
Abstract
Echinococcosis (hydatidosis) is traditionally endemic in Southeast Europe, Serbia included. In Serbia, echinococcosis is mandatory reportable, and this review analyzes the officially reported data as well as the research data published between 1998 and 2010. Official data on human and animal infections were obtained from the Institute of Public Health of Serbia (IPHS, 2010), and from the Ministry of Agriculture, Trade, Forestry and Water Management (MATFWM) and the Statistical Office, respectively. Published data were obtained by searching the Medline, Scopus, and Google databases using “echinococcosis,” “hydatidosis,” and “Serbia” as key words. In addition, the search included national journals and doctoral theses, as well as conference proceedings. Only Echinococcus granulosus has been reported in Serbia, with a total of 409 cases of human infection officially reported during the observed period as opposed to 820 cases described in clinical studies. No trend in the incidence of infection was shown among adults, but the number of cases in children continuously decreased over the period. Patients were more frequently female and from rural areas. Differences in the geographic distribution of cases were noted, with a lower incidence in the central part of country. Liver disease was by far the most common presentation, but cases of unusual cyst locations have been described. Among domestic animals, sheep were the most highly infected species. A decreasing incidence of echinococcosis in animals has been noted as of the 1970s. Echinococcosis continues to be endemic in Serbia in the 21st century, but despite predictions, neither official data nor those from clinical studies indicate its re-emergence. However, there is gross underreporting. Public health authorities should actively work to increase reporting, as only valid reported data provide an accurate basis for future control plans.
Introduction
E
The first report on echinococcosis in Serbia dates back to 1899, when a review of the first 10 years of activity of the State General Hospital in Belgrade (established in 1889) reported six cases of echinococcosis among a total of 26,748 patients (Subbotić, 1899). Echinococcosis was very rarely diagnosed before World War II (Lalošević et al., 2008), after which the number of diagnosed cases started to increase and, according to the reports of the Institute of Public Health of Serbia (IPHS, 2010), towards the end of the 20th century (in 1997), the incidence was 0.21% per 100,000 inhabitants.
Analysis of the genetic diversity of E. granulosus (sensu lato) in Europe showed that of the six strains recognized in the Mediterranean region (Dakkak, 2010), in Serbia only E. granulosus sensu stricto genotype G1 and E. canadensis G7 were identified in humans, swine, and cattle, and only G1 in sheep (Čolović, 2009; Maillard et al., 2009).
In this review, we analyzed the official reports and published studies on the epidemiology and epizootiology of echinococcosis in Serbia during the last decade. Official data on human infections were obtained from the Reports on Infectious Diseases in Serbia, published annually by the IPHS (
Human Echinococcosis
Epidemiological characteristics
Echinococcosis is mandatory reportable in Serbia. Based on the IPHS reports, a total of 409 cases (26 children and 383 adults) of echinococcosis was reported between 1998 and 2010. The incidence of infection was 0.28–0.63 cases per 100,000 inhabitants (Fig. 1). On the other hand, the clinical studies of echinococcosis published during the study period (Table 1) involved 820 patients, treated only in several leading institutions in Serbia (implying there may have been more). This obviously indicates that underreporting has occurred. Even 51% (383/748) of adult patients and 36% (26/72) of children treated in hospitals were not reported to the IPHS. Irrespective of the absolute numbers of cases, however, and in contrast to what may have been expected, neither official nor study data showed any trend in the incidence of infection in adults. Moreover, in children, there was a trend of decrease in the incidence of infection (Fig. 2). An increase in the incidence of CE has been shown following structural and economical reform in transition countries (Shaikenov et al., 2003; Todorov et al., 1999), and could therefore have been expected in Serbia, which was not only in transition but also a post-war society. However, according to the published data, this was not the case; this could indicate a decreasing environmental risk, which is also supported by the decreasing number of cases in children because cases in children are a result of exposure in the near past.
