
Abstract
Introduction:
Enhancing foodborne disease (FBD) surveillance and improving the timeliness of outbreak detection have been identified as public health priorities. Consumer complaint data have become increasingly useful for FBD surveillance and the detection of outbreaks. Calls to poison centers are a potential source of consumer complaint data. A retrospective analysis of data from the National Poison Data System (NPDS) (2000–2011) was undertaken to evaluate the value of data collected through the United States poison centers for detection of large national outbreaks and recalls.
Methods:
Demographic and clinical data were summarized. Prevalences of FBD calls were calculated and analyzed for time trends. Significant increases in daily call prevalences were identified, and dates of the increases were compared to the announcement of 18 national outbreaks/recalls.
Results:
Over the 12-year period, there were 433,788 unique calls self-reporting a suspected FBD exposure in humans. Overall, daily call prevalences decreased over time. Only about half of callers reported common gastrointestinal clinical effects. Of the 42 identified significant increases in call prevalences, none occurred within 14 days before an outbreak announcement; 7 occurred within 14 days after an outbreak announcement.
Conclusions:
Based on this analysis, there are significant limitations to using self-reported FBD exposures to NPDS as a source of information for FBD surveillance of large national outbreaks and recalls; however, a syndromic approach may yield different results and should be explored. Improved data collection and coordination with public health agencies may improve the ability to use NPDS data to monitor FBD in near real-time, identify potential outbreaks, and improve situational awareness.
Introduction
F
Given the large-scale effect on health, the Centers for Disease Control and Prevention (CDC) has identified reducing FBD as a “Winnable Battle” and cited two areas where action would markedly influence public health: (1) improving knowledge of the incidence, trends, burden, and causes of FBD outbreaks; and (2) improving capacity to detect and respond quickly to FBD outbreaks (CDC, 2013). The CDC Infectious Disease Framework identified several priorities for enhancing FBD surveillance, including improving the collection and communication of timely, accurate, and complete data, as well as improved coordination and information flow between clinicians, clinical laboratories, and public health agencies (Frieden and Khabbaz, 2011).
Currently, FBD surveillance is conducted by >3000 state and local public health agencies under 50 different state laws. Pathogen-specific surveillance systems employ microbiological methods to link cases and trace illnesses to their source, but most reported cases are never linked to an outbreak. Most FBD outbreaks are detected through consumer complaint systems, which are widely used by state and local health departments (Li et al., 2011). Utilizing consumer complaint systems to conduct FBD surveillance offers the benefit of capturing information on all cases, not just those reported to public health officials (Hedberg et al., 2008).
One potential source of consumer complaint data is the American Association of Poison Control Centers (AAPCC) National Poison Data System (NPDS), which contains data about exposure and information calls managed by poison centers (PCs) serving the 50 states, the District of Columbia, Puerto Rico, and U.S. territories (Bronstein et al., 2012). Each day, trained health professionals manage about 11,000 phone calls from U.S. residents, health professionals, and public health officials, and collect standardized data based on caller responses (Bronstein et al., 2012; AAPCC, 2013). NPDS data have been used to monitor trends in critical public health problems such as unintentional overdose of acetaminophen (Bond et al., 2012) and drug abuse (Marsolek et al., 2010; Wilson et al., 2011). While data from the Arizona Poison and Drug Information Center Arizona have been used to identify cases of FBD (Derby et al., 2005), no study has evaluated NPDS data as a potential source of FBD consumer complaint data. Therefore, the purpose of this study was to evaluate the use of NPDS data for surveillance of large national FBD outbreaks and recalls in the U.S.
Materials and Methods
This evaluation utilized NPDS data from calls reporting potential FBD exposures to PCs; data from all callers were not available for this analysis. Complete information was extracted for all calls from 2000 to 2011 coded by the PCs as “food products/food poisoning” in the NPDS database (Table 1). All calls reporting a FBD exposure were included in the data extract, regardless of their plausibility for FBD. Information calls (i.e., callers requesting information with no known exposure) and animal exposures (i.e., callers reporting FBD in animals) were excluded from data analysis.
Within the NPDS database, caller data are de-identified and recorded in a standardized computer format. Self-reported demographic, exposure, and clinical information are collected from each caller using predefined fields. Free-text notes may be recorded by the health professional but are not uploaded into NPDS. For each call, the presence of 131 predefined clinical effects (defined to be signs, symptoms, or laboratory abnormalities) was recorded and categorized as related, not related, or unknown if related. Only clinical effects relevant to FBD (abdominal pain, diarrhea, nausea, vomiting, rectal bleeding, fever, and headache) were summarized in the analysis; it was assumed the caller did not report the clinical effect if it was missing in NPDS. For multiple entries related to a single call, the first record was retained along with clinical effects and outcomes reported across all entries.
Demographic and clinical data were summarized including call date, gender, age, caller location, product implicated, reason for exposure, exposure site, exposure duration, clinical effects, duration of clinical effects, and medical outcome. Descriptive statistics were used to characterize trends in call prevalences over time. Call prevalences were calculated by dividing the number of FBD calls by population estimates from the U.S. Census Bureau's 2000 and 2010 data and the corresponding estimates from the Census Bureau's American Community Survey (U.S. Census Bureau, 2012). Call prevalences were plotted over time, and the Cochran–Armitage trend test was used to assess trend significance (p<0.05) over the 12-year period. State-specific call prevalences were calculated using state-specific census data and were geographically mapped.
CDC's Early Aberration Reporting System (EARS) was used to identify significant increases in daily call prevalences (Hutwagner et al., 1997, 2003). In EARS, users can select one of four Cumulative Sum algorithms to detect significant changes, referred to as anomalies, from short, static, or moving baselines. The healthcare algorithm is recommended for use with patient-reported chief-complaint healthcare data and was selected for this analysis. In this algorithm, a daily call prevalence exceeding 1 SD above the baseline call prevalence is considered an anomaly. Since call prevalence rates may differ on weekdays versus weekends, the baseline call prevalence is calculated using the call prevalences from the prior 28 days for weekdays (i.e., weekdays only, excluding weekends) and the prior 14 days for weekends (i.e., weekends only, excluding weekdays). According to EARS documentation, the shorter baseline period is appropriate when there is known seasonal variation, as in the case of FBD. Since consecutive days of increased call prevalences could artificially inflate the baseline call prevalence, the algorithm excludes the 2 days before the day analyzed from the baseline period.
If NPDS data can be used as a timely and sensitive surveillance system, anomalies in FBD daily call prevalences should precede major outbreaks. Therefore, dates of anomalies were compared to the first public announcement of selected FBD outbreaks (Table 2). The date of first public announcement was determined by searching press releases issued by the U.S. Department of Agriculture, the Food and Drug Administration, and CDC. When no press release could be found, a general internet search was used to find the earliest date of media reports. The number of call prevalence anomalies was evaluated for seasonal trends, and the anomalies occurring within 7, 14, and 28 days before and 7 and 14 days after outbreaks and recalls were tabulated.
Recall due to lack of complete and proper inspection of cattle.
Recall with no associated outbreak.
