
Abstract
The objective of this study was to examine the recent trends in the epidemiology of campylobacteriosis in Israel. A Sentinel Laboratory-Based Surveillance Network for Bacterial Enteric Diseases was established in Israel by the Israel Center for Disease Control (ICDC). This network generated data on subjects from whom Campylobacter spp. was isolated in community and hospital laboratories. Further characterization of the isolates was done at the Campylobacter National Reference Laboratory. Data from these two sources were integrated and analyzed at the ICDC. Between 1999 and 2012, 40,978 Campylobacter stool isolates were reported to the ICDC by the sentinel laboratories. The incidence rate of campylobacteriosis increased from 65.7 per 100,000 in 1999 to 101.7 per 100,000 in 2012. This increase resulted from a significant rise in the incidence of campylobacteriosis in the Jewish population which, since 2009, surpassed the consistent higher incidence of the disease in Israeli Arabs. The peak morbidity in Israel consistently occurred in late spring, with a risk excess in males compared with females, in younger age groups and earlier in the life span among Arabs than among Jews and others. These results suggest that further analytical studies should be carried out to identify risk factors responsible for the increased incidence of campylobacteriosis and better direct prevention and control of the disease in Israel.
Introduction
C
In the United States, the Foodborne Diseases Active Surveillance Network (FoodNet) estimated an annual incidence rate of 13.6 cases per 100,000, but many more cases go undiagnosed or unreported, and campylobacteriosis is estimated to affect over 1.3 million persons every year (CDC, 2014).
In industrialized countries, children under the age of 5 and especially those <2 years have the highest incidence of illness (Heymann, 2008; WHO, 2011).
In this article, we present data generated by the sentinel surveillance network on agent and host-dependent characteristics of Campylobacter spp. enteric infections occurring in Israel between 1999 and 2012.
Materials and Methods
Study population
An active Sentinel Laboratory-Based Surveillance Network (SLBSN) for bacterial enteric diseases (salmonellosis, shigellosis, and campylobacteriosis) was established in Israel in 1997 at the Israel Center for Disease Control (ICDC). Eight community and hospital-based laboratories representing the different geographic regions of Israel participate in this network: Northern Israel: Haemek Medical Center, Clalit Haifa Health Maintenance Organization (HMO); Central Israel: Sheba Medical Center, Maccabi HMO Dan District Laboratory, Petah-Tikva Clalit HMO; Jerusalem District: Hadassah Medical Centers, Meuhedet HMO Laboratory; Southern Israel: Soroka Medical Center in Beer-Sheba. Clalit HMO Petah-Tikva Laboratory was added to the network in 2004.
Isolation and identification of Campylobacter species was performed at the sentinel clinical microbiological laboratories using similar routine microbiological procedures. Identification of Campylobacter spp. was carried out at the Campylobacter Reference Laboratory of the Ministry of Health in Jerusalem using standard methods (Fitzgerald et al., 2008).
Demographic data on individuals with a positive stool sample for Campylobacter spp. and isolate characterization were obtained from the sentinel laboratories and transferred to the ICDC, where they were integrated with the data on further characterization of the isolates at the Campylobacter National Reference Laboratory. A case of campylobacteriosis was defined as a subject with a positive stool culture for Campylobacter spp. at the sentinel laboratories. Isolate of the same species from the same individual within a month were counted only once.
The catchment population sizes of the different sentinel laboratories served as denominators for incidence calculation. Such data were accessed from the Central Bureau of Statistics and HMOs affiliated with the labs.
The population served by the eight sentinel laboratories was well defined by age, gender, and population group (“Jews and others” include Jews, non-Arabic Christians, and the population not affiliated with a religion; and “Arabs” include Muslims, Arab Christians, and Druze). The total population monitored by the SLBSN covers in average 47.9% of the total Israeli population. The Arabs comprised 19.2% of the sentinel surveillance population, similar to their actual proportion (20%) in the total Israeli population.
