
Abstract
A multischool outbreak of salmonellosis caused by Salmonella enterica serovar Napoli was investigated in the province of Milan from October to November 2014, following an increase in school absenteeism coinciding with two positive cases. Epidemiological studies detected 47 cases in four primary schools: 46 children and 1 adult woman (51.4% males and 48.6% females, median age 8.9). From these, 14 cases (29.8%) were severe and resulted in hospitalization, including 6 children (12.8%) who developed an invasive salmonellosis. The epidemic curve revealed an abnormally long incubation period, peaking 1 week after the first confirmed case. Twenty-five available isolates were typed by pulsed-field gel electrophoresis showing an identical pattern. The isolate belongs to ST474, an ST composed exclusively of Salmonella Napoli human strains isolated in France and Italy. Antibiotic resistance analysis showed resistance to aminoglycosides, correlating with the presence of the aminoglycoside resistance gene aadA25 in its genome. Trace-back investigations strongly suggested contaminated ham as the most likely food vehicle, which was delivered by a common food center on 21 October. Nevertheless, this ingredient could not be retrospectively investigated since it was no longer available at the repository. This represents the largest Salmonella Napoli outbreak ever reported in Italy and provides a unique scenario for studying the outcome of salmonellosis caused by this emerging and potentially invasive nontyphoidal serotype.
Background
I
It has been reported that some nontyphoidal serotypes such as Choleraesuis or Dublin are more likely to cause bacteremia (Wilkins and Roberts, 1988), but no studies have focused on the invasive ability of the serotype Napoli yet.
In Europe, infections caused by Salmonella enterica serovar Napoli have notably increased over the last few years, mainly affecting France, Switzerland, and Italy (Fisher et al., 2009). During the period 2000–2013, the incidence of Salmonella Napoli has increased by 256%, thus becoming the 13th most prevalent serotype isolated from humans (Eurosurveillance editorial team, 2015). The same trend was observed in Italy, where in 2011, Salmonella Napoli became the sixth most common serotype identified in humans with most cases reported in the Lombardy region (Graziani et al., 2013), where in 2013, its incidence (1.49 × 100,000 inhabitants) exceeded that of S. Enteritidis (1.19 × 100,000 inhabitants), reaching third position in this northern Italian region (Italian surveillance system IT-ENTER-NET, 2014).
Although Salmonella Napoli usually causes sporadic cases, it has been responsible for causing outbreaks in the past. The first reported Salmonella Napoli outbreak occurred in the United Kingdom at the beginning of the 80s due to the consumption of contaminated chocolate bars produced in Italy (Gill et al., 1983). This serotype has also been responsible for causing an outbreak attributed to horse salami in 1984 (Costa et al., 1986) and a waterborne epidemic in a primary school in 2011 (Zuliani et al., 2012), both of which occurred in northern Italy. However, Salmonella Napoli epidemiology, ecology, and virulence have been little investigated, since it seems to be hyperendemic in this Italian region.
In Italy, clinicians report cases of infectious diseases (suspected or ascertained) to the Local Public Health Units (LPHUs), which are responsible for carrying out epidemiological investigation. During the period from 21 October to 15 November 2014, the Milano 1 LPHU detected 47 cases of Salmonella Napoli infection involving four primary schools and a common catering service localized at Paderno Dugnano, a town adjacent to Milan, Italy. A multidisciplinary team was called in composed of healthcare authorities, clinicians from the various hospitals, and microbiologists from the Reference Laboratory to investigate the suspected outbreak.
In this study, we present the results of the investigation of the largest Salmonella Napoli outbreak ever reported in Italy, which provides information for gaining valuable insight into salmonellosis caused by this emerging serotype and highlights its ability to become invasive.
Materials and Methods
Epidemiological investigations
After being alerted by a school director on 3 November, the LPHU started retrospective and prospective investigations to determine the day of origin, the likely source, and the burden of the salmonellosis epidemic.
A confirmed case was defined as a person (1) attending one of the affected schools, (2) suffering from abdominal pain, diarrhea, and/or fever, and (3) having a stool and/or blood culture positive for Salmonella Napoli, in the period from 21 October to 15 November 2014. Suspected Salmonella Napoli cases were estimated according to the school absenteeism observed during the period from 20 October to 15 November 2014.