Data management and statistical analyses were performed using SAS 9.3 (SAS Institute, Cary, NC). The U.S. map of call prevalences was created using ArcGIS (version 10.1; Ersi, Redlands, CA). All other figures were created using R (version 3.0.1). AAPCC's Data Access Committee and Board of Directors approved the data request. The study was exempted by the North Carolina State University's institutional review board.
Results
A total of 479,465 records associated with the AAPCC generic codes “food products/food poisoning” were extracted from NPDS. There were 465,495 unique calls, including information (N=27,821) and exposure (N=437,674) calls, to PCs during the 12-year period (Table 3). Of these, 433,788 were exposure calls for humans. The most frequently reported exposure was “Food Poisoning—Unknown” (39%). Multiple exposures were reported by 11,179 callers (2.6%). Slightly more callers were female (56%) than male (Supplementary Table S1; Supplementary Data are available online at
The most commonly reported exposure site was “Own Residence” (76%), followed by “Restaurant/Food Service” (14%) (Supplementary Table S4). Most (97%) reported an exposure lasting <8 h. The most commonly reported reason for exposure was “Unintentional—Food Poisoning” (64%) (Supplementary Table S5).
Most callers (74%) reported 1 or more of the 131 possible clinical effects, but only about half (54%) reported common gastrointestinal clinical effects (abdominal pain, diarrhea, nausea, and vomiting) (Table 4 and Supplementary Tables S6 and S7). Thirty-two percent of callers reported two or more gastrointestinal clinical effects, but only 5% reported all four. Few callers reported other clinical effects associated with gastrointestinal disease including rectal bleeding, fever, and headache. Most callers had minimal clinical effects and were not followed (55%), or had minimally bothersome clinical effects that resolved rapidly (23%). The duration of clinical effects was missing for most reported callers (78%), although duration is only recorded if the patient is followed and the medical outcome is determined to be at least a minor effect (Supplementary Table S8). The most commonly reported duration of clinical effects was “>8 and ≤24 hours” (8%).
There are 131 reportable clinical effects possible.
Gastrointestinal clinical effects are diarrhea, nausea, vomiting, and abdominal pain.
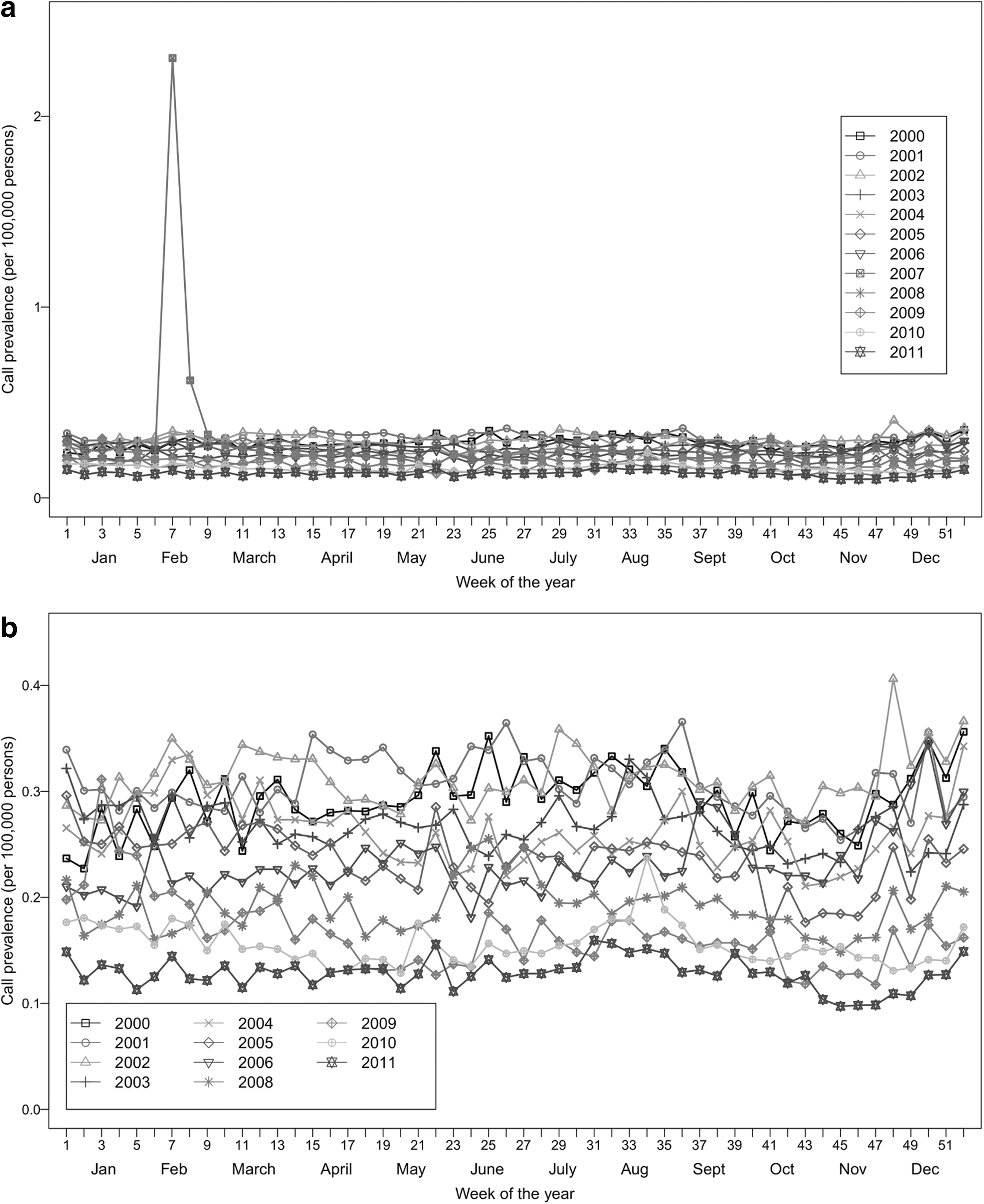
Call prevalences are presented by year in Figure 1. There was a decreasing trend in call prevalences (p<0.001) over the 12-year period. The mean annual FBD call prevalence was 12.3 calls per 100,000 persons (range 6.7–16.2 per 100,000 persons). There were not strong trends in weekly call prevalences, although there was a large increase in call prevalence in February 2007 (Fig. 2a). There were not strong trends in call prevalences when 2007 data was excluded (Fig. 2b). Call prevalences varied by state (Fig. 3), with the Southwest and Northwest having the highest prevalences.
