
Abstract
Objective:
Enteric illness represents a significant burden of illness in Canada and internationally. Building on previous research, an expert elicitation was undertaken to explore the routes of transmission for 28 pathogens involved in enteric illness in Canada. This article considers the subcategories of foodborne, waterborne, and animal contact transmission.
Methods:
As part of an expert elicitation, 31 experts were asked to provide estimates of source attribution for subcategories of foodborne (n = 15), waterborne (n = 10), and animal contact (n = 3) transmission. The results from an online survey were combined using triangular probability distributions, and median and 90% credible intervals were produced. The total proportion and estimated number of cases of enteric illness attributable to each type of food commodity, water source, and animal exposure route were calculated using results from the larger elicitation survey and from a recent Canadian foodborne burden of illness study (Thomas et al., 2013).
Results:
Thirty experts provided foodborne subcategory estimates for 15/28 pathogens, waterborne subcategory estimates for 14/28 pathogens and animal contact subcategory estimates for 5/28. The elicitation identified raw produce, recreational water, and farm animal contact as important risk factors for enteric illness. These results also highlighted the complexity of transmission, with greater uncertainty for certain pathogens and routes of transmission.
Conclusions:
This study is the first of its kind to explore subcategories of foodborne, waterborne, and animal contact transmission across such a range of enteric pathogens. Despite inherent uncertainty, these estimates present an important quantitative synthesis of the roles of foodborne commodities, water sources, and pathways of animal contact in the transmission of enteric illness in Canada.
Introduction
E
Expert elicitation has previously been used as a source attribution tool, to explore the role of transmission in the most common enteric infections in Canada and around the world (Cressey and Lake, 2005; Hoffmann et al., 2006; Havelaar et al., 2008; Ravel et al., 2010; Vally et al., 2014; Butler et al., 2015). Some have focused particularly on subcategories of foodborne transmission (Hoffmann et al., 2006; Havelaar et al., 2008; Davidson et al., 2011), but very limited data exist on waterborne and animal contact routes.
As part of the Public Health Agency of Canada's (PHAC) burden of enteric illness and source attribution efforts, an expert elicitation was undertaken to attribute transmission of 28 enteric pathogens (Butler et al., 2015). An objective of this study involved the elicitation of specific subcategory estimates for foodborne, waterborne, and animal contact transmission of these same pathogens, which is the focus of this article. This research will help inform future research and surveillance efforts in Canada.
Materials and Methods
A six-stage expert elicitation for the attribution of 28 enteric illnesses to five major routes of transmission and their respective subcategories was undertaken in January–April 2014, methods described elsewhere (Butler et al., 2015). Briefly, a panel of 31 Canadian experts were each assigned 10 pathogens, based on self-assessed expertise collected in a presurvey.
Experts were asked to attribute 100 domestically acquired cases transmitted via food, water, or animal contact to their subcategories (Supplementary Material S1; Supplementary Data are available online at
Estimates were excluded where experts assessed confidence as 1/5 (low). Median and 90% credible intervals (CrI) for each subcategory were calculated from cumulative triangular probability distributions built using the Microsoft Excel add-in @Risk (Version 6.1.2; Palisade Corporation, Newfield, NY). Statistical methods are described elsewhere (Butler et al., 2015).
Cumulative estimates of transmission were combined with estimated distributions of annual cases for 28 pathogens obtained from recent Canadian burden of enteric illness estimates (Thomas et al., 2013). For enterotoxigenic Escherichia coli (ETEC), verotoxin-producing E. coli (VTEC) non-O157 and E. coli, other (non-VTEC, non-ETEC strains of E. coli), estimated domestic cases were determined by multiplying the domestic cases of VTEC O157 from Thomas et al. (2013) by the identified ratios relative to VTEC O157 from Thomas et al. (2013), derived from Scallan et al. (2011) and Chui et al. (2011). The estimated distributions of domestic cases for each pathogen (Npathogen) were multiplied by the cumulative distributions estimated via each of food, water, and animal contact transmission (e.g., Ppathogen[food]), derived from the first stage of the elicitation survey (Butler et al., 2015) using @Risk. These estimates were then multiplied by the distributions of the proportion of cases transmitted by each subcategory (e.g., Ppathogen[beef]) to estimate how many cases were attributable to specific commodities (e.g., Nbeef), and their 90% CrI.
Ethics approval was obtained from Health Canada and PHAC's Research Ethics Board on January 13, 2014 (REB 2013-0033).