Initially, in the presence of their parents, affected pupils were asked to report any extra-scholar activities, the beginning and the nature of the symptoms, and the food consumed the previous or the same day as the beginning of the symptoms. Parents were asked about secondary cases in the family. Patient information forms were requested from pediatricians and hospitals, and the professionals involved were interviewed telephonically. The common catering service that was responsible for supplying meals to all of the affected schools (four primary schools) as well as to seven infant schools and three secondary schools was investigated. Taking into account the date of the first confirmed case (21 October) and considering the typical salmonellosis incubation period (6–72 h), menus delivered by the catering service to all schools between 18 and 21 October were investigated.
The catering service was investigated on its compliance to standard protocols (Hazard Analysis and Critical Control Point [HACCP] System), hygienic conditions, quality controls, and official documentation. Microbiological investigations were conducted on kitchen tools and surfaces, and all kitchen operators (ten) were interviewed in situ and subjected to stool culture analysis. Of ingredients contained in the suspected meal, only a salad sample was available for microbiological analysis. Hygienic conditions and quality controls were also inspected for the salad manufacturer. The Department of Veterinary Prevention of the LPHU—which is responsible for monitoring animals and food for pathogen contamination—was interviewed with the aim of locating a possible contaminated ham batch circulating in the Lombardy during this period.
In a second interview, directors from all schools served by the common catering service were requested to provide school absenteeism information during the period from 21 October to 15 November. All affected pupils from the four primary schools were asked whether they ate the ingredients in the meal on 21 October.
Microbiological and molecular characterization
Salmonella spp. isolates were serotyped at the LPHU Laboratory according to the White–Kauffmann–Le Minor scheme (Grimont and Weill, 2007). Pulsed-field gel electrophoresis (PFGE) analysis was performed for 25 representative isolates at the Regional Reference Laboratory of University of Milan using XbaI digestion, according to the PulseNet protocol (Graves and Swaminathan, 2001). XbaI-digested DNA from S. enterica ssp. enterica serotype Braenderup H9812 was used as a size reference standard (Hunter et al., 2005). Clustering analysis was performed with BioNumerics 6.6 software (Applied Maths, Sint-Martens-Latem, Belgium). In silico multilocus sequence typing (MLST) analysis was performed previously for the representative strain SN310 (Huedo et al., 2015).
Antibiotic resistance analysis was carried out at diverse hospital laboratories using the Phoenix™ System (BD Diagnostics, Sparks, MD). The following antibiotics were tested: amikacin, amoxicillin/clavulanic acid, ampicillin, aztreonam, cefepime, ceftazidime, ceftriaxone, colistin, ertapenem, fosfomycin, gentamicin, imipenem, levofloxacin, meropenem, norfloxacin, piperacillin/tazobactam, ticarcillin, ticarcillin/clavulanic acid, tigecycline, tobramycin, and trimethoprim/sulfamethoxazole. Antimicrobial breakpoints were determined using the criteria proposed by the European Committee on Antimicrobial Susceptibility Testing (EUCAST).
The genome of the Salmonella Napoli outbreak-related isolate—named Salmonella Napoli strain SN310—(GenBank accession number LFIH00000000.1) (Huedo et al., 2015) was examined for the presence of putative aminoglycosides resistance genes using the software CARD (The Comprehensive Antibiotic Resistance Database,
Results
Description of the outbreak
During the week 3–7 November, the LPHU received notifications from three Directors of three primary schools from Paderno Dugnano reporting increased absences among children due to enteritis, coinciding with two salmonellosis cases. Some children—those with more severe symptomatology—required medical attention that later resulted in the identification of Salmonella in their stool and/or blood samples. At this moment, the LPHU started interviews of affected children and families, and kept in close contact with the various schools, healthcare centers, and laboratories to detect more related cases.
Overall, during the period from 21 October to 15 November, a total of 47 cases of salmonellosis were confirmed; 1 female professor and 46 children (51.4% males and 48.6% females, median age 8.9 years), all belonging to four primary schools (Table 1). Abdominal pain, diarrhea, and fever were common symptoms among the patients, and in some cases, blood was detected in their feces. Fourteen patients (29.8%) required hospitalization, among which there were 6 children (12.8%) who also had positive blood culture. The general attack rate was 3.5% (Table 1). School absenteeism observed in the four primary schools during the epidemic suggests that the real burden was considerably higher, since a total of 142 pupils missed at least 1 day of school due to enteritis (Table 1), although most of them did not require medical care.
