
Abstract
A variety of approaches to attribute foodborne diseases to specific sources are available, including hazard occurrence analysis, epidemiological methods, intervention studies, and expert elicitations. The usefulness of each method to attribute disease caused by a foodborne hazard depends on the public health question being addressed, on the data requirements, on advantages and limitations of the method, and on the data availability of the country or region in question. Previous articles have described available methods for source attribution, but have focused only on foodborne microbiological hazards. These articles have described strengths and weaknesses of each method, but no guidance on how to choose the most appropriate tool to address different public health questions has thus far been provided. We reviewed available source attribution methods; assessed their applicability to attribute illness caused by enteric, parasitic, and chemical foodborne hazards to the responsible sources; and renamed some of the approaches. The main objective was to make recommendations on the most appropriate method(s) to attribute human disease caused by different foodborne hazards. We concluded that the proportion of disease that can be attributed to specific foods items or transmission routes may be estimated for the majority of the evaluated hazards by applying one or more of the source attribution methods assessed. It was also recognized that the use of source attribution methods may be limited to specific countries, reflecting the data availability.
Introduction
F
A variety of approaches to attribute foodborne diseases to specific sources are available, including hazard occurrence analysis (the subtyping and the comparative exposure assessment methods), epidemiological methods (analysis of data from outbreak investigations and studies of sporadic infections), intervention studies, and expert elicitations (Pires et al., 2009a). Each of these methods presents advantages and limitations, and the usefulness of each depends on the public health questions being addressed and on characteristics and distribution of the hazard. Additionally, methods have different data requirements and attribute human illness at either the point of production (reservoir) or of exposure to the food, and therefore their utility will vary depending on the hazard and/or the country or region in question. The choice of the method to be used should be guided by these factors.
In 2006, the World Health Organization developed a strategy to estimate the global burden of foodborne disease (
Previous articles and reports have described available methods for source attribution, their requirements, advantages, and limitations, but have focused only on foodborne microbiological hazards (Batz et al., 2005; EFSA, 2008; Pires et al., 2009). These articles have described the general strengths and weaknesses of each method, but no guidance on how to choose the most appropriate tool to address different public health questions had been provided thus far. We reviewed available source attribution methods, assessed their applicability to attribute illness by foodborne hazards of each hazard-group (enteric pathogens, including bacterial and viral pathogens, as defined by FERG; parasites; and chemicals) to the responsible sources, and renamed some of the approaches. The main objective of this review was to make recommendations on the most appropriate method(s) to attribute human disease caused by specific foodborne hazards.
Main Concepts
Human foodborne illness source attribution is defined as the partitioning of the human disease burden of one or more foodborne illnesses to specific sources, where the term source includes reservoirs and vehicles. We restrict the term reservoir to describe an animal species or nonanimal substance upon which a pathogen depends for its survival or from which a chemical compound originates. Many foodborne hazards have more than one reservoir. We define a vehicle as an inanimate carrier of a hazard from its original reservoir until final exposure. The pathway from reservoir to exposure may involve multiple vehicles; vehicles of foodborne hazards are traditionally food items, but other sources (e.g., contaminated drinking water, recreational water, or live animals) can be vehicles of the same hazard.
Harmonized source categorization is necessary to compare and integrate results from various data sources, source attribution models, approaches, or hazards. FERG considers four main types of transmission routes from the main reservoirs to humans: foodborne, environmental, direct contact with animals, and person-to-person transmission; for the purpose of source attribution, person-to-person transmission may not be relevant because the aim is to estimate the relative importance of the original sources of the pathogen (to which the index case would have been exposed to) and to use this information to define control measures in the food chain. For foods, FERG has adopted a categorization scheme adapted from Painter et al. (2009) and modified it to accommodate subcategories that are common in the countries or regions of a particular study. When relevant, environmental transmission routes (e.g., contaminated water or air emissions of industrial pollutants) and transmission through direct contact with animals are considered.
Human illness source attribution can take place at different points along the food chain (points of attribution), most often at the point of reservoir (e.g., animal production stage, environment emissions) or point of exposure (end of the transmission chain). The point of attribution depends on the method chosen, which will depend on the risk management question being addressed and on the availability of data. Source attribution estimates obtained through the application of different methods are not necessarily comparable and optimally should not be used exclusively, but instead—and whenever possible—be complemented with results of other studies.