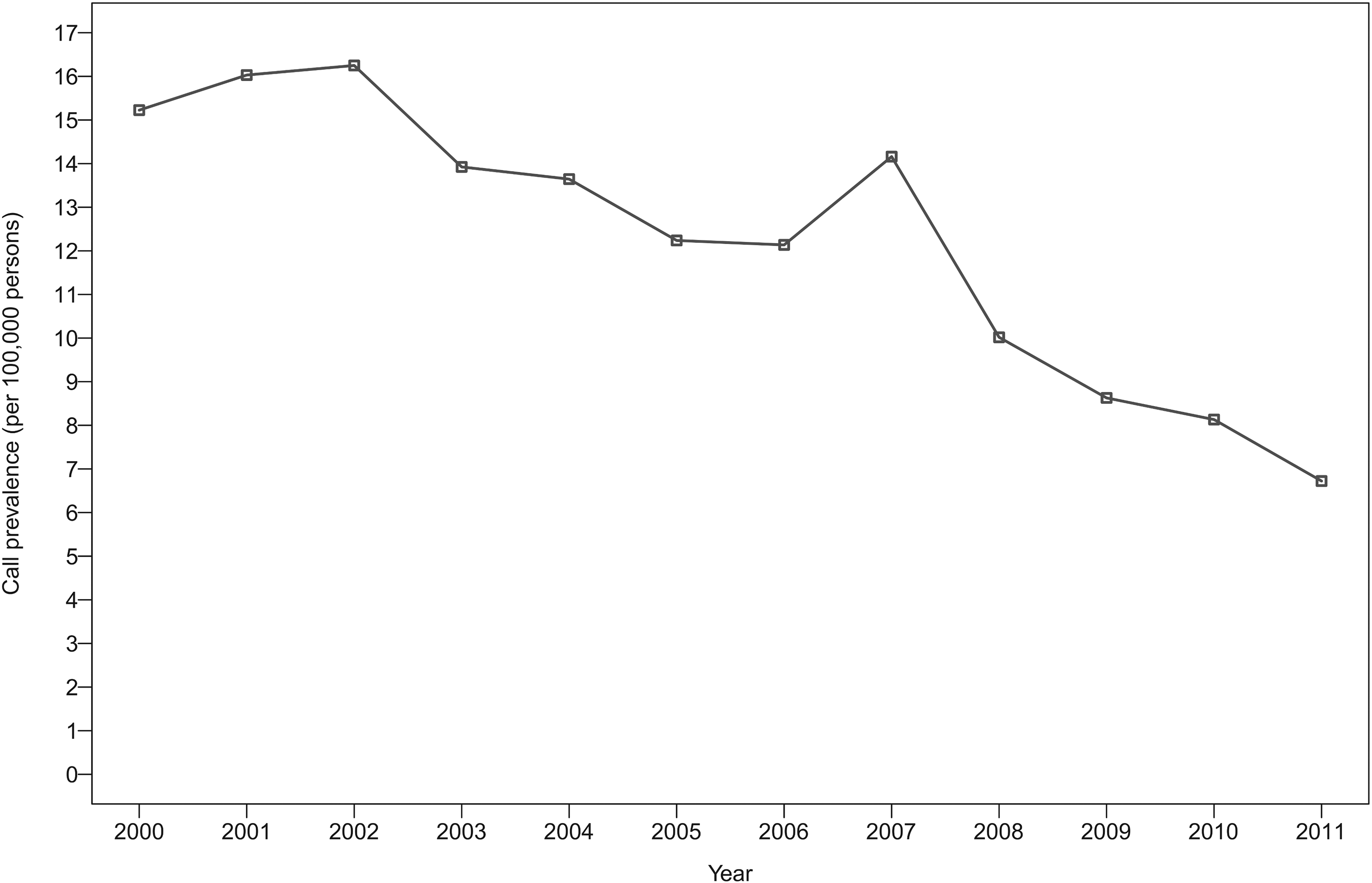
Yearly prevalence of self-reported foodborne disease calls per 100,000 persons reported to U.S. poison centers from 2000 to 2011.
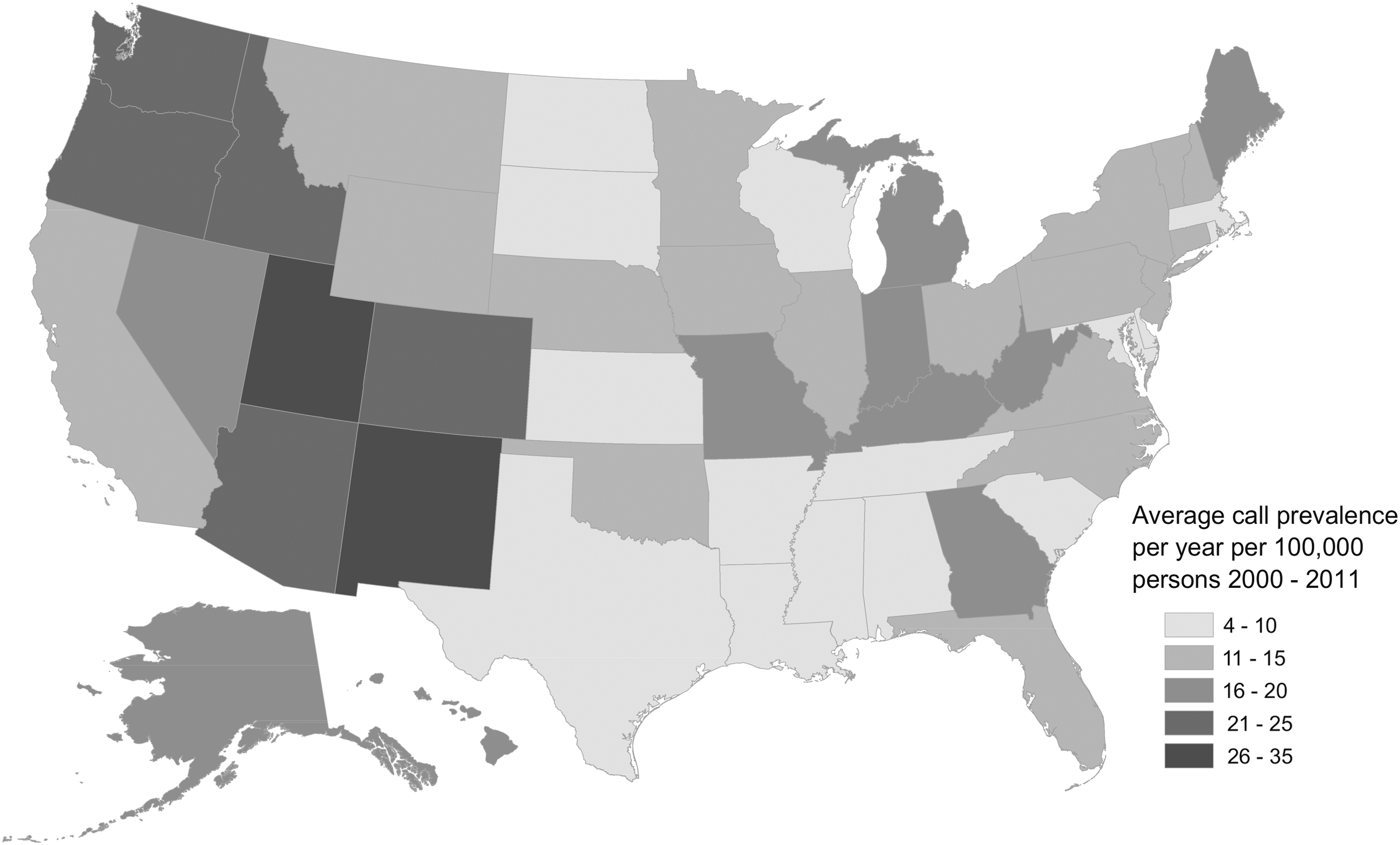
Average yearly prevalence of self-reported foodborne disease calls per 100,000 persons reported to U.S. poison centers by state from 2000 to 2011.