Results
Attribution estimates for specific subcategories of foodborne, waterborne, and animal contact transmission routes were provided by 30 of 31 participating experts. Responses were excluded where confidence was ranked as 1/5 (low), representing 7/148 (5%) foodborne, 3/71 (4%) waterborne, and 6/70 (9%) animal contact transmission estimates. Data were also excluded for foodborne (n = 3) and waterborne (n = 1) transmission where major transmission route analysis indicated inappropriate clusters of responses (implying nonenteric transmission) (Butler et al., 2015).
Five or more experts provided foodborne subcategory estimates for 15/28 pathogens; waterborne subcategory estimates for 5/28 pathogens; and animal contact estimates for 5/28 pathogens. No subcategory estimates were provided for pathogens where less than 10 cases per 100 were attributed to that particular route (e.g., 8.3% of adenovirus transmission attributed to food and no foodborne subcategory estimates were provided).
Kitchen door attribution estimates for foodborne transmission were provided for 13/28 pathogens, with an average of two expert estimates per pathogen where provided. The shifts in attribution calculated from these estimates were negligible, but implied that cross-contamination, particularly from (raw) poultry in the kitchen, may play an important role in disease transmission, especially for Campylobacter spp. and nontyphoidal Salmonella spp.
Medians and 90% CrI from the cumulative distributions for foodborne, waterborne, and animal contact transmission subcategories are presented in Tables 1, 2, and 3, respectively, for pathogens with ≥5 experts responding. The elicited probability distributions should be interpreted with caution considering the uncertainty demonstrated in the CrI.
VTEC non-O157, verotoxin-producing Escherichia coli.
VTEC O157, verotoxin-producing Escherichia coli.
GUDI, ground water under the influence of surface water.
VTEC O157, Verotoxin-producing Escherichia coli.
