
Abstract
Listeria monocytogenes infection (listeriosis) is an uncommon but severe foodborne illness that affects mainly individuals with recognized underlying conditions: the elderly, immunocompromised individuals, and pregnant women and their fetuses. The aim of this study was to obtain epidemiological data on cases of listeriosis occurring in Portugal from 2008 through 2012, collected in hospitals on a voluntary basis. L. monocytogenes isolates were characterized by genoserotyping by multiplex polymerase chain reaction, DNA macrorestriction pulsed-field gel electrophoresis (PFGE), and determination of minimal inhibitory concentration (MIC, μg/mL) for 12 antibiotics. During this period, 203 cases of listeriosis were detected. The annual incidence rate observed ranged from 0.2 to 0.7 cases per 100,000 inhabitants. Nineteen cases (9.5%) corresponded to maternal/neonatal (MN) infections. The mean age of the nonmaternal/neonatal (non-MN) cases with documented age was 59 years, and 46.4% occurred in patients aged over 65 years. The majority of listeriosis cases were caused by genoserogroup IVb isolates, and PFGE analysis revealed a high molecular diversity, suggesting that most were sporadic. Nevertheless, several clusters of isolates presenting different geographic and time distributions were detected. The incidence of antibiotic-resistant isolates of L. monocytogenes was low but significantly higher than in previous years (2003–2007). The implementation of a national surveillance system monitoring the incidence of listeriosis and antimicrobial resistance of strains would be most valuable, allowing identification of sporadic and outbreak cases, to detect general trends in antibiotic susceptibilities, and potentially identify food sources of clinical strains.
Introduction
L
The European Food Safety Authority (EFSA) and the European Centre for Disease Prevention and Control (ECDC) reported an overall European Union (EU) notification rate of 0.41 cases of invasive listeriosis per 100,000 population in 2012 (EFSA, 2014). Although its incidence was relatively low, when compared to other foodborne illnesses such as campylobacteriosis (55.49 per 100,000 population) or salmonellosis (28.6 cases per 100,000 population), listeriosis represented the most severe human disease in terms of hospitalization, with the highest case fatality rate (17.8%) of all the zoonotic diseases under EU surveillance (EFSA, 2014). In Portugal, an active surveillance program for listeriosis does not exist. Nevertheless, the incidence of this disease was 0.14 cases per 100,000 population in 2003 (Almeida et al., 2006), and 0.23 cases per 100,000 population in 2007 (Almeida et al., 2010), based on information from voluntary reporting.
The aim of this study was to obtain epidemiological data on cases of listeriosis occurring in Portugal from 2008 through 2012. Isolates of L. monocytogenes were collected from voluntary collaborating hospitals and were characterized by (1) genoserotyping by multiplex polymerase chain reaction (PCR); (2) DNA macrorestriction pulsed-field gel electrophoresis (PFGE); (3) and determination of minimal inhibitory concentration (MIC, μg/mL) of 12 antibiotics.
Materials and Methods
Case definition and data collection
Listeria monocytogenes isolates were collected from 25 volunteer hospitals (the major hospitals in the country), covering ca. 90% of the population (Portuguese National Institute of Statistics,
Incidence of disease was calculated by dividing the number of cases that occurred during 1 y by the estimated average Portuguese population obtained from the Portuguese National Institute of Statistics (
Isolate characterization
Species confirmation was performed by carbohydrate fermentation (rhamnose, xylose, and mannitol) and Christie Atkins Munch-Petersen (CAMP) test. Confirmed isolates of L. monocytogenes were stored in tryptic soy broth with 30% (vol/vol) glycerol at −80°C in the culture collection of the Listeria Research Center of Escola Superior de Biotecnologia (LRCESB).
Genoserotyping or PCR grouping
Genoserotyping was determined by PCR grouping with a multiplex PCR as described by Doumith et al. (2004) using primers targeting fragments of genes lmo0737, ORF2819, ORF 2110, lmo1118, and prs (MWG-Biotech, Muenchenstein, Switzerland). PCR was performed in an Eppendorf thermocycler (Eppendorf, Hamburg, Germany) and PCR products were resolved on a 2% agarose gel containing 0.5 μg/mL of ethidium bromide (Eurobio, Courtaboeuf, France) and visualized and photographed under an ultraviolet transilluminator (Bio-Rad Gel Doc 2000™ imaging system, Bio-Rad Laboratories, Milan, Italy). This assay differentiates five major subtypes, each representing more than one serotype: genoserogroup IVb (serotypes 4b, 4d, and 4e), genoserogroup IIa (serotypes 1/2a and 3a), genoserogroup IIb (serotypes 1/2b, 3b, and 7), genoserogroup IIc (serotypes 1/2c and 3c) and genoserogroup IV (serotypes 4a and 4c).