Usefulness and Applicability of Source Attribution Methods for Foodborne Hazards
The assessment of the usefulness and applicability of methods to attribute foodborne disease to the main types of transmission (foodborne, environmental, animal contact, and person-to-person) and to specific foodborne routes was qualitative and based on characteristics of the methods and of the hazards. In addition, published source attribution studies were collected and reviewed to support the assessment.
The principles and data requirements of available source attribution methods are summarized in Table 1, which also includes references to examples of conducted studies. More details of the methods, as well as strengths and limitations of each, have been described in Pires et al. (2009), Batz et al. (2005), and the European Food Safety Authority (EFSA) (2008).
Includes case–control studies, case-series studies, and cohort studies.
NA, nonapplicable.
Attribution of human illness to foods, environment, and person-to-person and animal contact
The first step in the source attribution process is to estimate the overall proportion of the burden of disease that can be attributed to the four main transmission routes. For most foodborne hazards, data-driven methods, based, for example, on surveillance and monitoring data, would require an exhaustive review and inclusion of all potential sources and pathways within these main routes, and consequently are not the most appropriate tool for this initial step when applied individually. We concluded that a combination of epidemiological methods could provide a more adequate picture of the relative importance of the types of transmission, namely, a combination of an analysis of outbreak data and of studies of sporadic cases. For hazards that are transmitted through a limited number of routes (e.g., Brucella spp.), the application of one epidemiological approach for source attribution may be sufficient. Alternatively, two methods are currently available to attribute disease to these main routes: expert elicitations and intervention studies.
Attribution of foodborne disease to food and other transmission routes could be undertaken for individual foodborne hazards or for syndromic groups (e.g., diarrheal disease). In both cases, expert elicitations can be conducted at a country or regional level, whereas interventions are optimally designed as small-scale population-based studies. The latter are also expensive and difficult to apply.
Attribution of human illness to specific foods
The usefulness and applicability of the available methods to attribute the burden of a disease to specific sources and pathways depends on the risk management question, on the characteristics of the hazard causing the disease, and on the data available to address the question. Figure 1 presents a diagram (here called tool-box for source attribution) that illustrates how these factors may influence the utility of source attribution methods, and how each method can be considered as a first or alternative choice to attribute human disease to sources.