Using total pathogen estimates from the Canadian foodborne burden of illness estimates (Thomas et al., 2013), 90% of cases of enteric illness with the 28 pathogens of interest were attributed to viruses, 8% to bacteria and 2% to parasites.
Food
For the foodborne estimates, raw produce was most frequently identified as the dominant source (3/14 pathogens) (Table 1); 21.8% (90% CrI: 8.1–37.5) of all foodborne cases were attributed to raw produce, 18.3% (90% CrI: 7.2–31.2) to seafood, and <10% each to the remaining subcategories (Fig. 1). For bacterial infections, the most attributed food vehicle was “other” (15.4%; 90% CrI: 3.2–28.7), followed by poultry (12.7%; 90% CrI: 2.9–24.8); raw produce was the most common food vehicle for parasitic (25.2%; 90% CrI: 4.6–54.3) and viral (29.1%; 90% CrI: 0.0–48.9) infections (Fig. 1).
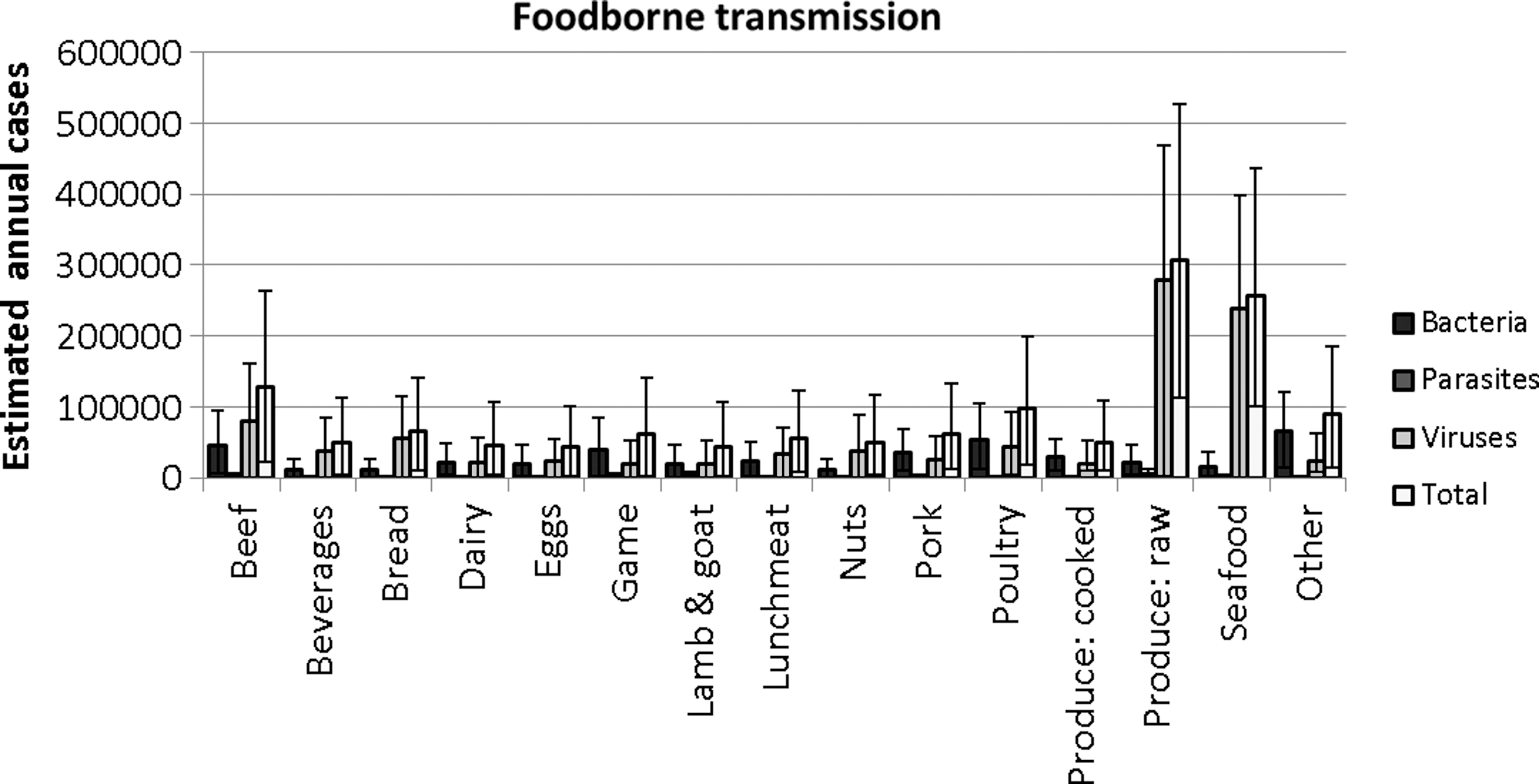
Proportion of foodborne cases attributed to 15 subcategories, by pathogen types and as a total. Error bars represent 90% credible intervals.
Water
For waterborne transmission, recreational water sources were the most commonly identified subcategory (3/5) (Table 2). Recreational water was attributed to the most cases overall within the waterborne transmission category (23.8%; 90% CrI: 2.6–52.8), and specifically for parasites (24.2%; 90% CrI: 8.3–46.1) (Fig. 2). Private well water was most frequently implicated for bacterial (29.4%; 90% CrI: 2.4–64.9) and viral infections (23.5%; 90% CrI: 1.0–53.0) (Fig. 2).

Proportion of waterborne cases attributed to 10 subcategories, by pathogen types and as a total. Error bars represent 90% credible intervals.
Animal
Farm animal contact was the most common vehicle within animal contact transmission (5/5) (Table 3). The majority of animal contact cases were attributed to farm animals (51.2%; 90% CrI: 5.5–100.0). Farm animal contact was identified as the main pathway for bacteria (54.0%; 90% CrI: 8.5–100.0), parasites (44.3%; 90% CrI: 6.6–92.1), and viruses (51.4%; 90% CrI: 4.3–100.0) (Fig. 3).