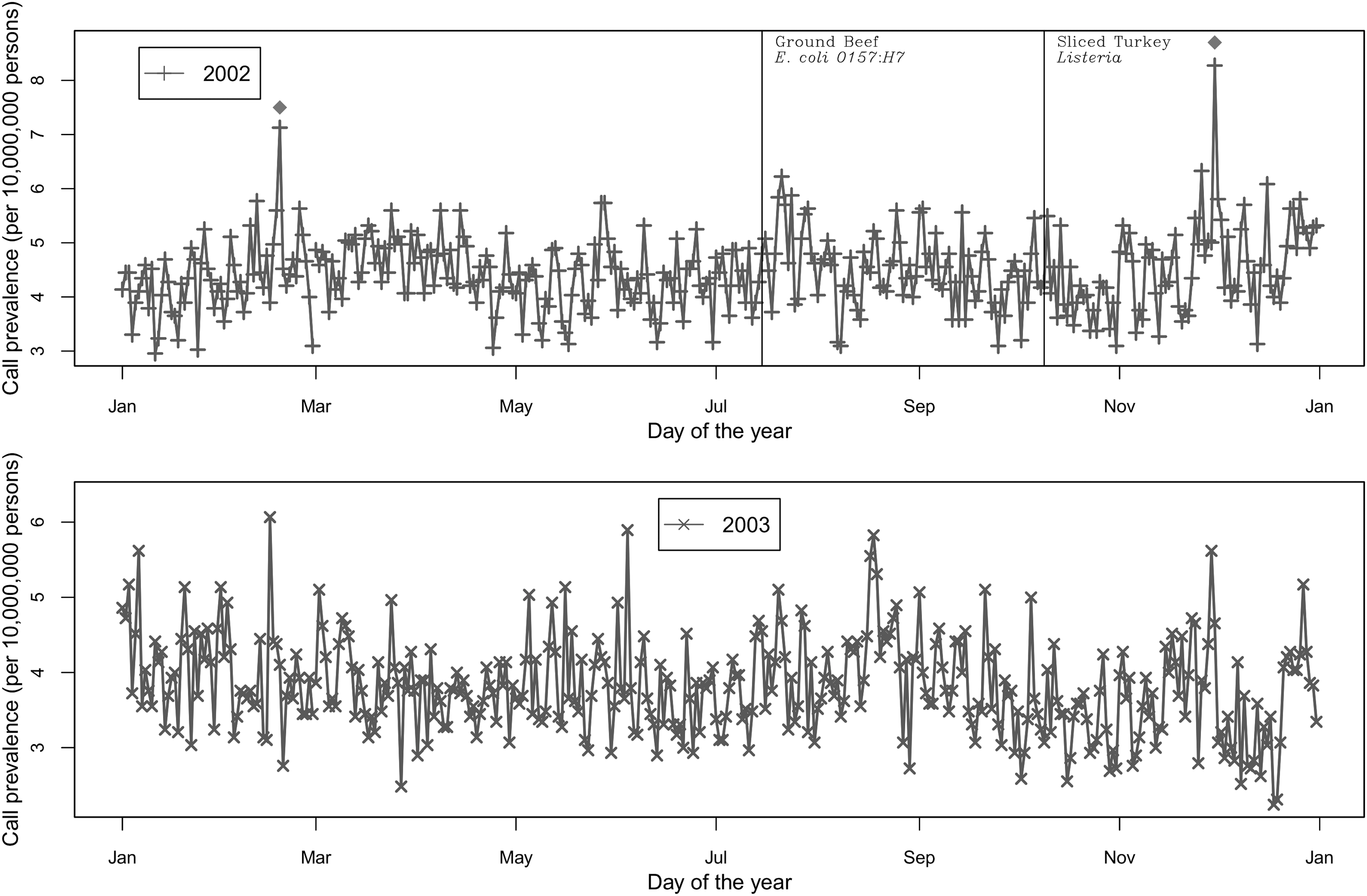
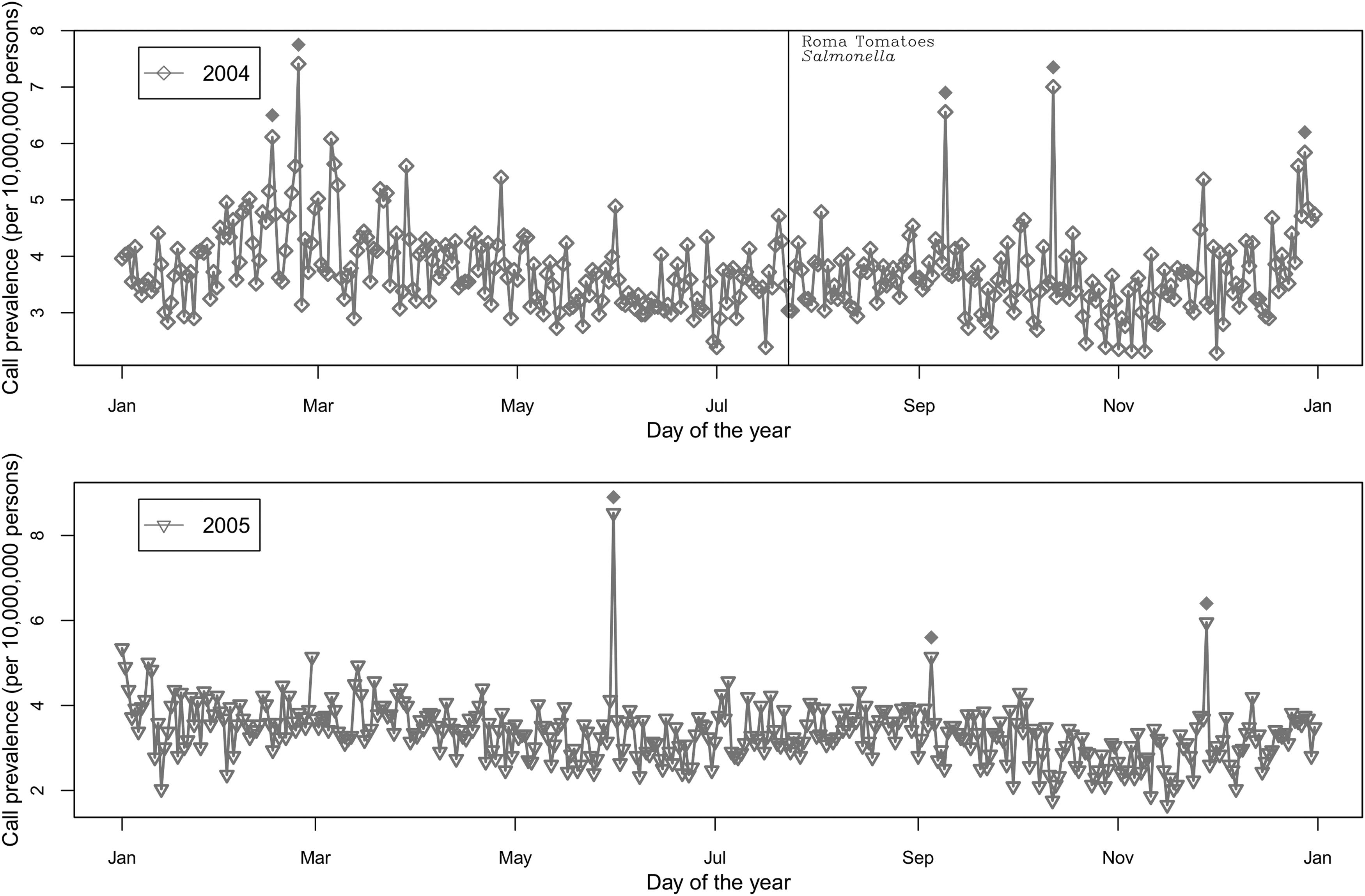
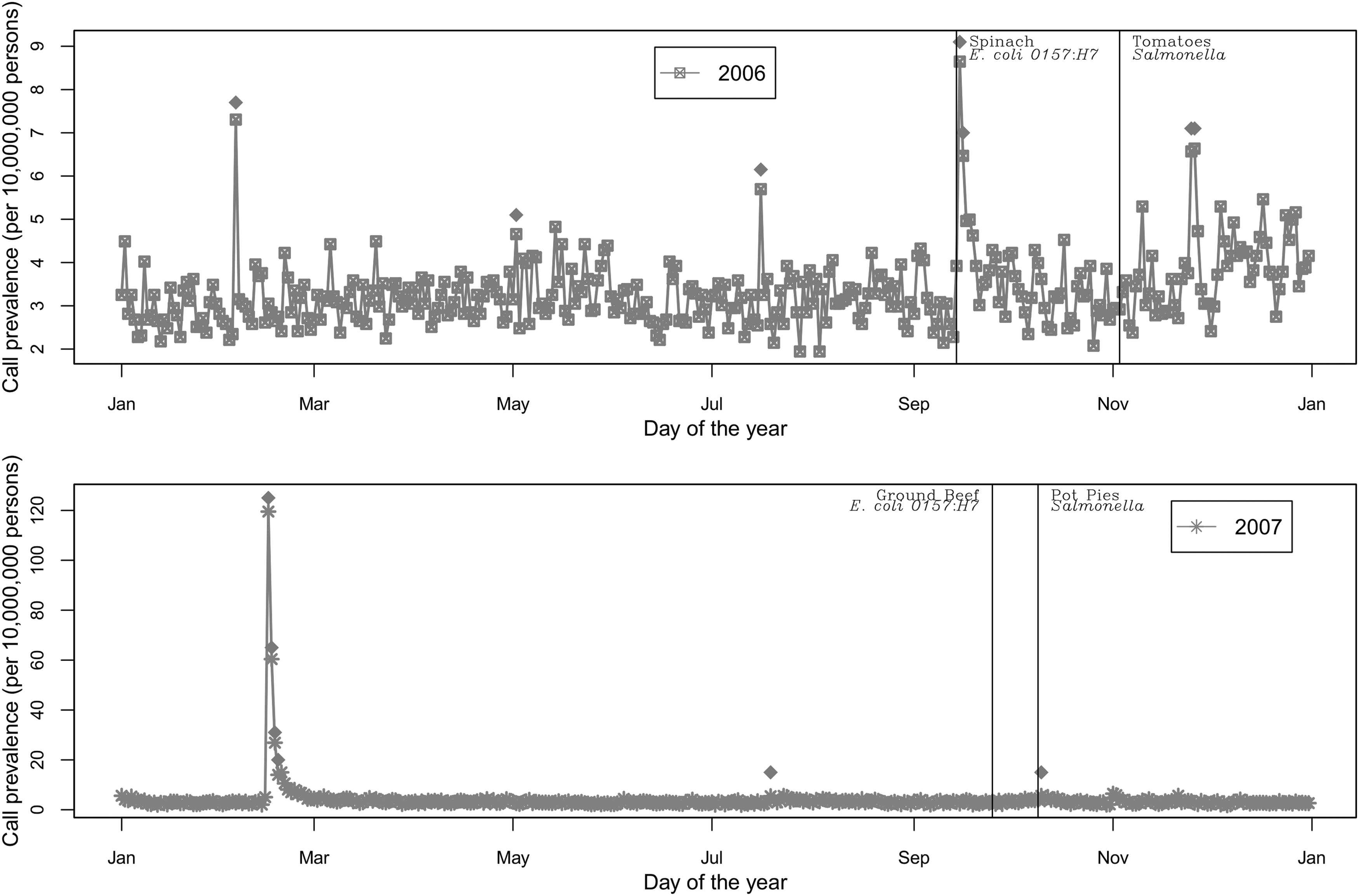
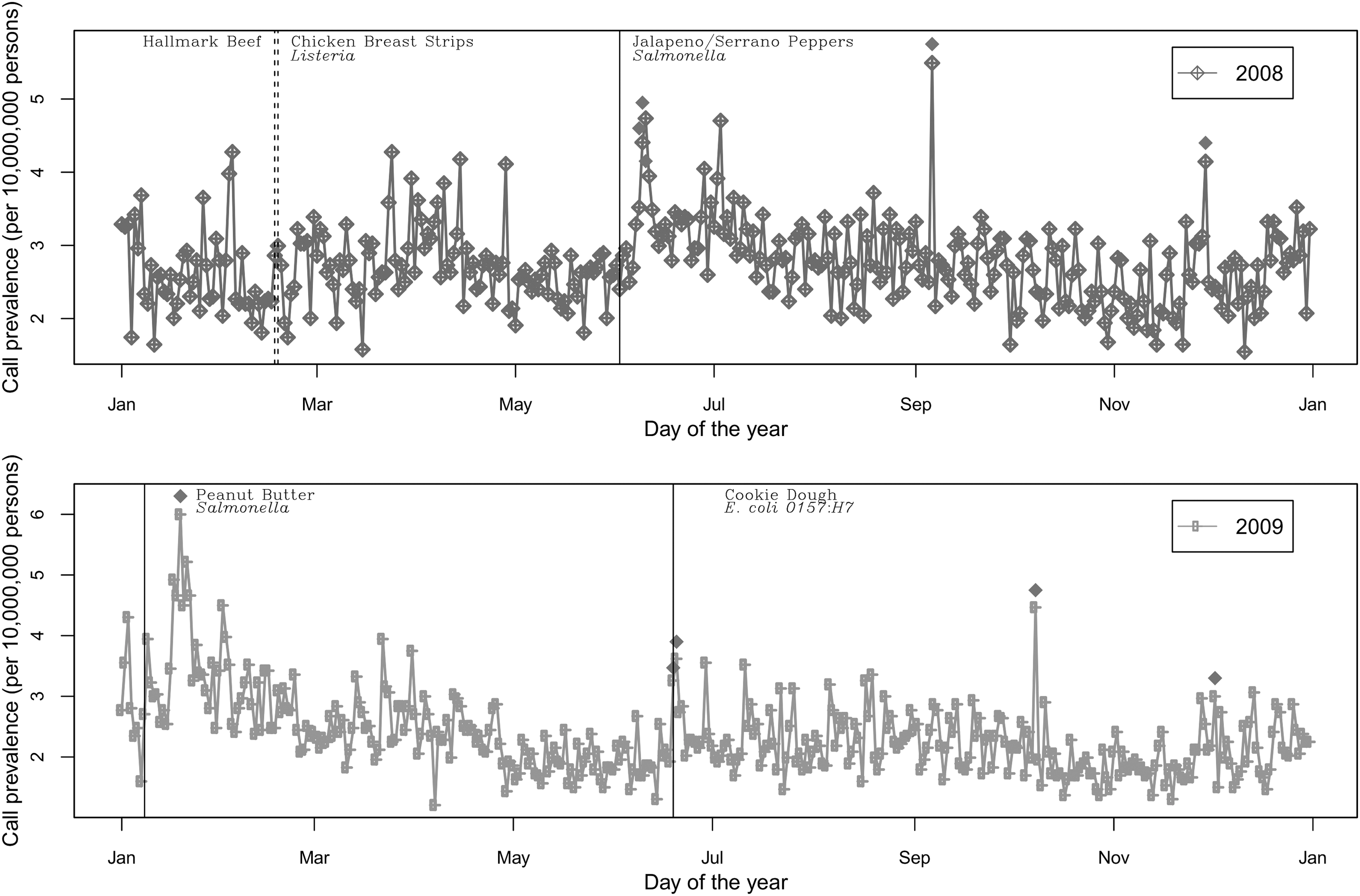
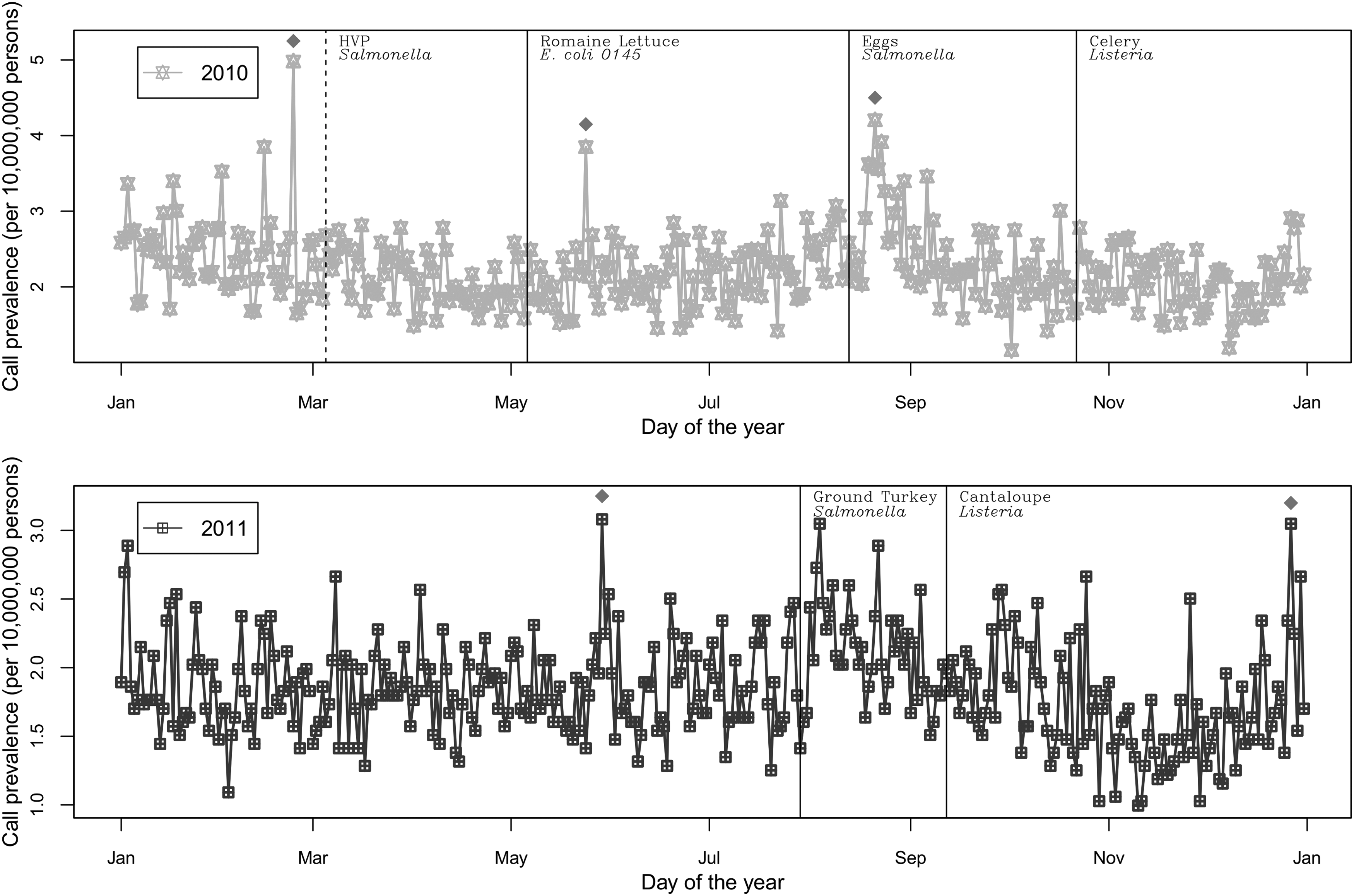
Forty-two significant changes in daily call prevalences (defined to be an anomaly) were detected during the 12-year period (Fig. 4). Dates of anomalies were compared to the first public announcement of 18 outbreaks/recalls (Table 5). Eleven anomalies occurred within 28 days before and 14 days after an outbreak/recall announcement. Most (91%) occurred after the public announcement. Only one occurred before the announcement of an outbreak/recall (hydrogenated vegetable protein, 2010). Four anomalies occurred on or within 7 days after an outbreak/recall announcements: spinach (2006), pot pies (2007), jalapeno/serrano peppers (2008), and cookie dough (2009). Three anomalies occurred 8–14 days after an outbreak/recall announcement: jalapeno/serrano peppers (2008), peanut butter (2009), and eggs (2010).