The active SLBSN operates in addition to a passive surveillance system conducted by the Israeli Ministry of Health Department of Epidemiology, where reports on notifiable diseases from laboratories and physicians are received (campylobacteriosis is a notifiable disease in Israel). These reports are incomplete as they lack information on the Campylobacter species and demographic data of cases of disease.
Data analysis
Annual incidence rates were calculated by dividing the number of laboratory-confirmed infections during the given year by the population size. Crude and age-adjusted rates were calculated for overall incidence comparisons between Jews and Arabs. Since only 31.6% of the isolates of Clalit HMO Petah-Tikva were further characterized to the level of Campylobacter species at the Campylobacter Reference Laboratory, the data from this laboratory were not included when calculating proportions and incidence rates of Campylobacter jejuni and Campylobacter coli. Time trends in incidence rates between 1999 and 2012 were examined using linear regression, with incidence rate of campylobacteriosis as the dependent variable and the year as the independent variable. To examine the statistical significance of the association between categorical variables, we used the χ 2 test. Data analysis was carried out using SAS software (Release 9.1.3; Service Pack 4; SAS Institute, Inc., Cary, NC).
Results
Between January 1, 1999 and December 31, 2012, 40,978 isolates of Campylobacter spp. were identified by the SLBSN. The number and percent of isolates reported by each laboratory and the number and percent characterized at the Campylobacter Reference Laboratory are displayed in Table 1.