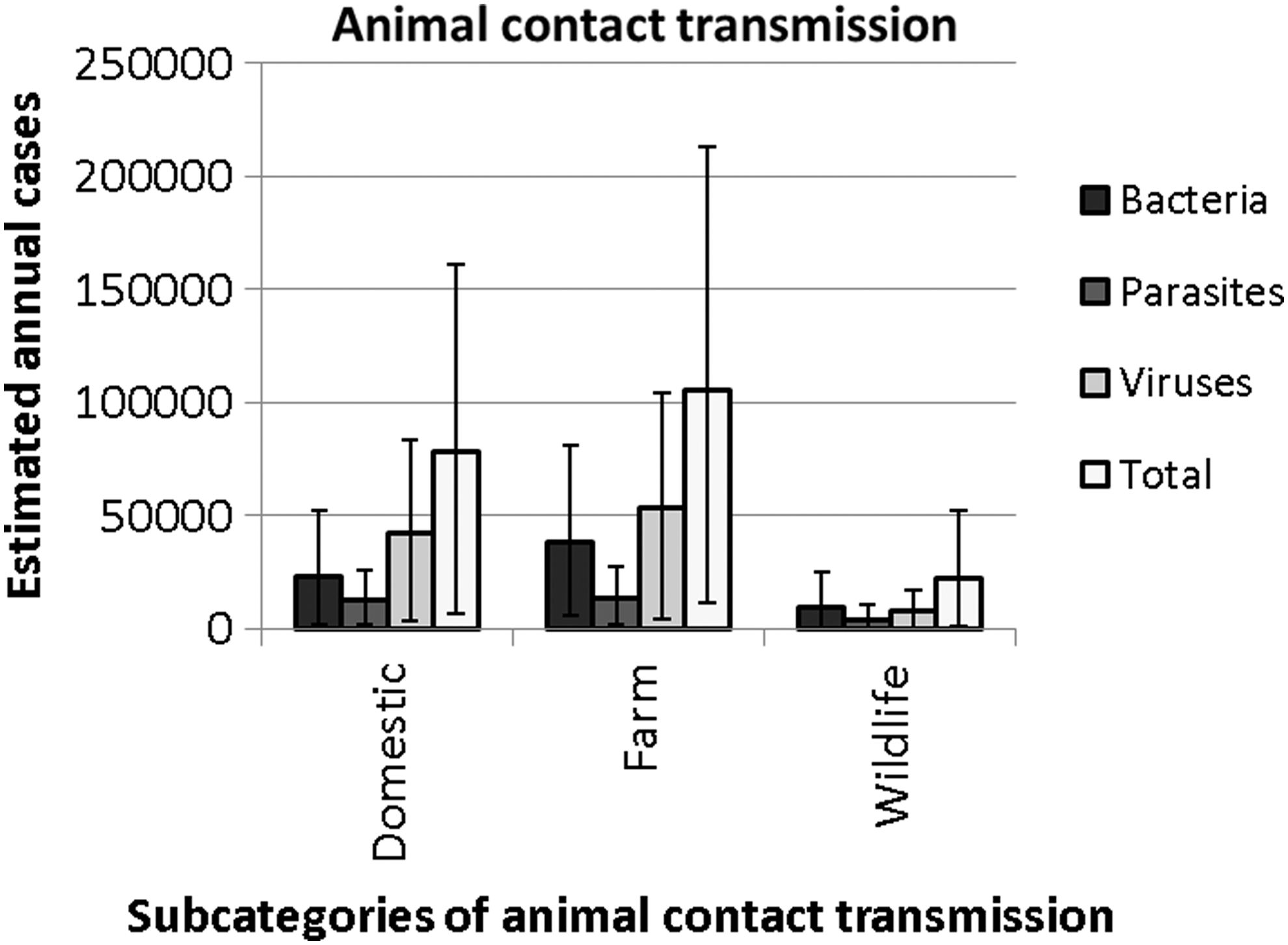
Proportion of animal contact cases attributed to domestic, farm, and wildlife animal contact, by pathogen types and as a total. Error bars represent 90% credible intervals.
Discussion
This study attributes the number of enteric cases related to 15 of 28 pathogens of public health importance in Canada to the subcategories of major enteric illness transmission routes (i.e., foodborne, waterborne, and animal contact). This study is one of the first to explore such an expansive list of enteric pathogens and has considered a wide range of viruses not considered in previous studies (Supplementary Material S2). Exploring the dominant sources of exposure to enteric pathogens, across and within transmission routes, is critical for public health initiatives targeted at reducing the burden of enteric illness in Canada. Identifying existing knowledge gaps related to enteric disease transmission dynamics in Canada is one outcome of this work.
Food
Raw produce was most frequently identified as the dominant source of foodborne transmission (7/24 pathogens) (Table 1). Of all foodborne cases, 21.8% (90% CrI: 8.1–37.5) were attributed to raw produce, 18.3% (90% CrI: 7.2–31.2) to seafood, and <10% each to the remaining subcategories (Fig. 1). For bacterial infections, the most attributed food vehicle was “other” (15.4%; 90% CrI: 3.2–28.7), followed by poultry (12.7%; 90% CrI: 2.9–24.8); raw produce was the most common food vehicle for parasitic (25.2%; 90% CrI: 4.6–54.3) and viral (29.1%; 90% CrI: 0.0–48.9) infections (Fig. 1). These results are similar to estimates from previous elicitations and from analysis of outbreak data (Supplementary Material S2).