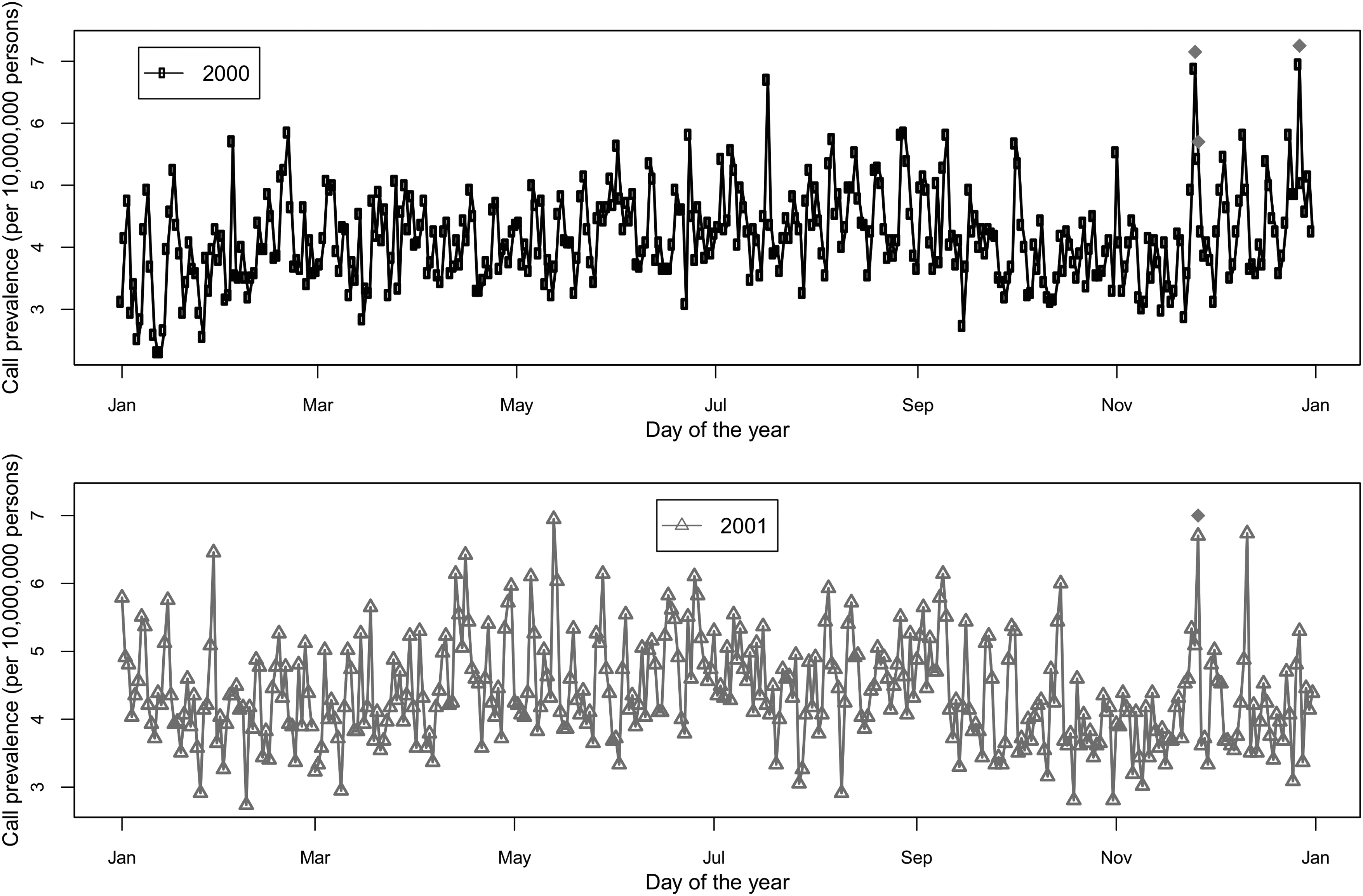
Daily prevalence of self-reported foodborne disease calls per 10,000,000 persons from 2000 to 2011. Vertical lines represent major national outbreaks (solid lines) or recalls (dashed lines). Diamonds above trend lines represent anomalies in call prevalence identified using Early Aberration Reporting System (EARS) software.
Time period surrounding the date of public health announcement for the selected national outbreaks or recalls.
Multiple anomalies were considered part of a unique event when they occurred within the specified time frame for the row.
Percent of national outbreaks or recalls with EARS anomalies near time of announcement.
Includes date of public announcement.
The number of anomalies detected varied by month over the 12-year period (Fig. 5). The highest number of anomalies occurred in winter months (February and November) followed by summer and early fall (June and September). Seven anomalies, the most of any 1 year, and six anomalies occurred in 2006 and 2007, respectively.
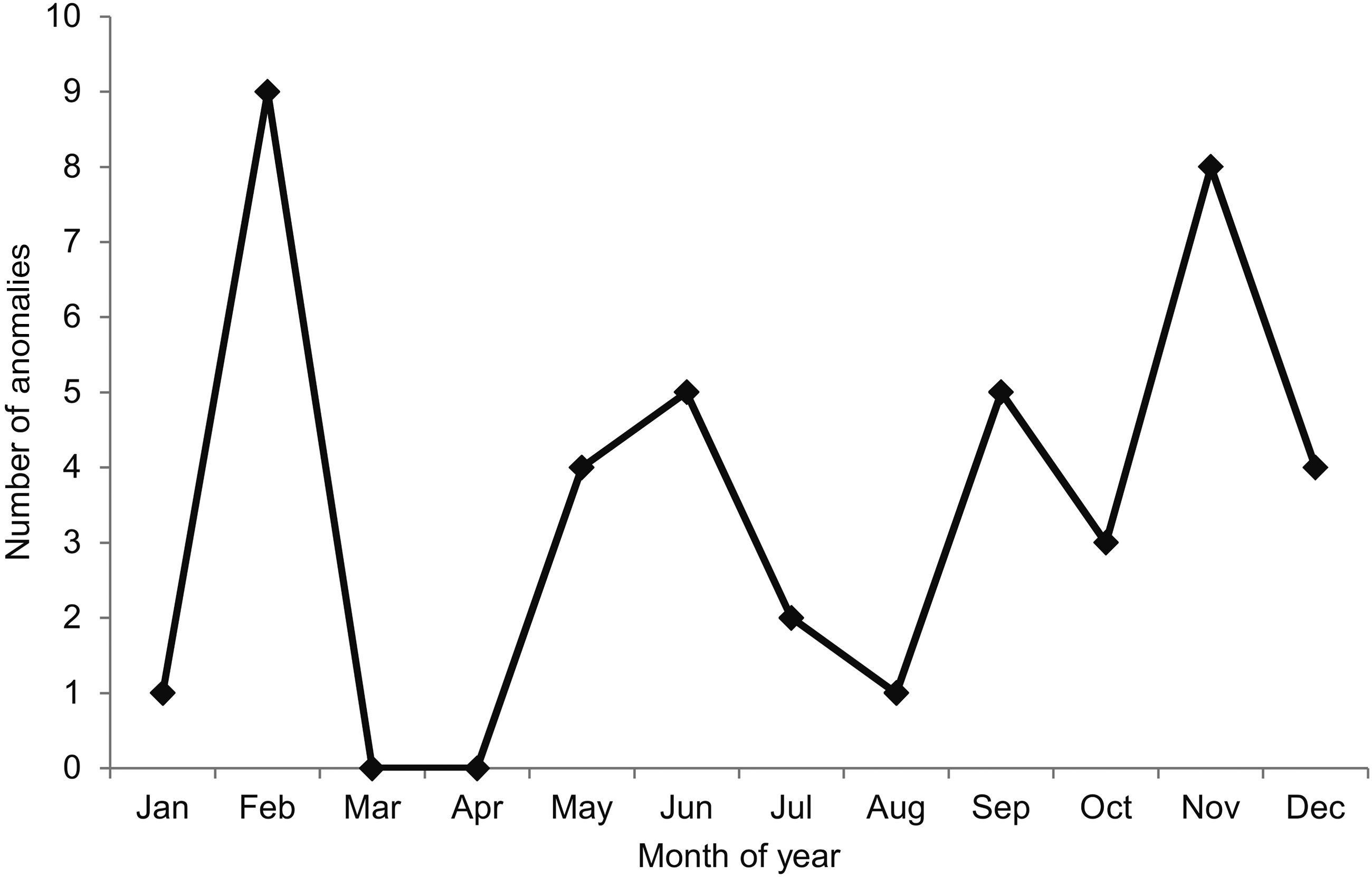
Monthly trends in anomalies of self-reported foodborne disease call prevalence identified by the Early Aberration Reporting System (EARS) using U.S. poison center data from 2000 to 2011.