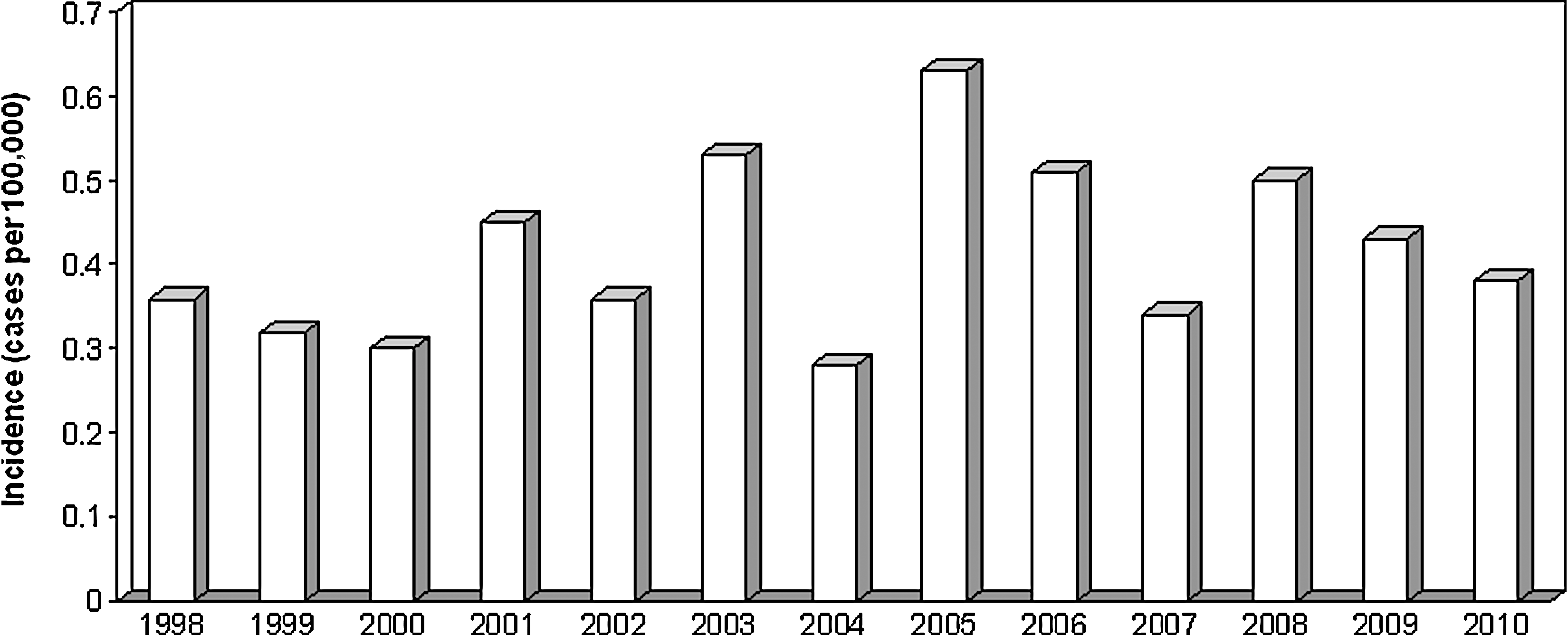
Incidence of echinococcosis in Serbia between 1998 and 2010 (according to official records).

Echinococcosis in children in Serbia between 1990 and 2006 (based on the data from Djuričić et al., 2010).
Years within the study period (1998–2010).
The geographical distribution of CE in Serbia shows very wide variations; thus, the cumulative incidence of reported cases over a 10-year period (2001–2010) ranged from 0.46 cases per 100,000 in the central part of country, and up to 39.0 cases per 100,000 in the south. In the Belgrade area (approximately 2,000,000 inhabitants), which is the most urban area of the country around the capital city, the cumulative incidence was on the low side (1.3 cases per 100,000 for 10 years). These data were mapped using Geographical Information Systems (ARC GIS 10.0; Esri, Redlands, CA), and spatial analysis was performed using the regularized spline method (Fig. 3). It is interesting that some areas with the highest and the lowest incidence of CE were in close proximity. Geographical mapping also provided visualization of the incidence in Serbia as part of a larger picture of the epidemiology of CE in the Balkan region, which was higher in regions bordering with countries with a higher infection rate and lower in regions bordering with countries with a lower infection rate. According to the World Health Organization (WHO), among the countries neighboring Serbia, the highest annual incidence (per 100,000 inhabitants) between 2001 and 2010 was reported for Bulgaria (range 3.88–9.27), followed by the Former Yugoslav Republic of Macedonia (0.3–1.89), Bosnia and Herzegovina (0.32–1.06), and Croatia (0.23–0.81), whereas the lowest incidence was reported for Hungary (0.05–0.13) (WHO/Europe, 2010). Data for Montenegro and Albania are too insufficient for comparison; although irregular, data for Albania are surprising since for some years no infections whatsoever were reported, whereas in 2010, one of the highest ever regional incidences of infection was established (5.27 cases per 100,000). Data for Romania are unfortunately not available from the WHO, but a recent study has shown an annual incidence of 3.8 cases per 100,000 in western Romania (region bordering with Serbia) between 2004 and 2010 (Calma et al., 2011).