Infection with Trichinella spp. is attributed largely to game (64.0%; 90% CrI: 14.1–92.2) and pork (31.0%; 90% CrI: 2.6–81.1) in the current study. Routine testing of swine as part of the Canadian Food Inspection Agency (CFIA) Trichinella control program (CFIA, 2013) demonstrates that domestic commercial herds are Trichinella-free, despite a recent (2013) case of human Trichinella spp. infection from a pig raised on a noncommercial farm (CFIA, 2013). This estimate highlights two limitations of this research design: (1) the inability to differentiate between domestic and imported foods: given the rarity of human trichinellosis, the role of imported meats could be significant; and (2) reliance of experts on historic trends over current exposures.
Beef was highlighted as the most important food commodity for VTEC O157 infections (47.4%; 90% CrI: 29.2–67.3), followed by produce: 19.5% raw and 1.2% cooked (20.7% total). This is similar to the previous Canadian elicitation, where beef was estimated to be responsible for 54.0–57.8% of VTEC O157 infections, followed closely by produce (23.1–28.8%) (Davidson et al., 2011). These results suggest consistency between the two Canadian studies, illustrating that for some infections, experts remain in consensus about the dominant sources.
Where estimates differ between this study and other Canadian studies (e.g., for Campylobacter spp. C. botulinum and Staphylococcus aureus), sources of disagreement are unclear. The differences in responses may reflect a lack of data from which experts can derive estimates, highlighting a knowledge gap for future research, given the role some of these pathogens play in the overall burden of foodborne illness. Alternately, they may reflect considerations related to food categories explored.
For Clostridium botulinum, current estimates indicate an important role of cooked (preserved) produce, which may correspond to canned goods in the “other” category in retrospective outbreak studies (Greig and Ravel, 2009). However, in outbreak studies, seafood (Greig and Ravel, 2009) and game (Ravel et al., 2009) are identified as the dominant risk factors.
Cyclospora cayetanensis transmission is mostly attributed to raw produce (61.7%; 95% CrI: 20.8–85.0), similar to the previous U.S. elicitation (Hoffmann et al., 2006) and outbreak studies from the United States (Batz et al., 2011) and internationally (Greig and Ravel, 2009). Epidemiological studies suggest that untreated drinking water and produce imported from endemic regions (particularly berries and salad greens) are significant risk factors, and the potential role of animals in transmission is unknown (Ortega and Sanchez, 2010).
Raw (unpasteurized) dairy consumption (especially milk) was identified in supplementary comments as an important transmission route for Campylobacter spp., VTEC O157, and VTEC non-O157. Raw milk was not specifically queried; however, dairy was implicated for Campylobacter spp. (9.5%), Listeria monocytogenes (17.0%), VTEC O157 (10.4%), and VTEC non-O157 (7.6%) (Table 1). The sale of raw milk is illegal in Canada, though cheeses made from raw milk are legal (Health Canada, 2014), and preliminary estimates indicate 3.1% of the Canadian population consumes raw milk and raw milk products.
Water
No previously published expert elicitations have explored the waterborne transmission route in such detail. Recreational water was attributed to the most cases overall within the waterborne transmission category (23.8%; 90% CrI: 2.6–52.8), and specifically for parasites (24.2%; 90% CrI: 8.3–46.1) (Fig. 2). Private well water was most frequently implicated for bacterial (29.4%; 90% CrI: 2.4–64.9) and viral infections (23.5%; 90% CrI: 1.0–53.0) (Fig. 2).
Recreational water exposure was identified as the main risk factor for 3/5 pathogens for which estimates were provided (Table 2). Waterparks and pools have been recognized as important sources of Cryptosporidium spp. and Giardia spp. infections (Snel et al., 2009; Yoder et al., 2012a, b) and pool-associated outbreaks in the United States (Lam et al., 2014) and Canada (CCDR, 2004). Cryptosporidium spp., C. cayetanensis, and Giardia spp. are particularly resistant to chlorine, which is the most common type of disinfectant used in these settings (WHO, 2011). During the 1-day discussion, experts questioned the likelihood of sufficient persistence of other Vibrio spp. in Canadian water temperatures to facilitate waterborne infection (Tantillo et al., 2004). Domestic waterborne transmission of Vibrio spp. through enteric routes (i.e., not wound infection) is not believed to play a major role in transmission (3.8–11.0% of Vibrio infection attributable to water) (Butler et al., 2015). Less than five experts provided estimates for any of the Vibrio spp. explored in this study., reflecting a lack of Canadian knowledge on this particular route of transmission.