HMO, Health Maintenance Organization.
During the study period there was an overall increase in the incidence of campylobacteriosis from 65.7 per 100,000 in 1999 to 101.7 per 100,000 in 2012, with some fluctuations over the years (p-value for trend <0.01) (Fig. 1). The isolation rate of Campylobacter spp. at four of the sentinel labs for which we had complete data on the number of stool samples examined for Campylobacter per month, showed a parallel increase trend, from 2.4% in 1999 to 4.6% in 2012 with similar fluctuations over the years.
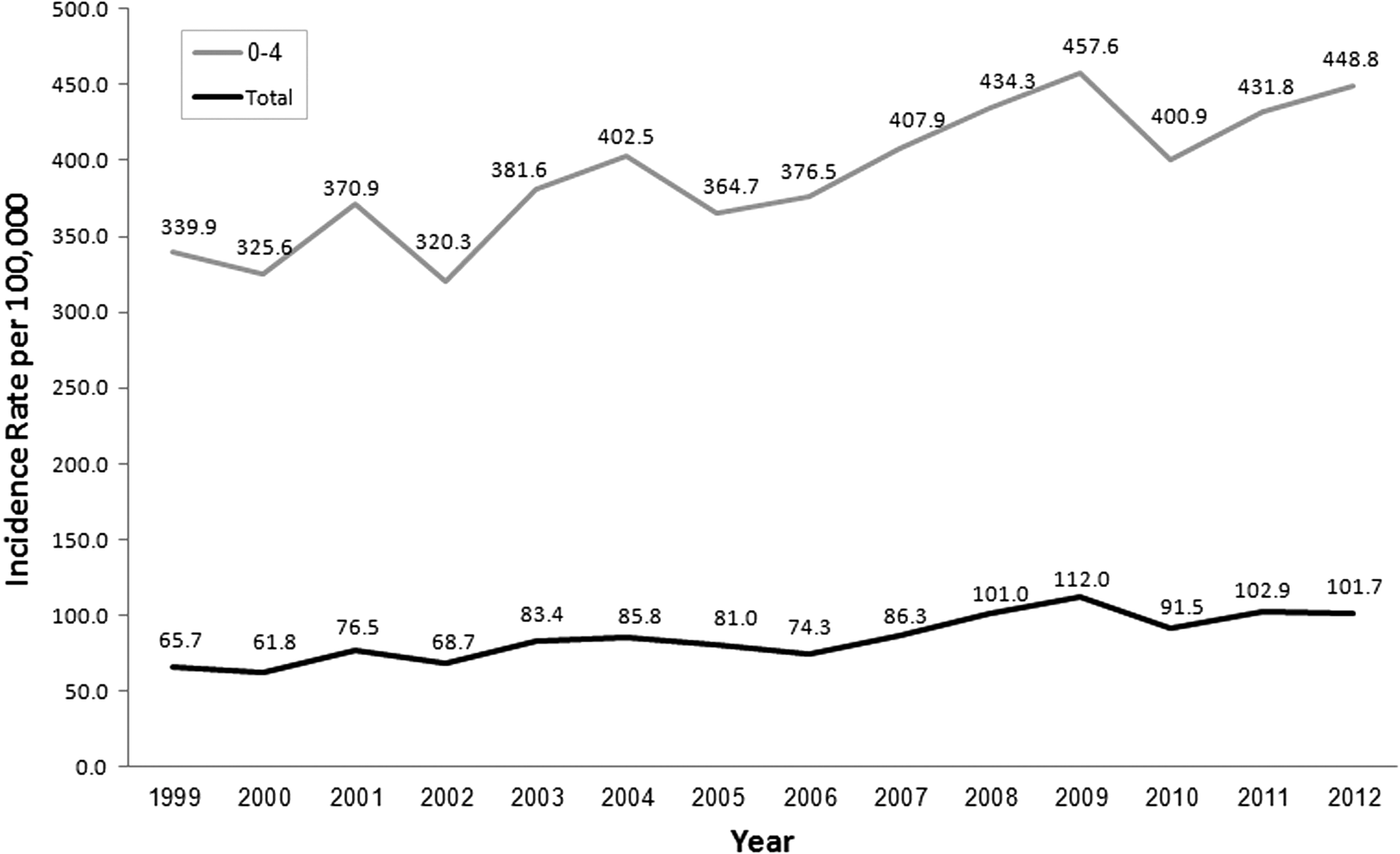
Total incidence (per 100,000) of Campylobacter isolates in sentinel laboratories and in the age group 0–4 years, 1999–2012.
The rise in incidence was seen in all age groups. The age group 0–4 showed consistently the highest incidence rates with a mean of 394.6 per 100,000 and an increase from 339.9 in 1999 to 448.8 per 100,000 in 2012 (Fig. 1).
Of all cases of campylobacteriosis, 50.3% were from children in the age group of 0–4 years. Within the total Campylobacter spp. isolates in the 0–4 age group, the highest proportion (38.3%) was identified in the first year of life.
The gender distribution of cases of campylobacteriosis in SLBSN by age groups is presented in Table 2. There was an excess of Campylobacter spp. isolates in males predominantly in the youngest age groups (Table 2). Incidence rates increased with time in both sexes at the same magnitudes (data not shown).
SLBSN, Sentinel Laboratory-Based Surveillance Network.
The incidence of campylobacteriosis was consistently the highest in May along the entire study period (Fig. 2).