Geographical distribution (spline analysis) of echinococcosis in Serbia between 2001 and 2010 (according to official records).
The data reported to the IPHS show that most patients (58%) were above 50 years of age (Fig. 4). We have analyzed (chi-square 2×2 tables) the proportion of male and female patients according to the total male and female populations for the particular years as provided in the Statistical Yearbooks of Serbia. Although women were infected significantly more often (68%, p<0.000), both overall and in each year, it is interesting that no gender differences were established in the younger age groups (between 1 and 39 years; p=0.402), whereas women above 40 were infected significantly (p<0.000) more frequently. Data from clinical studies also showed the predominance of female patients, with the exception of the study on albendazole treatment of CE (Jevtić et al., 2008) in which male subjects predominated; this is not surprising since the study was conducted in a military hospital. All clinical studies showed a 54–60% predominance of patients from rural areas. These results are similar to data from the neighboring countries. In Bulgaria, the incidence of infection was higher in rural residents and in women, while the incidence peak occurred between the fourth and seventh decades of life (Todorov et al., 1999 ). In western Romania, there was a slight predominance (52.7%) of patients above 40, 62.1% cases were women, and the incidence of infection was higher in rural areas (Calma et al., 2011).
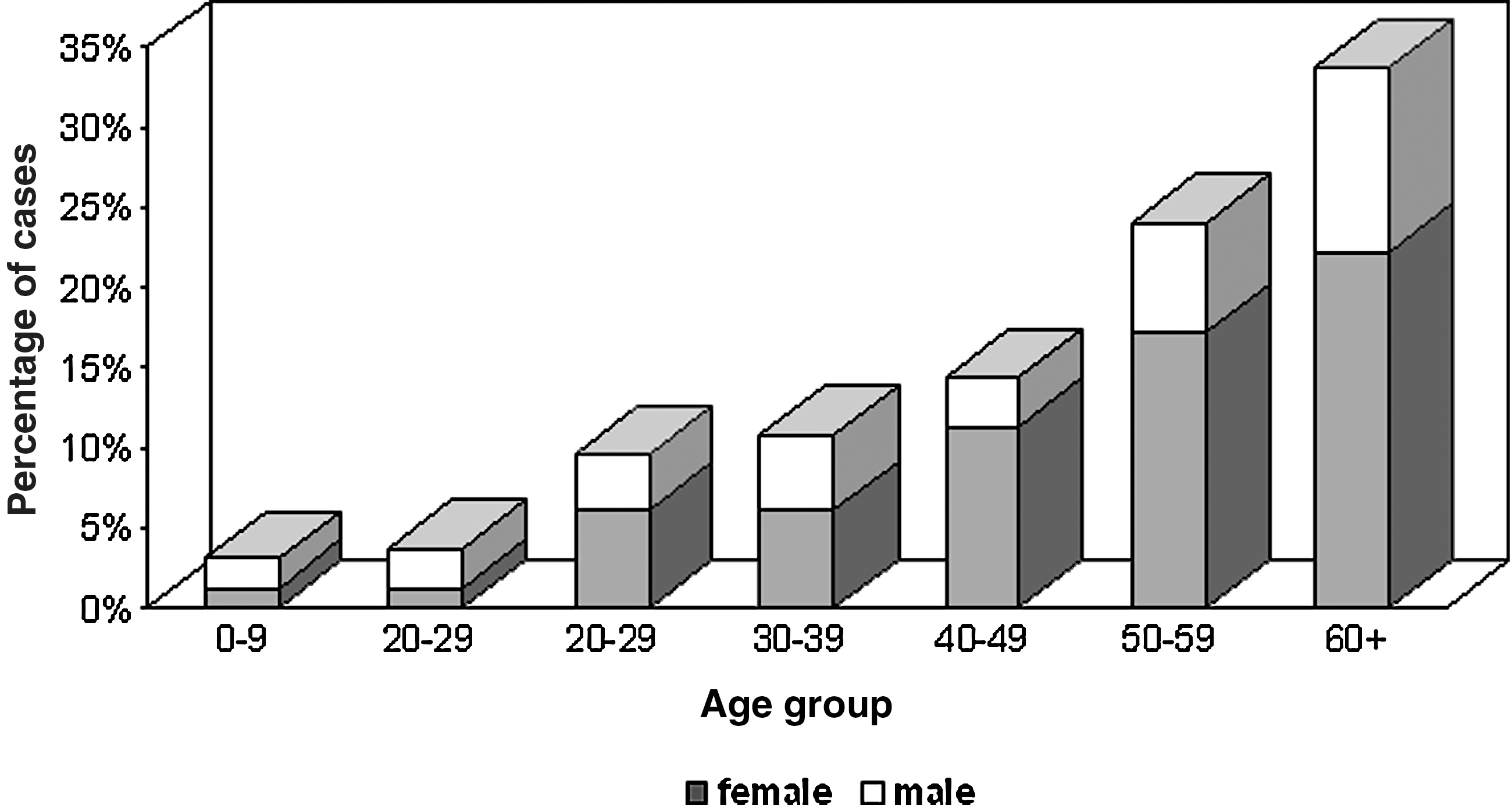
Age and gender distribution of echinococcosis in Serbia between 1998 and 2010 (according to official records).
Prevalence of human and domestic animal infection depends on the level of contamination of the environment, which thus reflects the incidence of dog infection. Above 85% of the patients with liver CE owned a pet dog (55% also owned a cat), but CE in other family members was acknowledged only by 2% of patients (Basarić, 2007). This indicates that individual behavior with dogs, pet or stray, was more important than whether the person owned a pet dog. In a study of genetic diversity of the E. granulosus strains isolated in Serbia, 53% of patients did not have contact with dogs or other domestic animals (Čolović 2009).
Clinical characteristics