Including adults from diner commission.
Invasive rate: (invasive infections/total cases) ×100.
Absent pupils due to enteritis during the period 20 October to 15 November.
SD, standard deviation.
All primary schools reported a similar percentage of absenteeism (9–13%). The most affected period was the week 27–31 October, with the maximum number of absences for all primary schools recorded on 28 October. This is in concordance with the epidemic curve (Fig. 1), which shows that most cases arose between 21 October and 2 November (a period of 13 days), peaking on 26 October (6 days after the first confirmed case). In three cases, the onset of symptoms was fairly delayed with the last case occurring 26 days after the first confirmed case, which may represent secondary cases.
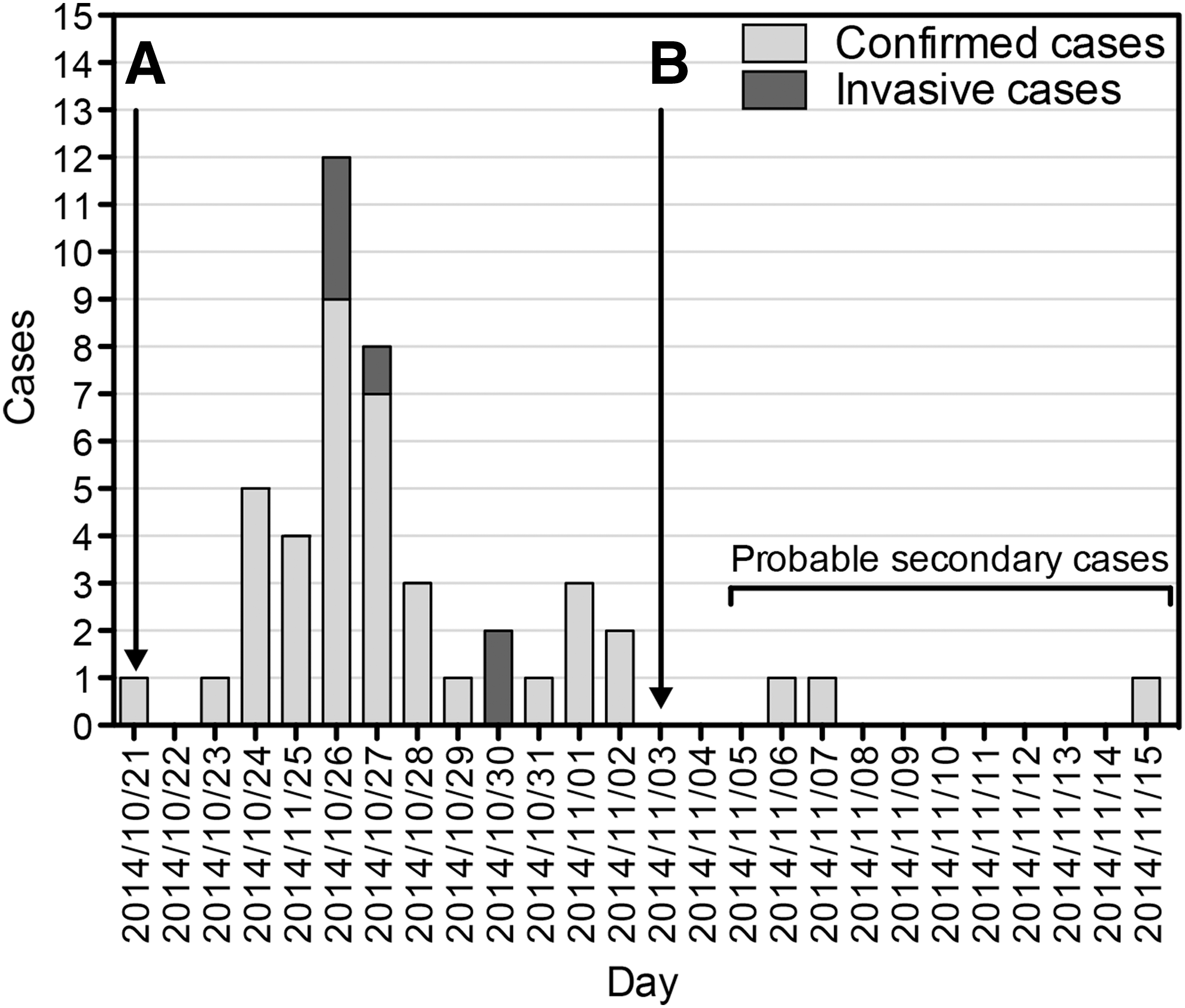
Epidemic curve of Salmonella Napoli outbreak. Confirmed cases are reported based on the day of the onset of the symptoms.