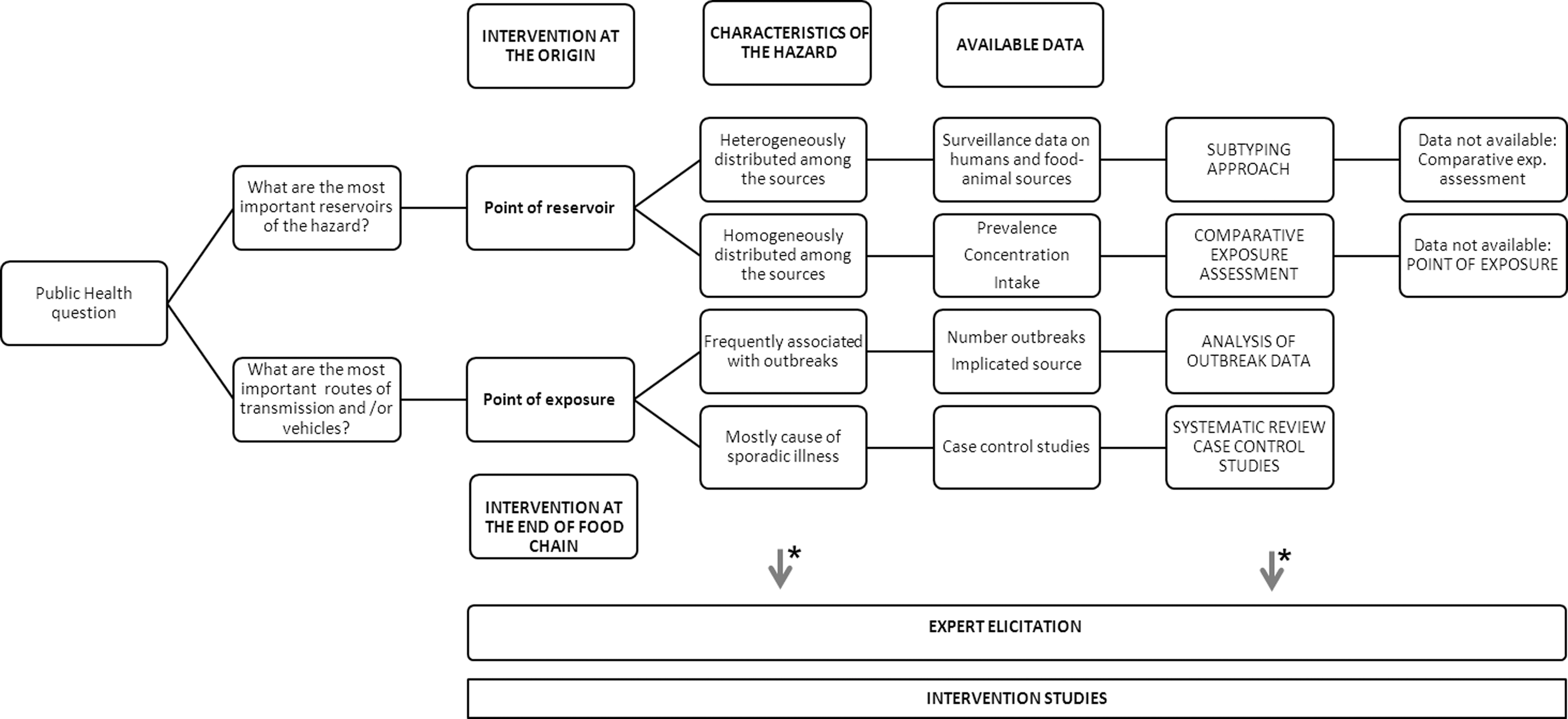
Tool-box for source attribution. *Expert elicitations and intervention studies are useful to attribute illness at any point of the transmission chain.
The risk management question will depend on countries/regions' food safety problems. The assessment of the applicability of methods was made for each foodborne hazard individually and was based on (1) the diversity and type of sources and routes of transmission to humans; (2) the existence of different subtypes of the hazard (e.g., species, serotypes, forms); (3) the availability of occurrence and surveillance data in the different world regions; and (4) the frequency of outbreaks of disease. When more than one source attribution method proves useful, the final choice of method will be determined by the question that needs answering and will be influenced by the analytical capacity in a country and the level of data sharing between agencies.
Source attribution studies already conducted and publicly available that could be identified were collected, and their results were analyzed and compared to support the assessment. The list of hazards considered in this review was based on the priority list defined by FERG (
The type of reservoir of the hazard will influence the applicability of some source attribution methods, particularly the subtyping approach. This approach applies to hazards with one or more animal reservoirs, to which disease can be traced back and where the hazard can potentially be controlled. Remaining approaches are in principle applicable regardless of the origin of the hazard, since they focus on routes of transmission or the point of exposure. Among epidemiological studies of sporadic cases, individual case-series, cohort, or case–control studies may be used to estimate the relative importance of risk factors for foodborne agents at a country (or part of the population) level, while a systematic review and meta-analysis of published studies will be useful to attribute disease at a more general or regional level; we focus here on the applicability of the latter. This approach can be applied when a sufficient number of studies have been conducted and published, and is able to combine results from multiple countries or regions and infer on the most important sources or risk factors for disease.
Enteric bacterial and viral pathogens
Enteric pathogens may include bacteria, virus, or parasites (the latter is addressed in the section on parasites, later in this article) and typically cause acute gastroenteritis in humans. Most enteric pathogens can be divided according to their main reservoir: (1) animal (one or more animal reservoirs) (e.g., Salmonella spp., Campylobacter spp.); (2) human (e.g., Shigella spp.); and (3) environment, including soil (e.g., Clostridium botulinum), and water (e.g., Vibrio cholerae). The majority of the enteric pathogens under focus are mostly transmitted through foods, but may also be transmitted through environmental routes, direct contact with animals, or person-to-person transmission.