Among the cyst localizations, official reports for a 7-year period (2004–2010) showed liver cysts in 68%, lung cysts in 8%, and a non-specified localization in 24% patients. In clinical studies, liver CE was also the most common, with 61% in children and 70% in adult patients (Djuričić et al., 2010; Jevtić et al., 2008). Multiple cysts (2–13 cysts) were diagnosed in 30–33% of the patients (Basarić, 2007; Ćulafić et al., 2007). Extrahepatic CE was described in practically all organs (spleen, lungs, diaphragm, urine bladder, suprarenal gland, intestines, kidney, heart, pancreas abdominal wall omentum, and peritoneum) (Basarić, 2007; Ćulafić et al., 2007; Jevtić et al., 2008). In a study of spleen CE, cysts were localized only in the spleen in 70% of the patients, while in the remaining 30% the liver was involved as well (Ćulafić et al., 2010).
Although the lungs were the second most common localization with 8% of all cases, few clinical data are available. Two cases of isolated pulmonary involvement were reported: one of a solitary cyst with eosinophil perifocal pneumonia (Đurić et al., 2000), and the other of disseminated pulmonary echinococcosis radiographically mimicking metastatic lung disease which regressed after 9 months of albendazole treatment (Milić et al., 2007), both in young males, aged 18 and 27, respectively. Interestingly, in the study of CE in children, cyst localization in the lungs was more frequent in boys (66%) and in the liver in girls (55%) (Djuričić et al., 2010).
Cerebral echinococcosis is extremely rare in Serbia. Although not studied per se, neither the study of Basarić (2007) involving a total of 1016 patients nor the study of Djuričić et al. (2010) involving 149 children, all operated for CE, reported a single case of cerebral CE. Moreover, a study of bioptic samples of the brain and meninges of 4,987 patients with craniotomy between 2000 and 2004 revealed only three cases of cerebral echinococcosis, of which two were adult patients with a solitary cyst each and one a 12-year-old boy with two cysts (Gazibara, 2005).
Several cases of rare cyst localizations, specific symptoms, or complications were reported (Table 2). Interestingly, the first ever description of an unusual cyst localization is, to the best of our knowledge, the report of a hydatid cyst in the buccal muscle published in Serbia back in 1903 (Petrović, 1903).