DNA-macrorestriction by PFGE typing
PFGE typing was performed according to the standard CDC PulseNet protocol (Graves et al., 2001) using the restriction enzymes ApaI (MBI, Fermentas, Burlington, Canada) and AscI (New England Biolabs, Ipswich, MA) and a CHEF Mapper XA (Bio-Rad Laboratories, Hercules, CA). PFGE images for individual isolates were processed to enhance contrast and reduce background. Similarity clustering was performed with the GelCompar software (Applied Maths, Sint-Martens-Latem, Belgium). Cluster analysis of the individual or combined PFGE pulsotypes was done by the unweighted-pair group method with average linkages, using the Dice coefficient to analyze the similarities between PFGE types. Classification of isolates into different ApaI and AscI patterns was visually validated, and pattern data were used to assign combined PFGE types to each isolate, designated by numbers. PFGE types obtained were compared with PFGE types of clinical isolates collected between 1994 and 2007 and included in the LRCESB database.
Antimicrobial susceptibility by microdilution-agar assay
Representatives of the main classes of antibiotics used in both human and animal medicine were selected for this study. Each test was carried on Mueller-Hinton agar (MHA; BioMérieux, Marcy l'Etoile, France) with cation adjusted for penicillin G (Sigma, Steinheim, Germany) and ampicillin (Fluka, Steinheim, Germany) and on MHA for the other 10 antibiotics: vancomycin (Fluka), chloramphenicol (Fluka), nitrofurantoin (Sigma), trimethoprim/sulfamethoxazole (SXT, Sigma), erythromycin, tetracycline, ciprofloxacin, streptomycin, gentamicin, and rifampicin (kindly supplied by the company Labesfal, Tondela, Portugal). MIC for each antibiotic was evaluated by the agar microdilution method using MHA supplemented with 3% (vol/vol) of lysed horse blood, as previously reported (Barbosa et al., 2013). For all antimicrobials, Escherichia coli ATCC 25922 and Enterococcus faecalis ATCC 29212 were used as quality control bacteria for MIC as recommended by Clinical and Laboratory Standard Institute (CLSI, 2007), formerly National Committee for Clinical Laboratory Standards (NCCLS, 2002). Apart from penicillin and ampicillin, for which specific breakpoints for Listeria susceptibility testing are defined by the CLSI, in the present study, others breakpoints used for the agar dilution method were those recommended by the CLSI criteria for veterinary pathogens or staphylococci as previously reported by Conter et al. (2009).
Statistical analysis
An analysis of variance was carried out to test the effect of time (2008–2012) on the MICs of the antibiotics investigated. All calculations were carried out using the software KaleidaGraph (version 4.04, Synergy Software, Dubai, UAE). Data were analyzed according to contingency tables (cross-tabulation) to assess dependency between serotypes of the isolates and resistance/susceptibility.
Results
Incidence and case fatality rate of listeriosis in Portugal
From 2008 through 2012, 203 cases of human invasive infection by L. monocytogenes were identified. Detailed information regarding each notified case is available in Supplementary Table S1 (Supplementary Data are available online at
Cases per 100,000 population.
CSF, cerebrospinal fluid; MN, maternal/neonatal cases; non-NM, nonmaternal/neonatal cases; N/A, information not available.
The overall annual incidence of listeriosis remained relatively constant in 2008, 2009, and 2012 (0.2, 0.2, and 0.3 cases per 100,000 inhabitants, respectively), but was higher in 2010 and 2011 (0.5 and 0.7 cases per 100,000 inhabitants, respectively). Among the 203 listeriosis cases recorded between the studied period, six MN and 49 non-MN cases had a fatal outcome; thus, the overall average case fatality rate observed was 31.6% and 26.6%, respectively.
Isolates characterization: genoserogroup and PFGE typing
Molecular genoserotyping identified 158 (77.8%) isolates belonging to serogroup IVb, 30 (14.7%) isolates belonging to serogroup IIb, and 15 (7.4%) isolates belonging to serogroup IIa (Table 1). Pregnancy-related cases were associated only with genoserogroup IVb (13 cases) and genoserogroup IIb (5 cases).