The only possible link among all affected schools was found to be the common catering service. Besides providing meals to these four primary schools, the food center also supplied food to seven infant schools and three secondary schools. Nevertheless, positive cases and an increment on school absenteeism were only reported among the primary schools. Accordingly, menus from the days before the first case were investigated for all schools served by the suspected food center. It was found that all schools generally consumed the same menu, except for the day 21 October on which the children attending the four primary schools consumed a menu composed of (1) “pizza margherita,” (2) a portion of ham, and (3) green salad with corn. Contrarily, the infant schools ate a menu composed of (1) pasta with spices, (2) omelet (pasteurized eggs), and (3) green salad with corn, while the secondary school pupils did not have lunch at school on the 21 October.
Microbiological analysis of the available salad sample resulted negative for the presence of Salmonella, and the manufacturer complied with all quality controls and hygienic conditions. Therefore, Salmonella Napoli was most probably transmitted through one of the ingredients in the pizza “margherita” or the ration of ham. Nonetheless, kitchen operators stated that the pizza was oven reheated for 30 min at 100°C, while the ham portion was served unheated and separately. Unfortunately, it was not possible to analyze the ham, as it was no longer available at the repository. However, the Department of Veterinary Prevention from the LPHU communicated that the routine quality controls carried out by the ham production plant were negative for the presence of Salmonella Napoli. This was supported by the fact that no other Salmonella Napoli case associated with the consumption of ham from the same production plant was reported. This makes us hypothesize that a cross-contamination occurred at the catering service facilities, which led to the examination of the facilities and staff. A microbiological analysis of the kitchen surfaces and tools, as well as all the stool cultures of kitchen workers, resulted negative. The facilities complied with standard protocols (HACCP System), including hygienic conditions, quality controls, and official documentation.
Identification and characterization of Salmonella isolates