The prognosis was generally good; no CE-caused deaths were officially reported. However, lethal CE was described in one case (Ivanović-Krstić et al., 2002) of cardiac cysts localized in the right ventricular wall, right atrial wall, tricuspid valve, left atrium and pericardium, as well as in the lungs. Surgical treatment was opted out because of the risk of cardiac perforation, and treatment with albendazole was unsuccessful. Eventually, death due to systemic involvement of the lungs, liver, and central nervous system ensued. Death as a result of postoperative complications (cardiopulmonary insufficiency or pulmonary embolism) was reported in 20 of 1061 patients (0.02%) with liver cysts (Basarić, 2007) and in one of 20 patients with splenic cysts (Ćulafić et al., 2010).
Echinococcosis in Animals
Official data from the MATFWM on CE in domestic animals are based on mandatory reports of the number of infected animals as provided by veterinary services supervising the abattoirs. Using these data and official annual records published by the Statistical Office on the number of animals (per species) slaughtered in abattoirs (RZS, 2010), we have calculated the prevalence of infection presented in Figure 5. A gradual but sustainable decrease in the prevalence of CE during the last decade is evident in all analyzed species (from 14% to 1% in sheep, from 13% to 2% in cattle, and from 9% to 4% in swine). In addition, comparison of these results with earlier data indicates that the incidence of infection has decreased since the 1970s (Savin et al., 1977). However, although the trend itself should not be disputable, the figures for the prevalence of infection in the different domestic animals should be taken with care as they may be limited by several reasons. Firstly, abattoirs do not necessarily report all planned slaughters to the veterinary services; secondly, the data for the years 2007–2008 are missing from the MATFWM database. Finally, but most importantly, as a result of the economic downfall arising from the conflicts of the 1990s, and structural and economical reform during transition from a socialized to market economy (characterized by privatization of state-owned companies, reorganization and/or closing of abattoirs which were previously part of large meat industry companies), the past 20 years have seen a dramatic increase in home slaughtering. However, the situation is currently improving; according to the Statistical Reports of Serbia, whereas in 2001, only 16% of swine, 17% of cattle, and 2% of sheep were slaughtered in abattoirs, after 2005 these figures increased to 30–33% for swine, to 40–47% for cattle, and to 5–7% for sheep. The epizootiological situation in the animals slaughtered at home is unknown, and we cannot say how it may reflect on the prevalence of CE in domestic animals in Serbia in general. Thus, the reported prevalences may be underestimates.
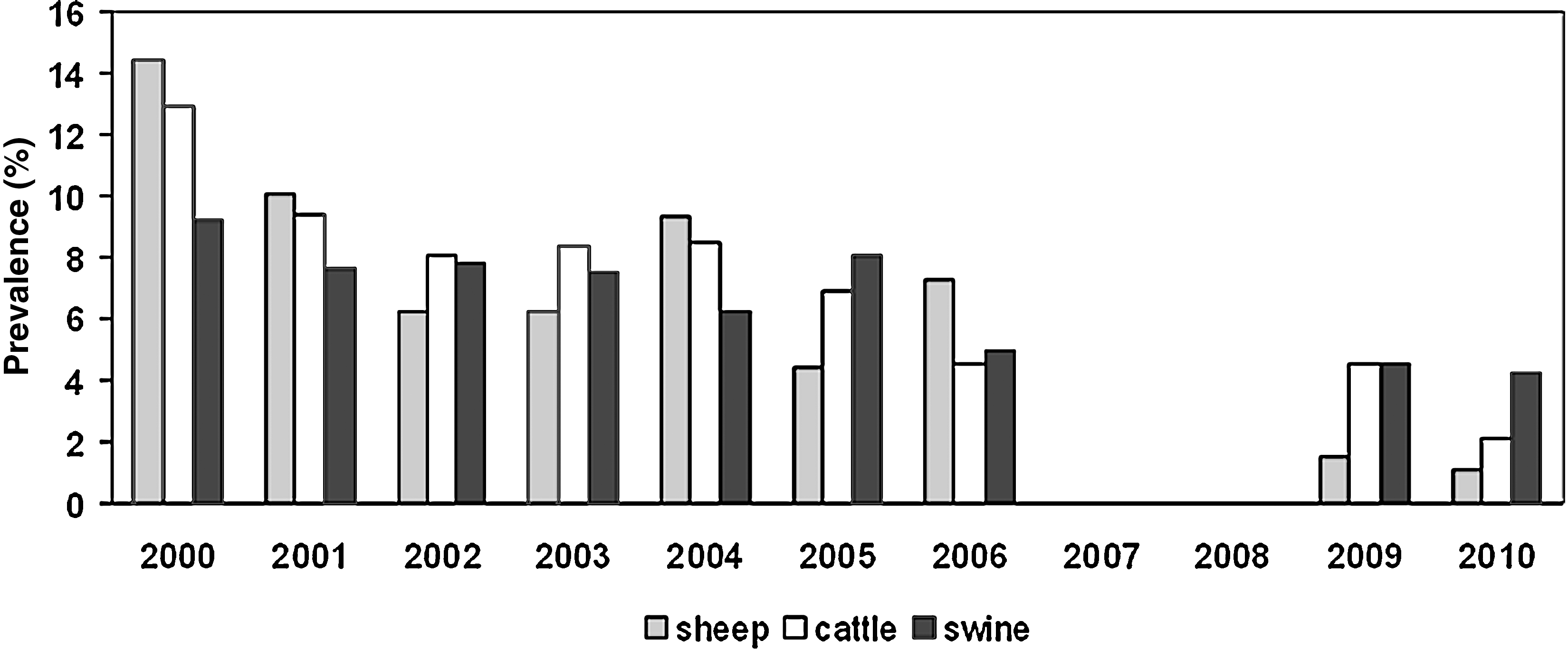
Prevalence of echinococcosis in swine, cattle, and sheep, slaughtered in abattoirs in Serbia between 2000 and 2010.
Echinococcosis in dogs was not studied in the past decade.
Prevention