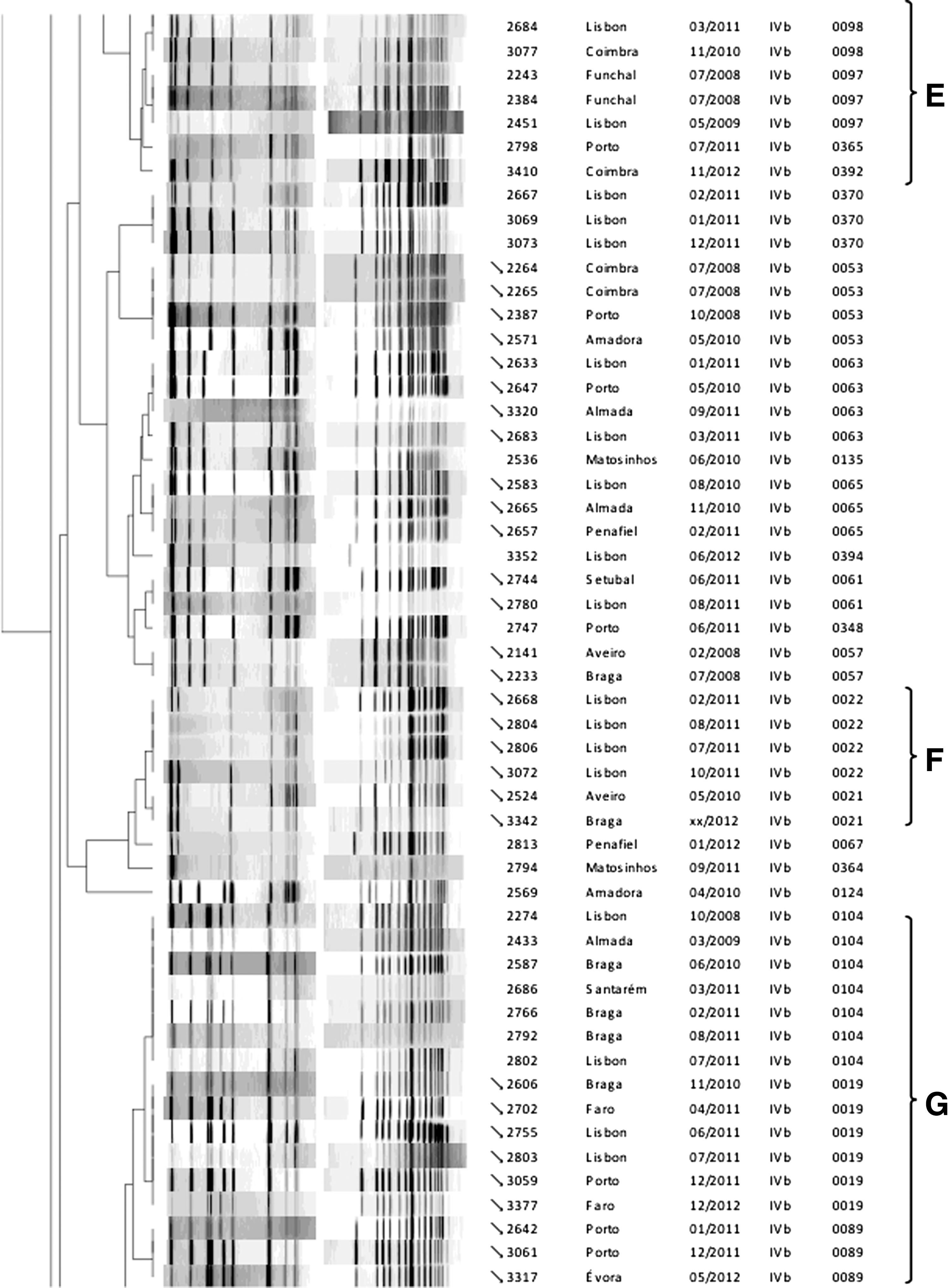
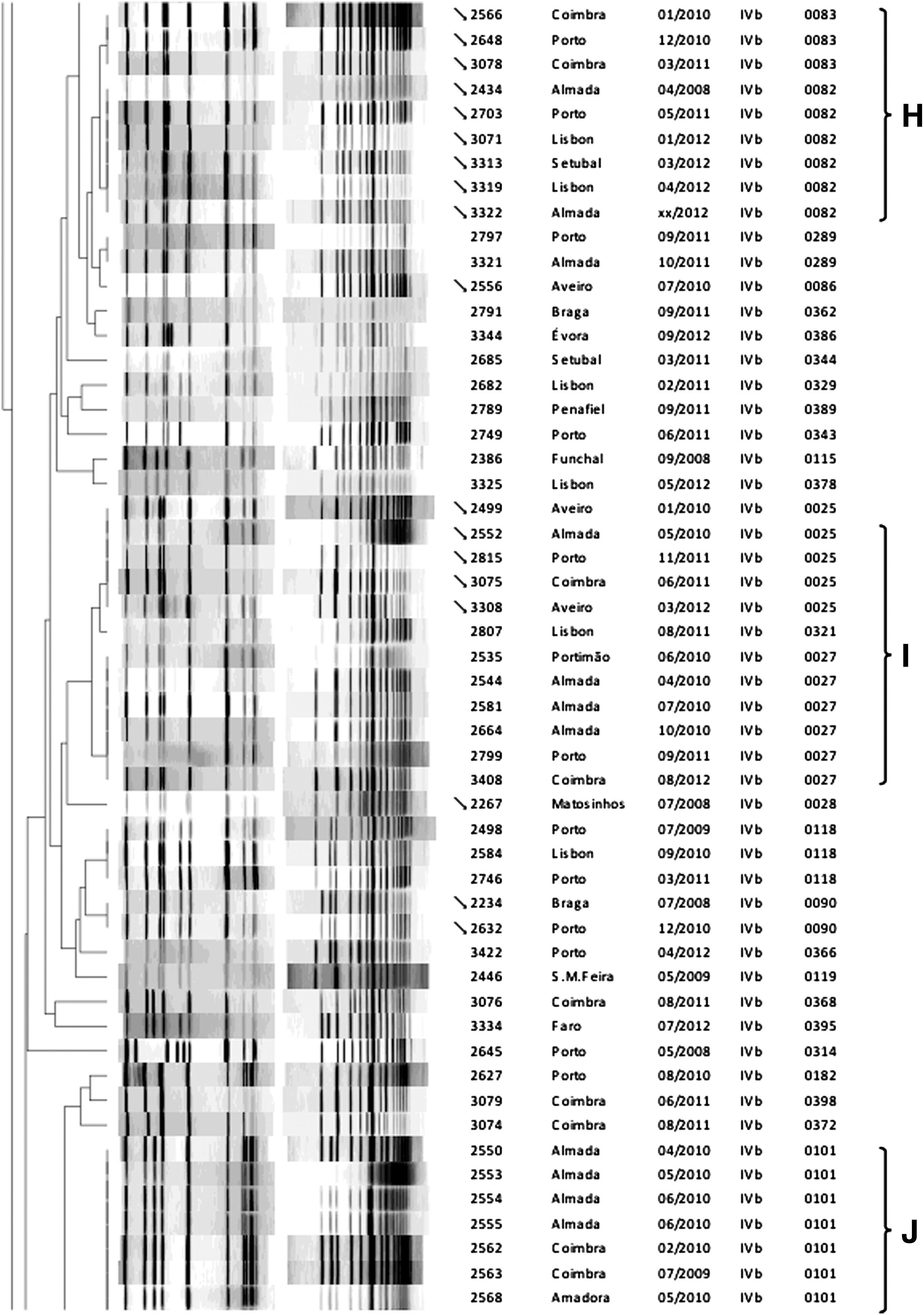
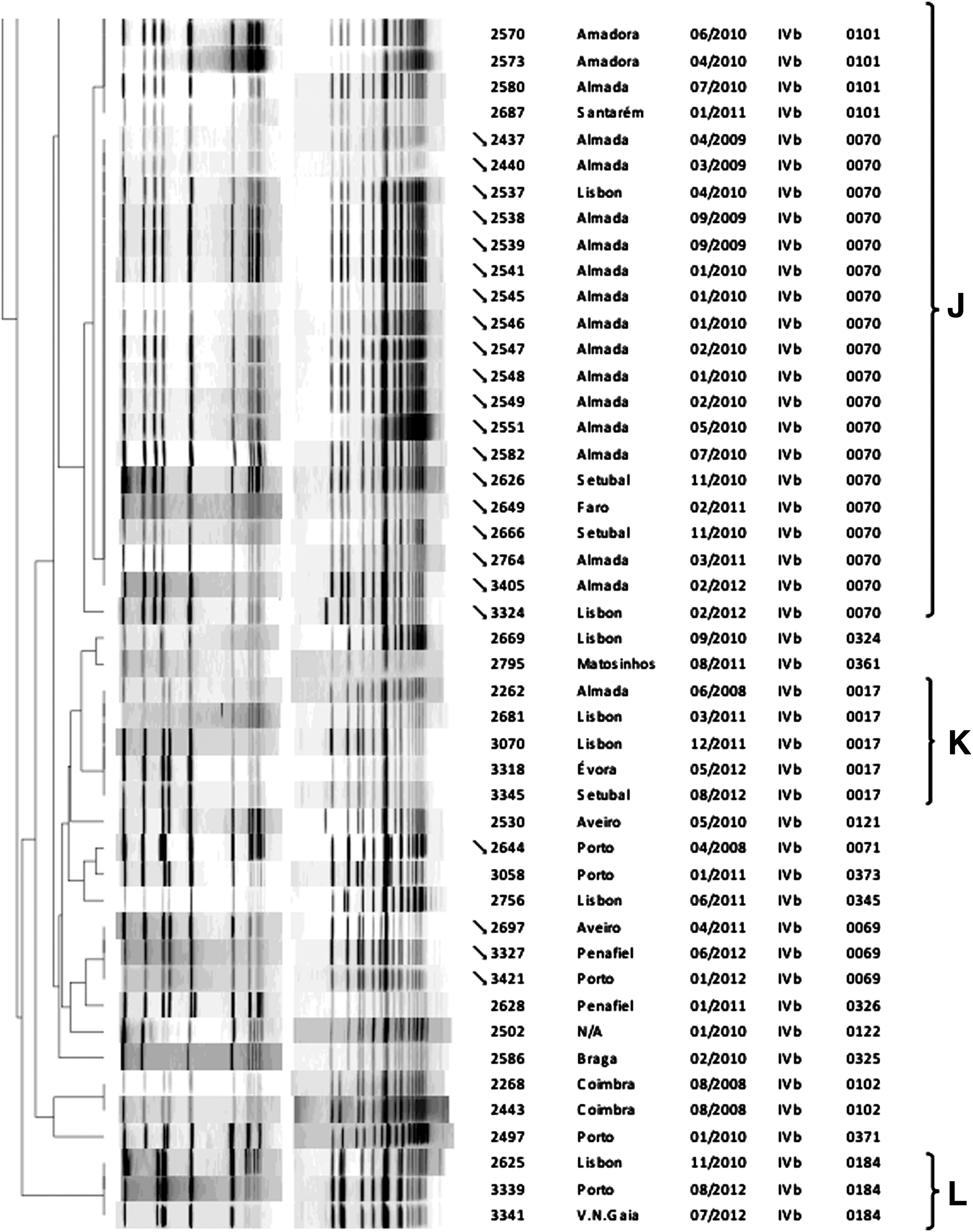
PFGE typing yielded a total of 91 PFGE types, based on combined analysis of AscI and ApaI patterns (Fig. 1). Fifty-four PFGE types (59.3%) were sporadic, occurring only once, namely: 6/9 of genoserogroup IIa; 10/16 of genoserogroup IIb; and 38/66 of genoserogroup IVb. The remaining 37 PFGE types contained 2 or more strains that presented indistinguishable AscI and ApaI patterns. Twenty-six PFGE types have been previously detected in isolates recovered from