Table 2 presents an overview of the applicability of available source attribution methods for enteric pathogens. Some methods were found to be more appropriate than others, but their application may be constrained by data unavailability in some countries or regions, and (when available) alternatives are presented.
STEC, Shiga toxin–producing Escherichia coli.
The subtyping approach proved to be the most appropriate method for Salmonella and Campylobacter. Both pathogens have animal reservoirs and occur in different forms (subtypes). For Salmonella, typing schemes are routinely or frequently applied in several countries worldwide, and typing data from public health surveillance and animal monitoring are frequently available. The approach has the advantage of attributing illness to the reservoir level (i.e., to the original sources of the pathogen), making its results particularly useful to inform risk management decisions and intervention strategies at the production level.
The subtyping approach has been successfully applied to attribute salmonellosis to sources in several countries. Some of these studies have demonstrated that a microbial subtyping model can be applied to attribute salmonellosis to sources in countries with less complete data sets (e.g., data with lower subtyping discriminatory power that derives from less sophisticated surveillance systems); this can be done by applying the model to data from multiple years (Pires and Hald, 2010) or from multiple countries (Pires et al., 2011c). For Campylobacter, the approach has been applied in several countries, namely, the United Kingdom. However, despite extensive work using a wide range of subtyping approaches, the application of such methodologies has hitherto not been as successful as for Salmonella. Additionally, the fact that few countries have implemented Campylobacter surveillance in animal production systems, and that genotypic typing methods are rarely applied results in a lack of suitable data in most regions of the world. A microbial subtyping approach has also been applied to attribute human cases of Listeria monocytogenes to sources in the United Kingdom (Little et al., 2010). Nonetheless, because L. monocytogenes does not have an animal reservoir and is not clonally disseminated through the food chain, the uncertainty in the estimates is large and may as a consequence compromise the validity of the results.
An analysis of data from outbreaks has been shown useful to attribute disease by several pathogens, and was considered the most appropriate method for Bacillus cereus, Clostridium perfringens, Clostridium botulinum, norovirus, Salmonella (if subtyping data is not available), Shiga toxin–producing Escherichia coli (STEC), Shigella, Staphylococcus aureus, Vibrio cholerae, and Yersinia enterolitica. Data from outbreak investigations for these pathogens are frequently available in both developed and developing countries, the method is easy to adapt, and results provide a useful indication of the most important sources of disease in the population. Moreover, the approach can be applied at a regional level, making it useful even in case of limited data availability at a country level (e.g., countries with few outbreaks reported each year).
The comparative exposure assessment was found to be an appropriate method to attribute disease by Campylobacter, Brucella spp., STEC, and L. monocytogenes, all pathogens being mostly transmitted through a limited number of food routes. The approach has been applied to attribute campylobacteriosis in The Netherlands (Evers et al., 2008) and New Zealand (Lake et al., 2007), and results have proven useful, particularly in exploring the contribution of nonanimal food sources (e.g., fresh produce) and nonfoodborne routes of transmission. Both studies highlighted the limitations resulting from paucity of data and large uncertainties, but occurrence and exposure data for these pathogens exist in many countries (including developing countries), which represents an advantage of the use of this approach.
A systematic review of epidemiological studies of sporadic infections was found to be an appropriate choice to attribute illness by Brucella spp., and a useful source attribution approach for STEC and Shigella. This approach has been recently applied and proven useful for Salmonella and Campylobacter (Domingues et al., 2012a, 2012b), but a replication of an analysis would only be useful after a sufficient number of additional studies are published. For this reason, the method is not suitable for routine source attribution analysis (e.g., annual source attribution) for any foodborne hazard.
Intervention studies are potentially useful to estimate the relative contribution of different sources of disease by most pathogens. Nonetheless, these are not often conducted because they are expensive and difficult to implement. Moreover, large-scale intervention programs (e.g., national control programs) typically encompass several measures and are influenced by external, concurrent factors, which hampers the measurement of the effect of specific interventions implemented in a given source on the burden of disease. On the other hand, small-scale/controlled studies are useful if the number of exposure pathways is limited for a particular hazard and each pathway is well‐characterized from source to exposure. In our review, intervention studies proved useful only for V. cholera. Several studies have investigated the role of different strategies in preventing disease conducted throughout the world (see e.g., Mintz et al., 1995).