Prevention of echinococcosis as a zoonotic infection has two aspects: prevention of the spread of infection among animals and prevention of its transmission to humans. Legally bounding plans of measures for the prevention of echinococcosis, made annually by the MATFWM, include yearly deworming with anti-Echinococcus drugs (prior to antirabic vaccination) of dogs and cats above 3 months of age, and strict care for disposal of their feces the following 2 days by the owners. Control of slaughtered animals, safe disposal of viscera of infected animals by competent personnel, and registration of cases diagnosed in abattoirs are all mandatory. Although these measures have resulted in a continuous decrease in the prevalence of infection of domestic animals over the last decade, better control of their implementation is advisable, especially in a situation of high home slaughtering rates. Recently introduced measures involving identification and registration of domestic animals (Law 91/05) and dogs with known owners (Regulation 115/2005 and 33/2007) may further contribute to the control of CE in the coming years in Serbia. In addition, a national strategy for dealing with dogs without known owners has been implemented in 2009, according to which the formerly widely used method of euthanasia has been replaced by measures that require local administrations to provide annual prevention plans adapted to the local situation (Law 41/09). These measures envisage organization of animal shelters by local administrations (before 2009 most shelters were a result of civic initiative), but the capacities of the existing shelters are currently insufficient, and deworming of sheltered dogs is occasionally not carried out for economic reasons. In Belgrade, shelters now apply the catch-neuter-chip-release strategy (including sterilization, registration, deworming, vaccination, and release of stray dogs) (Regulation BG 37/11). Further positive effects of this strategic switch from euthanasia to sterilization may by expected, as a decrease in the number of stray dogs in Belgrade has already been recorded—from 10,396 in 2005 to 8,500 in 2010. Adoption of similar strategies, including deworming, by all local administrations is expected to lead to better control of CE.
A major conclusion of this review is that, although CE is still endemic in Serbia, neither officially reported nor published research data show its current re-emergence. However, as shown above, there is gross underreporting. For a prevention strategy to be adequate, valid data on the incidence of infection as well as on its geographic distribution are a prerequisite. On the other hand, a high number of reported cases from less developed regions of Serbia and significantly more cases from rural areas clearly show that local health services are apt to recognize the disease, a fact that underlines underreporting itself as the main obstacle. To reverse the situation, information campaigns on the importance of reporting are needed for both the medical and veterinary communities, coupled with strict surveillance by the relevant public health authorities. This is all the more important as it is the healthcare and veterinary personnel that are expected to carry out systematic community education on the measures to prevent echinococcosis at the population level.
Footnotes
Acknowledgments
The study was financially supported by the Ministry of Education and Science of Serbia (grant for project III 41019).
Disclosure Statement
No competing financial interests exist.