All 47 human isolates were serotyped at the LPHU Laboratory and were identified as Salmonella Napoli. Twenty-five representative isolates—stool and blood isolates from various patients belonging to different schools—were typed by PFGE and showed identical pulsotype (Fig. 2), which did not match with any Salmonella Napoli isolate in our collection. In one of our previous studies, the genome of the representative strain SN310 was sequenced and the in silico MLST analysis revealed that the isolate belongs to ST474 (Huedo et al., 2015).
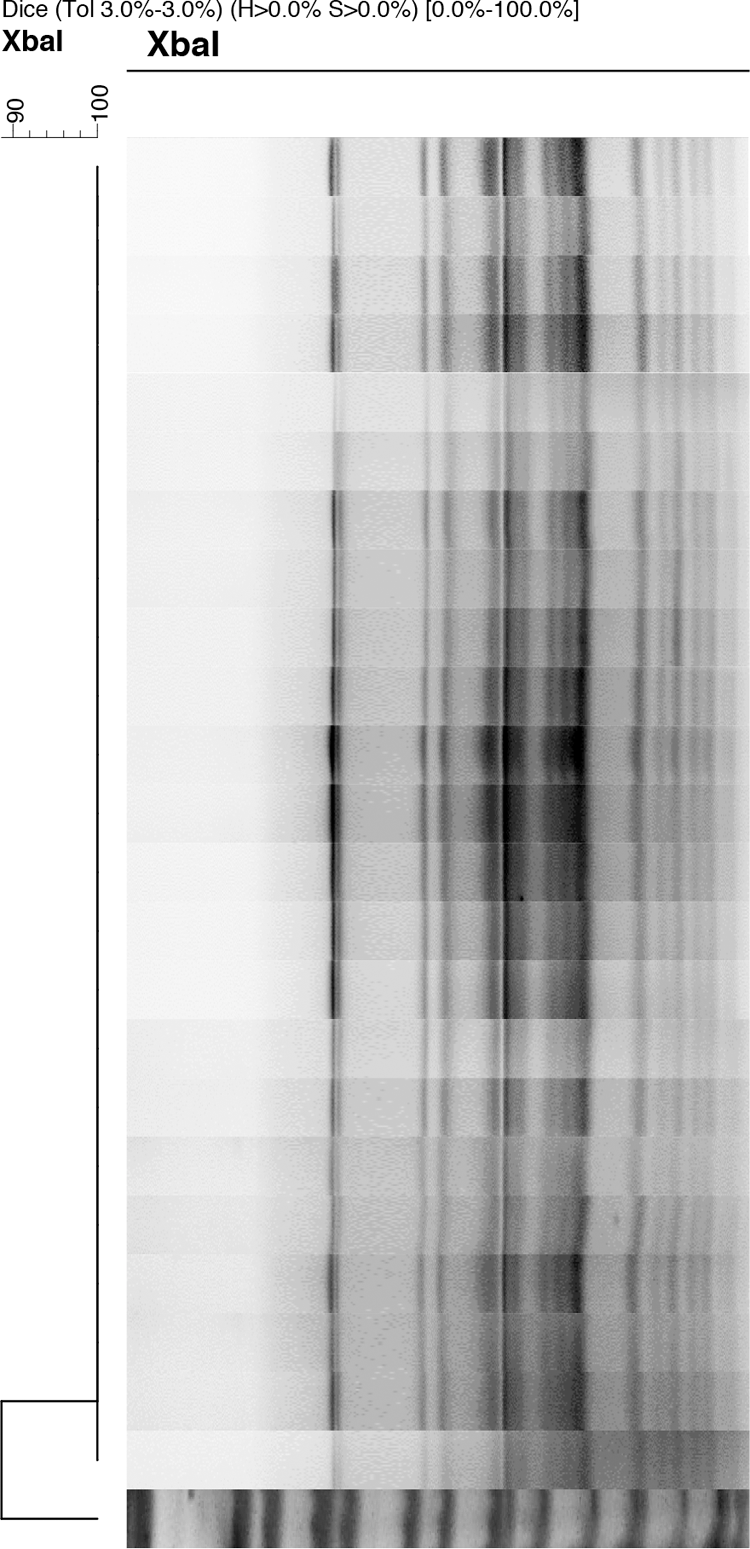
Banding profile determined by pulsed-field electrophoresis and dendrogram showing the genetic relatedness of 25 Salmonella Napoli human isolates recovered from patients during the outbreak. Salmonella Braenderup was used as molecular size marker.
Antibiotic resistance was tested for 10 isolates showing the same resistance profile. Surprisingly, the isolate was only resistant to all aminoglycosides tested: gentamicin, tobramycin, and kanamycin. The genome of the representative outbreak isolate Salmonella Napoli strain SN310 (Huedo et al., 2015) was in silico investigated for the presence of putative aminoglycoside resistance genes using CARD software (McArthur et al., 2013). A homologue of the gene encoding for the adenyltransferase AadA25 from Pasteurella multocida—which confers resistance to aminoglycosides (Michael et al., 2012)—was identified in its genome, suggesting a direct implication on such resistance.
Discussion
Various factors hindered the rapid detection of the outbreak. First, patients from four distant primary schools were taken to different hospitals. Second, many cases were not notified to the corresponding LPHU, despite the mandatory requirement. Third, there was an increase in viral gastroenteritis in Milan, which coincided with the Salmonella Napoli epidemic, and consequently, certain doctors did not feel that bacterial stool culture was required. Finally, the prolonged Salmonella Napoli incubation period (Fig. 1) did not allow for the early detection of the outbreak.
Although the incubation period for nontyphoidal salmonellosis is generally 6–72 h, nontyphoidal salmonellosis outbreaks with similar prolonged incubation periods have been reported (Seals et al., 1983; Nagai et al., 1999), also in a Japanese school (Matsui et al., 2004). Overall, it appears that the ingestion of low bacterial doses usually entails long incubation periods (Abe et al., 2004) and low attack rates (Matsui et al., 2004).