human clinical cases occurred between 1994 and 2007 (Fig. 1). Thirty-two clusters including 2 or more isolates with indistinguishable or very closely related (>96%) PFGE types were identified. Twelve of these clusters (A–L, highlighted in Fig. 1) included L. monocytogenes isolates recovered from unrelated clinical cases that occurred in the same hospital location, over short periods of time apart.
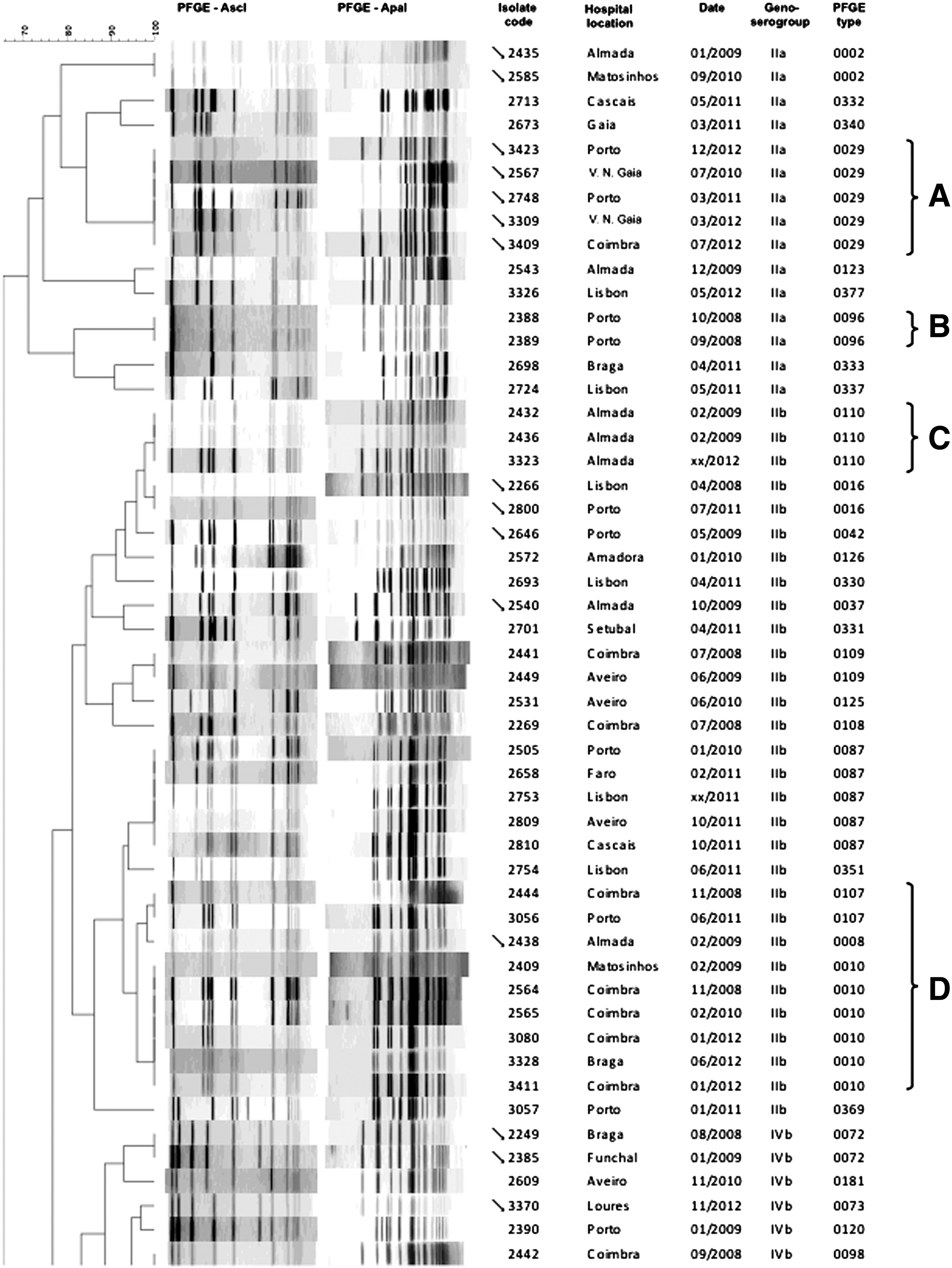
Pulsed-field gel electrophoresis (PFGE) types obtained with restriction enzymes AscI and ApaI of 203 Listeria monocytogenes isolates collected from human listeriosis cases occurred in Portugal, 2008–2012. Letters A to L indicates major clusters that include, at least, two isolates recovered from clinical cases that occurred in the same hospital location, over short periods of time apart. → indicates PFGE types previously detected in isolates recovered from human clinical cases that occurred in Portugal between 1994 and 2007.
Antimicrobial susceptibility
Table 2 shows the MIC90 and MIC50 values determined for L. monocytogenes isolates collected from 2008 to 2012. All the isolates were susceptible to ampicillin, the preferred agent to treat listeriosis. Resistances to ciprofloxacin (n=49), rifampicin (n=28), nitrofurantoin (n=84), and to streptomycin (n=118) were observed. Twenty-nine isolates (14.3%) were resistant to 2 or more antimicrobials of different classes. No significant differences (p>0.05) were found between antibiotic resistance and genoserogroup, except for rifampicin, which present higher MIC values for serogroup IVb.
Trimethoprim-sulfamethoxazole in the ratio 1:19. Breakpoints are expressed as the trimethoprim concentration.
MIC, minimum inhibitory concentration; SXT, sulfamethoxazole.