Expert elicitations constitute an alternative method for all pathogens, whenever the data requirements for other (most appropriate) choices are not fulfilled.
Parasites
The assessment of the usefulness of source attribution methods excluded parasites with a single definitive animal host (e.g., Taenia solium and Anisakis simplex), where elimination of the parasite in that host or breaking the infections cycle would prevent infection in humans.
Table 3 presents the recommended source attribution methods to attribute human illness by parasites. Alternatives for the most appropriate method (first choice) are presented in cases of data unavailability.
The subtyping approach does not apply to any of the parasites covered by this review since the pathogens are not routinely subtyped. Likewise, occurrence data appear to be unavailable, limiting the use of a comparative exposure assessment approach. Epidemiological studies of sporadic infections are most useful to identify the relative importance of exposure routes for disease caused by Cryptosporidium spp. and Giardia lamblia. Several case–control studies of sporadic infections have been conducted and published throughout the world. Thus, a systematic review and meta-analysis of these studies were found to be the most appropriate method for these two pathogens. This approach would be useful for source attribution at a regional level. For Toxoplasma gondii, this method was also found appropriate, and a comparative exposure assessment was found useful to estimate the relative risk posed by different meat sources. The method has been successfully applied in the Netherlands (Opsteegh et al., 2011) and, if data are available, could be useful in other countries.
An analysis of outbreak data was found appropriate to attribute disease by Fasciola hepatica and Trichinella spp., as outbreaks do occur and are reported throughout the world, and data from outbreak investigations are available in some regions.
No occurrence data or epidemiological studies are available for Ascaris lumbricoides, Echinococcus spp., and E. histolytica, and the only method found useful to attribute human illness by these pathogens was expert elicitation. This approach can be applied to any of the parasites if the data requirements for other methods are not met.
Chemical hazards
Chemical foodborne hazards may cause chronic disease, usually as a consequence of long-time exposure, potentially with accumulation of the hazard in the human body. Chronic disease is frequently linked to carcinogenic and genotoxic effects, kidney and liver malfunctioning, among others. In general, case–control studies investigating the impact of exposure to these hazards on human health focus on the disease (e.g., cancer) and its risk factors (e.g., exposure to a chemical compound). However, they seldom focus on food exposure, as this would be more appropriate for acute diseases, for which it is possible to measure an association between the consumption of a food and the onset of disease within a short period of time. Consequently, case–control studies do not appear useful to attribute disease by these compounds. In contrast, cohort studies, when available, may be useful to identify risk factors and sources of exposure to the hazards.
In general, chemical hazards do not present multiple forms with different associations between sources, and thus the subtyping approach does not apply. Dioxins and dioxin-like compounds are an exception, as these occur in different forms, and it may be possible to investigate the source of origin through a subtyping approach; however, this has never been tested. Likewise, and because outbreaks of disease are rare or nonexistent, an outbreak analysis approach is not useful to attribute human disease.
The overview of methods recommended to attribute disease by chemical hazards is presented in Table 4.
The comparative exposure assessment approach proved to be the most appropriate method to attribute disease by the chemical hazards under study. Each hazard has a relatively small number of routes of exposure, and occurrence data (concentration) of the hazards in food sources are available in several countries worldwide. The approach has previously proven useful to compare the relative exposure to various chemical hazards through different foods (in, e.g., European Member States). Examples of successful studies are the exposure assessments conducted by EFSA for aflatoxins (EFSA, 2007), cadmium (EFSA, 2009b), and lead (EFSA, 2010). This approach is a simple application and can be applied to other countries when exposure data are available.
Epidemiological studies, particularly cohort studies, have been undertaken for lead, and a review of these could be useful for source attribution. These approaches have not been found useful for any other hazard. In case of lack of data for other source attribution methods, an expert elicitation was presented as an alternative for all the hazards.