A fair amount of evidence supported the hypothesis that the ham eaten on 21 October was the most probable vehicle of transmission: (1) the only different meal that was delivered exclusively to all affected schools contained a “pizza margherita” and a portion of ham, (2) the pizza was reheated, while the ham was served separately, without additional treatment, and (3) the affected patients declared that they had eaten the suspected ham. However, it was not possible to determine the origin of ham contamination accurately. Our current hypothesis is that salad ingredients contaminated with Salmonella Napoli led to the contamination of tools and/or surfaces, and eventually, Salmonella Napoli contamination of the ham. Most probably, the primary contaminant was removed from salads by washing and standard treatments, while the ham was added to the meal without additional treatment. However, this hypothesis could not be verified due to the delay in the outbreak investigation.
One limitation of this study is the lack of interviews to unaffected pupils who also ate the suspected contaminated ingredient. Consequently, it was impossible to perform a case–control study to strengthen the hypothesis that ham was the likely cause. Nevertheless, according to the information provided by the canteen staff in the four affected primary schools, it appears that most children actually ate the suspected ingredient (all children stay at school for lunch every day). This fact suggests contamination with low bacterial doses and would be consistent with the long incubation period and the elevated school absenteeism observed in this epidemic.
Although the only available salad sample did not show Salmonella contamination, the fruits and vegetables may have come from different Italian producers, and the tested sample may not be representative. Evidences of Salmonella Napoli outbreaks due to the consumption of contaminated Italian rucola were reported in Sweden in 2008 and 2009 (EFSA Panel on Biological Hazards (BIOHAZ) Panel, 2013). More recently, during the months of the epidemic, there was an RASFF (Rapid Alert System for Food and Feed) notification reporting the presence of Salmonella Napoli in Italian rucola salad, which indicates the circulation of this serotype among Italian vegetables during this period (RASFF 2014.1410).
In the Salmonella Napoli outbreak reported in the United Kingdom in 1982 (Gill et al., 1983), it was found that the contaminated Italian chocolate bars contained a very low bacterial load (1.6 cells/g) (Greenwood and Hooper, 1983). Interestingly, the manufacturing plant was located very close to Paderno Dugnano (19 km away). Altogether, it seems clear that the Lombardy is a geographic reservoir of Salmonella Napoli. Currently, it is thought that the environment is the main reservoir for Salmonella Napoli (Fisher et al., 2009), but further research is required to clarify its ecology.
The outbreak reported in this article had clinical characteristics comparable with a typhoid-like salmonellosis. For example, the incubation period for Typhi and Paratyphi A is typically 7–14 days (Crump et al., 2015). Likewise, rates of bacteremia observed for Salmonella Typhi range from 5% to 30%, depending on the dose of ingestion (Waddington et al., 2014), and gastrointestinal bleeding may develop in up to 10% of hospitalized patients (Crump et al., 2015). Likewise, Salmonella Napoli infection can also cause high fever as in the case of typhoid salmonellosis.
Similar elevated rates of hospitalization and bacteremia have been reported for Salmonella Napoli infections in the past in Italy (Oggioni et al., 2010) and in England and Wales (Gill et al., 1983). Together with our results, it seems that Salmonella Napoli can easily cause invasive salmonellosis, even in people without generally accepted risk factors.
The isolate responsible for this epidemic showed resistance to aminoglycosides, which seems uncommon among Salmonella Napoli isolates (Graziani et al., 2011). Furthermore, the isolate belongs to ST474 (Huedo et al., 2015) and to eBURST group (eBG) 60 (Achtman et al., 2012), which are composed exclusively of Salmonella Napoli strains isolated from humans in France and Italy during the period 2001–2014. These results provide proof of the recurrence of Salmonella Napoli strains belonging to ST474 on human infections in this European area.
Conclusions
Reports of Salmonella Napoli are increasing in Europe and especially in northern Italy, where in 2014, it caused the biggest Salmonella Napoli outbreak ever reported in this country. Our investigations have also proved that this particular serotype can cause elevated rates of invasive salmonellosis. Overall, Salmonella Napoli infections still require research that must be carried out urgently to prevent its occurrence and avoid possible international dissemination. Furthermore, the results obtained have emphasized the importance of strengthening surveillance to improve early outbreak detection, investigation, and steps for detecting the source with the aim of halting outbreaks and improving practices.
Footnotes
Acknowledgment
This work was supported, in part, by the Ministero della Salute (IZSLER13/10-PRC2010013).
Disclosure Statement
No competing financial interests exist.