Discussion
Listeria monocytogenes is a major foodborne pathogen responsible for high hospitalization and death rates. Implementation of a surveillance system for listeriosis is a critical measure for rapid outbreak detection, identification of sources of contamination, and tracking of transmission routes of L. monocytogenes. In 2012, the EU reported a global incidence rate of 0.41 human listeriosis cases per 100,000 inhabitants across member states; country-specific notification rates were highest in Finland, Spain, and Denmark (1.13, 0.93, and 0.90 cases per 100,000 population, respectively), and the lowest in Romania (0.05 cases per 100,000 population) (EFSA, 2014). Despite the EU requirement for all Member States to notify cases of human listeriosis to EFSA, in this report no notification data are available for Portugal as listeriosis is not a notifiable disease and no national surveillance system is implemented in that country. The annual incidence of listeriosis in 2012 was 0.3 cases per 100,000 inhabitants: higher than the values observed in 2003 and 2007 (0.14 and 0.23 cases per 100,00 inhabitants, respectively) (Almeida et al., 2010), and lower than the European global incidence in 2012. A slowly increasing trend was observed in the number of listeriosis cases reported in the EU between 2008 and 2012 (EFSA, 2014). Given that patient data and strains used in this study were collected in hospitals across the country on a voluntary basis, the true number of cases reported is expected to be underestimated. Furthermore, invasive listeriosis is an infrequent disease, with clinical symptoms difficult to identify; thus, some of the cases that actually occur may not be diagnosed (Scallan et al., 2011). The number of pregnancy-associated infections was relatively low (9.5%) when compared to values observed in other countries with implemented active surveillance systems for listeriosis (approximately 17%) (Goulet et al., 2012; Silk et al., 2012). An underestimation is likely related to undiagnosed cases that occur in the first term of pregnancy. It is also important to highlight that Portugal has one of the lowest fertility rates in the world (UNFPA, 2013). Among the high-risk population groups in Europe, susceptibility of individuals aged >65 y has been reported to be the highest in 2012 (EFSA, 2014). The fact that 46.4% of the total number of cases of listeriosis described here occurred in this age group is noteworthy, as this is an increasing demographic group in Portugal, already representing 19% of the total population (The World Bank;
Although latest-generation DNA sequence-based methods, such as whole genome sequencing, present a higher discriminatory power that allows an exhaustive evaluation of genetic variations between L. monocytogenes strains (Gilmour et al., 2010; Knabel et al., 2012; Schmidt et al., 2014), serotype identification and PFGE typing remain the preferred standard typing methods in routine laboratories for listeriosis surveillance and outbreak detection (de Valk et al., 2005; Sabat et al., 2013). The majority of listeriosis cases were caused by genoserogroup IVb (serotypes 4b, 4d, and 4e) L. monocytogenes strains, followed by genoserogroup IIb (serotypes 1/2b, 3b, and 7) strains, whereas genoserogroup IIa (serotypes 1/2a and 3a) strains were responsible for the lowest number of cases. Other authors, however, have reported serogroup IIa strains more frequently isolated from clinical human cases than serogroup IIb and/or IVb strains (Doorduyn et al., 2006; Knabel et al., 2012; Silk et al., 2012; Mammina et al., 2013; Lopez-Valladares et al., 2014). Serotypes 4b and 1/2b isolates are regarded as potentially more virulent, and are therefore more overrepresented among human listeriosis cases worldwide than serotype 1/2a, overrepresented among food isolates, and linked with more frequent human exposure (Nightingale et al., 2005; Garrido et al., 2009; Orsi et al., 2011). In Portugal, serogroups IVb and IIb L. monocytogenes isolates are reported as the most frequently found in food products (Guerra et al., 2001; Pintado et al., 2005; Leite et al., 2006; Ferreira et al., 2011; Almeida et al., 2013). Genoserogroup IIc was never identified among collected isolates, despite the fact that a minority of clinical cases caused by serotype 1/2c strains have been reported in other countries (Goulet et al., 2008; Mammina et al., 2013). Characterization of L. monocytogenes by PFGE typing revealed a high molecular diversity, suggesting that the majority of the listeriosis cases were sporadic. Nevertheless, several isolates with different geographic and time distributions presented closely related PFGE types, and thus grouped into major clusters. Although this could mean that some PFGE types are more common, and thus widely distributed in the country, a common source of food contamination cannot be ruled out. In fact, a number of studies have demonstrated by molecular subtyping methods that more cases than acknowledged represent outbreaks (Sauders et al., 2003; Clark et al., 2010; Gaulin et al., 2014). One major cluster, Cluster I, grouping 30 listeriosis cases occurred in Lisbon and Vale do Tejo region between January 2010 and February 2012, led to an outbreak investigation, and proved to be linked with consumption of contaminated pasteurized milk cheese (P. Teixeira, 2013, personal communication).
From a public health perspective, this fact stresses the importance of the implementation of an effective surveillance system that assures a prompt notification of the clinical cases (and corresponding epidemiological data), as well as the monitoring of L. monocytogenes in food products. Given the high mortality rate, morbidity, and economic burden associated with listeriosis, it is extremely important to rapidly identify a contaminated food product and remove it from the distribution chain. Molecular subtyping techniques (e.g., routine serotyping and PFGE analysis) are essential to identify contamination sources and transmission routes of this pathogen to humans.