Discussion
In this evaluation, we concluded that expert elicitations or intervention studies are the most appropriate methods to estimate the proportion of a disease attributed to foods for hazards that are not predominantly foodborne. Other source attribution methods could be used, namely, epidemiological approaches (EFSA, 2008). However, estimating the proportion of disease that is foodborne in a comprehensive manner (i.e., accounting for all potential food routes) or relatively to other (nonfoodborne) transmission routes may be challenging using these data alone. Individual analyses of sporadic illnesses are often unable to quantitatively estimate the attribution for a full range of potential exposure pathways, and although outbreak surveillance systems usually document foodborne and other transmission routes (e.g., environmental routes), a summary of these data may not provide a complete picture of the relative contribution of different types of transmission for disease, because (1) captured transmission routes may not represent the variety of pathways within these main groups, or (2) some types of transmission are not likely to cause outbreaks at all. As illustrations, exposure through drinking water is likely to cause outbreaks; on the other hand, illness caused by direct contact with live animals is more likely to occur sporadically, and consequently not be captured in an outbreak surveillance system.
We also concluded that the proportion of disease that can be attributed to specific foods items or transmission routes may be estimated for the majority of the evaluated hazards by applying one or more of the source attribution methods assessed. However, it is also recognized that the estimates may be limited to specific regions of the world reflecting the data availability. In general, epidemiological approaches, specifically analysis of outbreak data and systematic review and meta-analysis of case–control studies of sporadic infections, proved useful for source attribution at a regional level when data are not available a country level. For Entamoeba histolytica, Echinococcus, and A. lumbricoides, expert elicitation appears at this point to be the only approach available.
The applicability and usefulness of the source attribution methods described varied for enteric, parasitic, and chemical hazards. In general, it can be concluded that, if an enteric pathogen has mainly an animal reservoir, can be subtyped by appropriate discriminatory methods, and subtyping data are available, the subtyping approach is appropriate to attribute human disease by that pathogen. This was verified for only two pathogens (Salmonella spp. and Campylobacter spp.). For the majority of the remaining enteric hazards, we concluded that source attribution by an analysis of data from outbreak investigations is appropriate. The comparative exposure assessment has been shown useful to attribute infections by pathogens that are mostly transmitted by a limited number of food routes, namely, STEC, L. monocytogenes, and Brucella. A systematic review of epidemiological studies of sporadic infections can be useful for enteric hazards that have been extensively studied throughout the world. From this group of hazards, the expert elicitation approach was the only source attribution option only for Entamoeba histolytica.
The nonenteric parasites included in this review have mainly one reservoir (e.g., Toxoplasma gondii in felines, Fasciola hepatica in ruminants), and thus source attribution methods may be particularly useful to estimate the proportion of disease that is foodborne, distinguishing it from waterborne, person-to-person, or direct contact with animals' transmission. The subtyping approach does not apply to any of these hazards, and the applicability of remaining methods varied between parasites.
We concluded that the comparative exposure assessment approach is the most appropriate method to attribute disease by all considered chemical hazards to sources. Given availability of data, this approach is simple to apply. Epidemiological studies, particularly cohort studies, have been undertaken for some of these chemicals, and a review of these could be useful for source attribution. In case of lack of data, an expert elicitation was presented as an alternative for all the hazards.
In addition to the estimation of the proportion of the burden of a disease that is foodborne, expert elicitations may be useful to extrapolate source attribution estimates from a given region/country to geographic areas for which no data to apply the recommended method are available. The availability of data for source attribution varies substantially between countries and even regions. Frequently, more complete datasets can be found in the developed world, and even developing regions are diverse (e.g., Africa appears to suffer particularly from lack of data). Thus, the development of methods to handle missing data and/or extrapolate source attribution results between countries, regions, or clusters of countries is particularly important. It is, however, important to emphasize that the use of the expert elicitation approach should not discourage the use of the data-based source attribution studies.
Conclusion
All reviewed source attribution methods have advantages and limitations, and these influence their utility to address public health questions. Because the purpose of this review was to make recommendations on the most appropriate method to attribute disease by each foodborne hazard, general drawbacks of the methods are not discussed. However, they are acknowledged, as is the benefit of, when possible, applying more than one source attribution method to answer a food safety question, and compare, validate, or merge obtained results. This approach would strengthen the conclusions on the most important sources of disease, and thus provide more robust evidence to inform risk management decisions.
Footnotes
Disclosure Statement
No competing financial interests exist.