Private wells were the primary source identified for 2/5 pathogens (Table 2). Canadian studies have demonstrated the role of private well water as a risk for enteric illnesses (Uhlmann et al., 2009; Galanis et al., 2014). In this study, GUDI wells were implicated in viral infections more frequently than bacterial or parasitic infections (Fig. 2).
Attribution to municipal water systems was divided based on the size of population serviced by the municipal system: large municipal systems (>1000 population served, 13.3% of total waterborne cases) and small municipal systems (<1000 population served, 23.1%). Size is used as a proxy of level of treatment, resources available to support treatment adoption, and operator training (Murphy et al., 2015).
Experts estimated that <1% of total waterborne infection was attributable to bottled water. Bottled water has been involved in several outbreaks in the United States; however, there is no current evidence of waterborne infections associated with bottled water in Canada (Brunkard et al., 2011).
Animal
This is the first expert elicitation to consider sources within the animal contact transmission route. Previous elicitations in Australia and the Netherlands explored transmission via direct animal contact (Vally et al., 2014) and human and animal transmission (Havelaar et al., 2008); the current study elucidates source attribution more deeply. Animal contact transmission was defined as relating to illness transmitted by exposure to animals (i.e., personal contact [hand or mouth] with animal/pet feed, animal/pet fur/coats, saliva, or feces). Farm animal exposure was estimated as the most likely transmission route for all five pathogens for which estimates are provided (Table 3). The majority of animal contact cases were attributed to farm animals (51.2%; 90% CrI: 5.5–100.0), and specifically for bacteria (54.0%; 90% CrI: 8.5–100.0), parasites (44.3%; 90% CrI: 6.6–92.1), and viruses (51.4%; 90% CrI: 4.3–100.0) (Fig. 3).
The likelihood of enteric pathogen transmission from household pets may be low compared to an encounter with farm animals or wildlife; however, the higher frequency of pet contact (David et al., 2014) would suggest this is an important exposure. Expert discussion highlighted the need to consider the relative extent to which frequent pet contact contributes to human enteric illness compared to low frequency exposure to farm animals and wildlife, and the relative risks, identified as a current knowledge gap in Canada. A limitation of these estimates is evident for animal contact transmission rotavirus, for which group discussion suggested zoonotic transmission was unlikely, yet animal contact transmission estimates have been produced (Table 3). This highlights the need to consider attribution estimates carefully in context of both the number of respondents and uncertainty as demonstrated by CrI width. A low response rate in this study is an indicator of a lack of knowledge for the specific pathogen and transmission route.
Study limitations
The limitations of this study are described in more detail in Butler et al. (2015). The study's greatest limitation is the low response rate, resulting in small panel sizes for some pathogen/product combinations. Wide confidence intervals for estimates of certain pathogens and transmission routes reflect uncertainty that arises from lack of knowledge and data, highlighting areas for future research. Recall bias related to large-scale or notable outbreaks that have occurred in Canada or globally could have skewed the expert estimates to reflect high impact, low likelihood events. This study lacks the ability to differentiate between risks from imported and domestic food exposures.
This study does not characterize variations in exposure between the local and national level. It can be conceptually difficult to balance the role of local or geographically specific exposure while producing nationally representative estimates, which contributes to the range of uncertainty presented for each estimate. This limits our ability to differentiate between the variability and uncertainty that influences the widths of the credible intervals presented herein.
Conclusions
Expert elicitation is a useful tool for answering difficult questions where data are unavailable or expensive to obtain. This study explored the source attribution of 15 of 28 enteric pathogens at a previously unexplored level of detail for subcategories of foodborne, waterborne, and animal contact transmission. These results highlight the importance of raw produce, recreational water, and farm animal contact in transmission of enteric diseases as well as the complexity of transmission. While gaps in our understanding of source attribution remain, highlighting areas for future research, this study helps to improve our understanding of the role of food commodities and other sources in the transmission of enteric illness in Canada.
Footnotes
Acknowledgments
The researchers would like to thank all of the participating experts for their participation and engagement with this elicitation project. This research has been conducted under a National Sciences and Engineering Research Council postdoctoral research fellowship held by Ainslie Butler, working with the Centre for Food-borne, Environmental, and Zoonotic Infectious Diseases and FoodNet Canada (formerly C-Enternet) with the Public Health Agency of Canada.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.