%) showing the same digestion pattern. The 11 Salmonella Weltevreden isolates were assigned to five different XbaI PFGE patterns, one of which consisted of five isolates (data not shown).

Unweighted pair group method with averages (UPGMA) analysis of pulsed-field gel electrophoresis (PFGE) profiles of 43 Salmonella enterica serotype Enteritidis in Guangdong from September 2009 to October 2010. A black box indicates resistance to the particular antimicrobial agent; a gray box indicates intermediate resistance to the particular antimicrobial agent. AMP, ampicillin; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefpime; CHL, chloramphenicol; CIP, ciprofloxacin; GEN, gentamicin; SMX, sulfamethoxazolel; TMP, trimethoprim; TET, tetracycline; STR, streptomycin.
Discussion
Although many developed countries conduct laboratory-based surveillance for enteric infections, China has only recently attempted to establish such a system. During the first year of laboratory-based surveillance in Guangdong, we detected a large cluster of Salmonella Typhimurium infections among infants and found that strains with this antimicrobial resistance pattern were highly resistant to clinically important antimicrobial agents. Our work also showed that this resistance pattern was not exclusive to Salmonella Typhimurium strains; other serotypes also expressed this resistance phenotype as well, reinforcing the need to couple phenotypic and genetic traits in characterizing diarrheal-causing strains of bacteria.
Infants accounted for a large proportion of cases in Guangdong, and DNA sub-typing identified one strain as the most common etiology for this group. Epidemiologists initiated an investigation of the large cluster of infant Salmonella Typhimurium–related diarrhea in January 2010 to determine the source. However, this study failed to identify a common food, water, or animal exposure associated with infection. In addition, some samples (including water, baby formula, and home animal swabs) were tested by laboratory, but no matched pathogens were identified (data not included in this study). Additional epidemiological investigations are in progress to identify the source of this unique Salmonella Typhimurium strain which is frequently isolated from infants.
The presence of resistance to multiple antimicrobial agents suggests that this strain arose under intense antimicrobial pressure, which is common among Salmonella transmitted by animals reared for food (Voetsch et al., 2004). How infants would have acquired Salmonella from a food animal source is also not clear; many were not yet eating solid foods, and no link to a common source of milk or formula was found (data not shown). Large outbreaks of Salmonella have been associated with infant food, but most infections are not part of a recognized outbreak, and the route of transmission for these sporadic infections is not well understood (Investigation Internationale, 1997; Rushdy et al., 1998). One large case-control study of infant Salmonella infections in the United States identified multiple risk factors, including absence of breastfeeding, consumption of concentrated liquid infant formula, contact with reptiles, riding in a shopping cart next to meat, and attendance at day care with other ill children (Jones et al., 2006). To investigate this problem, the following steps need to be taken. First, laboratory-based integrated Salmonella surveillance needs to be enhanced throughout China to combine both human and animal sides and to combine epidemiology, clinical, and laboratory. Second, there is a need to strengthen epidemiologic investigation of infant Salmonella infections. Guangdong epidemiologists are now conducting extensive interviews and home visits for all infant Salmonella cases from this surveillance system to generate hypotheses about a common source and transmission route.
Salmonella 4,5,12:i:- was found to be one of the most common serotypes in Guangdong. This serotype is antigenically similar to Salmonella Typhimurium which has the antigenic formula 4,5,12:i:1,2, but lacks expression of the second phase flagellar antigen (Switt et al., 2009). Salmonella 4,5,12:i:- has recently been recognized as an emerging cause of infection around the world (Hopkins et al., 2010; Switt et al., 2009). The high rate of multidrug resistance observed in China for this serotype is similar to Europe and South Asia (Hopkins et al., 2010; Pornruangwong et al., 2008), but this is not the case in North and South America (Hoelzer et al., 2010; Switt et al., 2009). Resistance to clinically important antimicrobial agents was also common among most Salmonella serotypes isolated in our surveillance and was higher than that reported in Western countries, but similar to other Asian countries (Lee et al., 2009; Ong et al., 2007; Su et al., 2004; Weill et al., 2006). Antimicrobial resistant Salmonella is an important public health problem, because resistant Salmonella infections have been associated with an increased risk of bloodstream infection (Helms et al., 2002; Martin et al., 2004). Further studies are needed to understand factors (e.g., selection pressure, pharmaceutical policy, “over the counter” usage) driving antimicrobial resistance among Salmonella serotypes and to measure the human health impact of antimicrobial resistance in China.
The most important limitation of our study was the low sensitivity of our system for laboratory-confirmed Salmonella. First, the province is heavily populated—larger than most countries in the world—yet only one to three hospitals in each prefecture were enrolling patients as a part of this project. Second, although we have recommended a standard case definition and isolation guideline, only a proportion of all patients with diarrhea have stool specimens collected for culture, and different practices between hospitals affect the enrollment of patients for stool culture. Finally, the overall Salmonella isolation rate was low, possibly because of previous antibiotic use or laboratory recovery. In the future, increasing the rate of specimen collection, the rate of isolation, the number of facilities in surveillance, and our understanding about health-seeking behavior will help to improve our understanding about disease incidence and increase the sensitivity for outbreak detection.
Conclusion
In conclusion, the first year of laboratory-based Salmonella surveillance in Guangdong identified a unique strain of multi-drug resistant Salmonella Typhimurium causing illness among infants and high rates of antimicrobial resistance for most serotypes. Epidemiologic studies of infant Salmonella and antimicrobial resistance, combined with efforts to improve the sensitivity of surveillance, will help strengthen both understanding and control of foodborne pathogens in China.
Footnotes
Acknowledgments
We are grateful for the participation and excellent work by sentinel hospitals in Guangdong Province. We also thank the China Field Epidemiology Training Program for technical support. In addition, we thank the technical experts from WHO Global Foodborne Infections Network, including Danilo M.A. Lo Fo Wong (WHO), Frederick J. Angulo and Patricia M. Griffin (CDC, United States), Jaap Wagenaar (Utrecht University, The Netherlands), Rene Hendriksen (National Food Institute, Denmark), Shaohua Zhao (Food and Drug Administration, United States) and Lai-King Ng (Public Health Agency of Canada, Canada). PulseNet International is acknowledged for their kind support in comparing Salmonella PFGE patterns in their database. This study was supported by the China—U.S. Collaborative Program on Emerging and Re-Emerging Infectious Diseases and WHO Global Foodborne Infections Network.
Disclosure Statement
No competing financial interests exist.