Discussion
FBD surveillance is a critical part of the food safety system and provides important information used to detect outbreaks, monitor trends, and quantify the impact of FBD. Pathogen-specific surveillance systems, which focus on laboratory-confirmed FBD cases, often result in under-reporting and substantial time delays in detecting outbreaks. Consumer complaint data have become increasingly useful for FBD surveillance and outbreak detection. In 2011, 81% of local health departments reported using a complaint-based surveillance system, and these complaint-based systems detected more outbreaks than any other surveillance mechanism (Li et al., 2011). In addition, the time from onset of illness to outbreak detection for consumer complaint systems was similar to reports by healthcare providers and less than pathogen-specific surveillance (Hedberg et al., 2008). Furthermore, complaint-based surveillance systems have the advantage of using information on all diseases, not just those reportable to CDC (Li et al., 2010, 2011). Nontraditional sources of consumer complaint data, including Google internet query data of gastrointestinal-related search terms (Desai et al., 2012), have been explored as a complement to traditional surveillance methods.
In the current study, we evaluated NPDS data as a potential source of consumer complaint data for detection of large national outbreaks and recalls. Local PC data have been demonstrated to have utility as a form of FBD surveillance (Derby et al., 2005). Call data from the Arizona Poison and Drug Information Center was used to identify cases of FBD and cross-referenced to laboratory confirmed cases reported to the Pima County Health Department. Interestingly, analysis of the PC data identified FBD cases that had not been reported to the health department. To date, no study has examined the utility of NPDS data.
Our evaluation of NPDS data found that self-reported FBD exposures might not be reliable for FBD surveillance. First, about half of calls did not report any common FBD clinical effects (diarrhea, nausea, vomiting, and abdominal pain). Second, a significant number of callers identified implausible FBD exposures or exposure routes (i.e., bee stings, etc.). For example, 211 callers, on average, self-reported botulism to PCs each year during the 12-year period. In contrast, CDC reported, on average, 140 cases of botulism per year for the same time period (CDC, 2013). Given the severity of botulism and mandatory reporting requirements, it is unlikely that so many botulism cases would have gone unreported to CDC. Third, individuals reporting a FBD exposure do not appear to know the true source of their exposure. Studies of sporadic and outbreak-related illnesses have found that foods prepared outside the home are an important source of FBD (Jones and Angulo, 2006). For example, of the 6647 outbreaks reported in the United States from 1998 to 2002, only about 20% of foodborne outbreaks were linked to private residences, whereas about 50% were associated with a restaurant/delicatessen (Lynch et al., 2006). However, in the current dataset, about 75% of exposures reportedly occurred at home, although it is unknown whether these exposures were related to food prepared in the home or food prepared outside the home but consumed at home. Finally, key data elements relevant to FBD surveillance are frequently missing (i.e., duration of clinical effects is not always recorded) or not collected by PCs. For example, while information on rectal bleeding is collected, this clinical effect could be quite different from bloody diarrhea, a key feature of a number of FBDs. Similarly, information on specific food, animal, water, and travel exposures was not collected. In addition, due to the lack of biological specimens, it was not possible to confirm FBD exposure or identify the specific pathogen.
In general, there was a decreasing trend in the self-reported FBD call prevalences over the 12-year period. However, this trend needs to be interpreted with caution as it could reflect the overall decreasing trend in PC calls (Bronstein et al., 2012) or a decrease in incidence of suspected FBD cases. According to the CDC, the incidence of FBD cases reported to public health officials in 2012 had not changed significantly from the 2006–2008 baseline (CDC, 2013). If the incidence of FBD is relatively constant over time but calls of FBD to PCs are decreasing in frequency, using NPDS for FBD surveillance may not be appropriate. A large increase in call prevalence was detected in February 2007. A post hoc literature search revealed that this increase might reflect a large national outbreak associated with peanut butter (FDA, 2007). However, it is uncertain why this increase was about five times greater than the maximum call prevalence in any other year.
Geographic and seasonal variations were observed in NPDS data. The highest call prevalences were observed in states in the Southwest and Northwest. In general, more anomalies in daily call prevalences occurred during November, February, June, and September, which is somewhat consistent with the seasonal trends expected for FBD (Wikswo et al., 2012). The incidence of norovirus tends to peak during winter months, whereas the incidence of bacterial FBD tends to be higher in late summer months (Wikswo et al., 2012). In 2006–2007, there was an ongoing norovirus epidemic (CDC, 2007) and, coincidentally, the largest number of anomalies in call prevalences was seen during the same time period, although these changes cannot be directly attributed to the outbreak.
Generally, NPDS data did not provide an early warning of large national outbreaks that were well publicized. Few unusual changes in daily call prevalences were identified around the time of the 18 national outbreaks/recalls. At most, there were five anomalies near the time outbreaks/recalls were announced publicly but most occurred after the outbreak/recall announcement, suggesting these data may not be useful for early detection. However, since most of these anomalies occurred shortly after public announcement, NPDS data could be used to enhance outbreak situational awareness. For example, during their investigation of the 2009 Salmonella Typhimurium outbreak associated with peanut butter, CDC used NPDS data to identify cases in five states that had not been detected through other surveillance systems (Wolkin et al., 2012).
There are several noteworthy limitations to the current evaluation of NPDS data. First, clinical effects data were not available for all callers, and the analysis was limited to self-reported exposures to FBD. Individuals reporting FBD were not definitively diagnosed, nor were epidemiological investigations conducted. Inconsistencies in the data, such as the absence of clinical effects and increased reports of botulism, suggest that individuals self-reporting FBD exposure to PCs may not actually be FBD exposures. Second, total number of calls received by PCs was not available; therefore, prevalences of FBD calls do not have precise denominators, which limit their interpretation. Third, we did not analyze regional trends in data, which may yield different results since 98% of FBD outbreaks occur at the state level (CDC, 2013).
Conclusions
NPDS is a potential source of FBD complaint data that could be used to monitor trends in FBD and identify potential outbreaks. However, it is currently difficult to draw conclusions about the utility of NPDS data for these purposes due to the questionable reliability of self-reported FBD exposures. Trends in FBD call prevalences appear to be decreasing, and exploratory analyses suggest that unusual changes in call prevalences occur after the announcement of national FBD events rather than before. Employing a syndromic approach may yield different results and should be explored.
Footnotes
Acknowledgments
This work was supported by the American Association of Poison Control Centers (J.G. and J.B.), and by U.S. Department of Agriculture (USDA) National Institute of Food and Agriculture (NIFA) under the auspices of the USDA-NIFA Food Virology Collaborative (NoroCore; B.K., grant number 2011-68003-30395).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.