The incidence of antibiotic resistant isolates of L. monocytogenes was low but higher than that observed in Portugal during the period 2003–2007 (Barbosa et al., 2013). With the exception of gentamicin, for all the antibiotics investigated, MIC values were significantly higher (p<0.05). The percentage of isolates resistant to ciprofloxacin increased from 1.0% to 24.5%, to nitrofurantoin from 20.0% to 24.0%, and to rifampicin and streptomycin from 0 to 14.0% and to 59%, respectively (data not shown). While no clinical isolate was found to be resistant to more than 1 antibiotic in the previous study (Barbosa et al., 2013), 14.4% of isolates recovered in the period 2008–2012 were resistant to at least 2 antibiotics of different classes. These results support a slow but emerging antibiotic resistance in L. monocytogenes. Monitoring for antibiotic resistance in strains of L. monocytogenes on a large scale, and assessing the risk of infection by these strains, is therefore highly recommended.
Conclusions
From 2008 through 2012, 203 cases of listeriosis were reported on a voluntary basis by Portuguese hospitals covering ca. 90% of the population. The annual incidence rate ranged from 0.2 to 0.7 cases per 100,000 inhabitants. Most of the cases were sporadic and caused by genoserogroup IVb. Approximately half of the cases occurred in patients aged ≥65 y. Given the demographic changes observed in the population, caused by aging and longer life expectancy, and consequently an upsurge of chronic conditions, more deaths due to listeriosis are expected. Therefore, prevention strategies should be implemented.
Footnotes
Acknowledgments
This work was supported by funding from the National Funds from the Fundação para a Ciência e a Tecnologia (FCT) through project Pest-OE/EQB/LA0016/2013 and from Fundo Europeu de Desenvolvimento Regional (FEDER), under Program ON2 thorough project KLEAR—Knowledge and tools for safety, quality and competitiveness in the food chain (n° NORTE-07-0124-FEDER-000052). Financial support for R.M. and V.F. was provided by FCT through doctoral fellowship SFRH/BD/71704/2010 and postdoctoral fellowship SFRH/BPD/72617/2010, respectively.
Disclosure Statement
No competing financial interests exist.
Members of the Research Team
Centro Hospitalar do Baixo Vouga, Entidade Pública Empresarial (EPE) (Sónia Ferreira, Raquel Diaz, Elmano Ramalheira); Centro Hospitalar do Barlavento Algarvio, EPE; Centro Hospitalar Lisboa Central, EPE (Cristina Marcelo, João Marques, Isabel Daniel, Isabel Peres, Margarida F. Pinto, Odete Chantre); Centro Hospitalar Lisboa Norte, EPE (J. Melo Cristino); Centro Hospitalar de Lisboa Ocidental, EPE (Judite Batista, Teresa Marques); Centro Hospitalar do Porto (Helena Ramos, Paulo Pereira); Centro Hospitalar de Setúbal, EPE (Jesuina Duarte, Luisa Espadinha, Andrea Bernardo, Inês Tapadinhas); Centro Hospitalar do Tâmega e Sousa, EPE (Isaura Terra, Flávio Assunção Mariana Viana); Centro Hospitalar e Universitário de Coimbra—Unidade Hospitalar de Coimbra (UHC) (Luisa Boaventura, Catarina Chaves, Teresa Reis); Centro Hospitalar de Vila Nova de Gaia/Espinho, EPE (Paulo Lopes, Vânia Soares); Hospital Beatriz Ângelo & Hospital de Cascais Dr. José de Almeida (Laura Brum); Hospital de Braga (Maria Alberta Faustino); Hospital de Faro, EPE; Hospital Distrital de Santarém, EPE (Paula Pinto); Hospital Dr. Nélio Mendonça, Madeira (Teresa Afonso); Hospital Espírito Santo de Évora, EPE (Adriana Coutinho); Hospital de Faro, EPE; Hospital Garcia da Horta (José Diogo, Ana Rodrigues, Isabel Nascimento); Hospital Militar de Belém (João Lago); Hospital Pedro Hispano (Maria Antónia Read); Hospital Prof. Doutor Fernando Fonseca (Luisa Sancho, Teresa Sardinha); Hospital de São João, EPE (Tiago Guimarães, Maria Dolores Pinheiro, Manuela Ribeiro); Serviço de Patologia Clínica Hospital CUF Descobertas & CML Dr Germano de Sousa (M. Favila Menezes, M. J. Sousa, J. Germano de Sousa); Serviço de Patologia Clínica (Laboratório de Microbiologia), Hospital de Curry Cabral (Helena Peres, Teresa Pina).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.