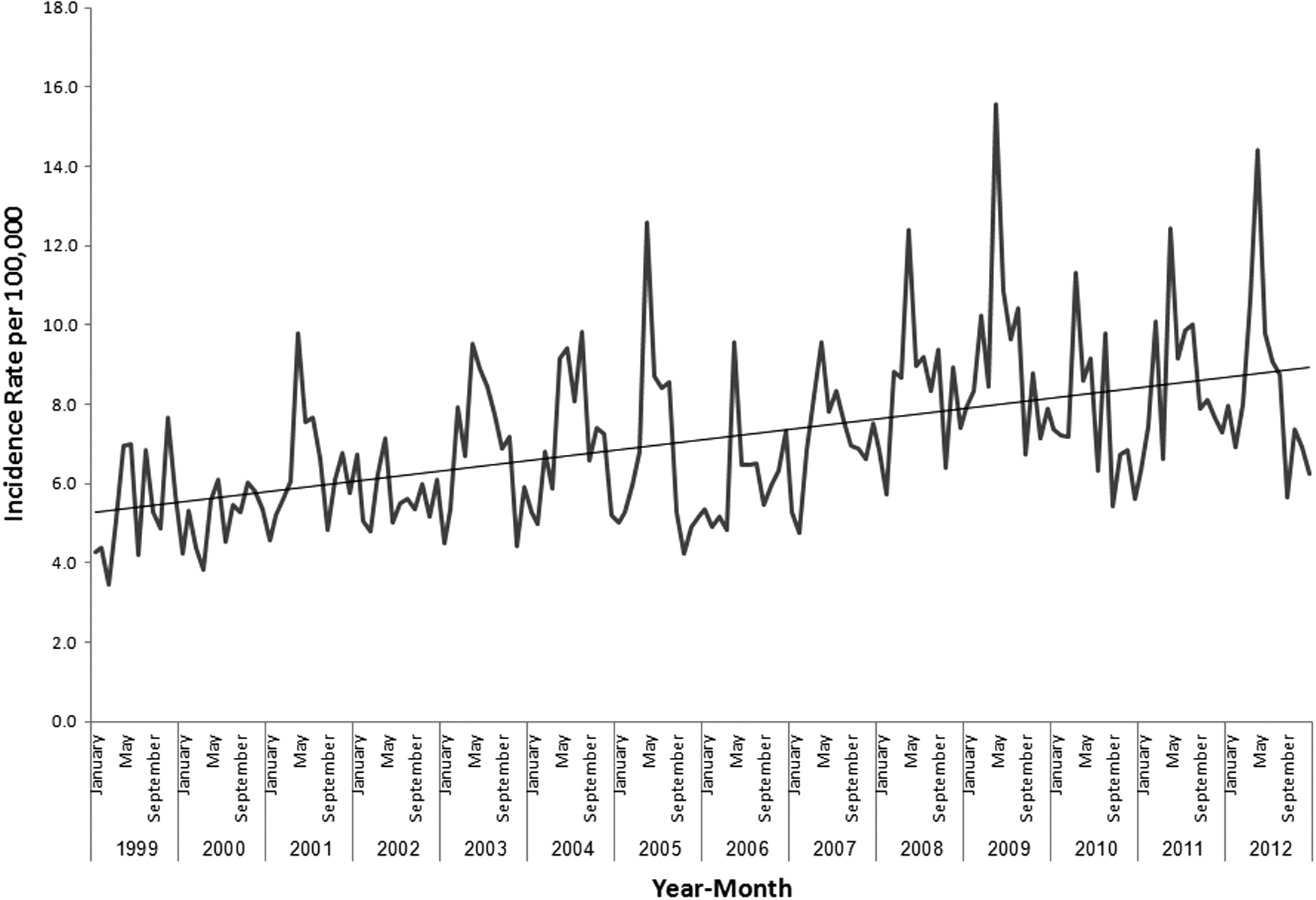
Incidence (per 100,000) of Campylobacter isolates by month in sentinel laboratories, 1999–2012.
Of the total Campylobacter spp. isolates, 8,923 (22.9%) were obtained from Arabs.
The mean age-adjusted incidence rate among Jews and others was 79.6 per 100,000 and 79.3 per 100,000 among Arabs. The age-adjusted incidence rate increased from 51.5 per 100,000 in 1999 to 103.3 in 2012 among Jews and others, and, from 73.6 per 100,000 in 1999 to 79.2 per 100,000 in 2012 among Arabs. The incidence rates of campylobacteriosis were higher among Arabs until 2008. After 2008, the incidence rates among Jews and others exceeded those of the Arab population.
The age group distribution among Jews and others and Arabs was significantly different (p-value < 0.01). About 38.6% of the isolates from Jews and others were from the age group 0–4 years as compared with 88.6% of the isolates from Arabs (Fig. 3).
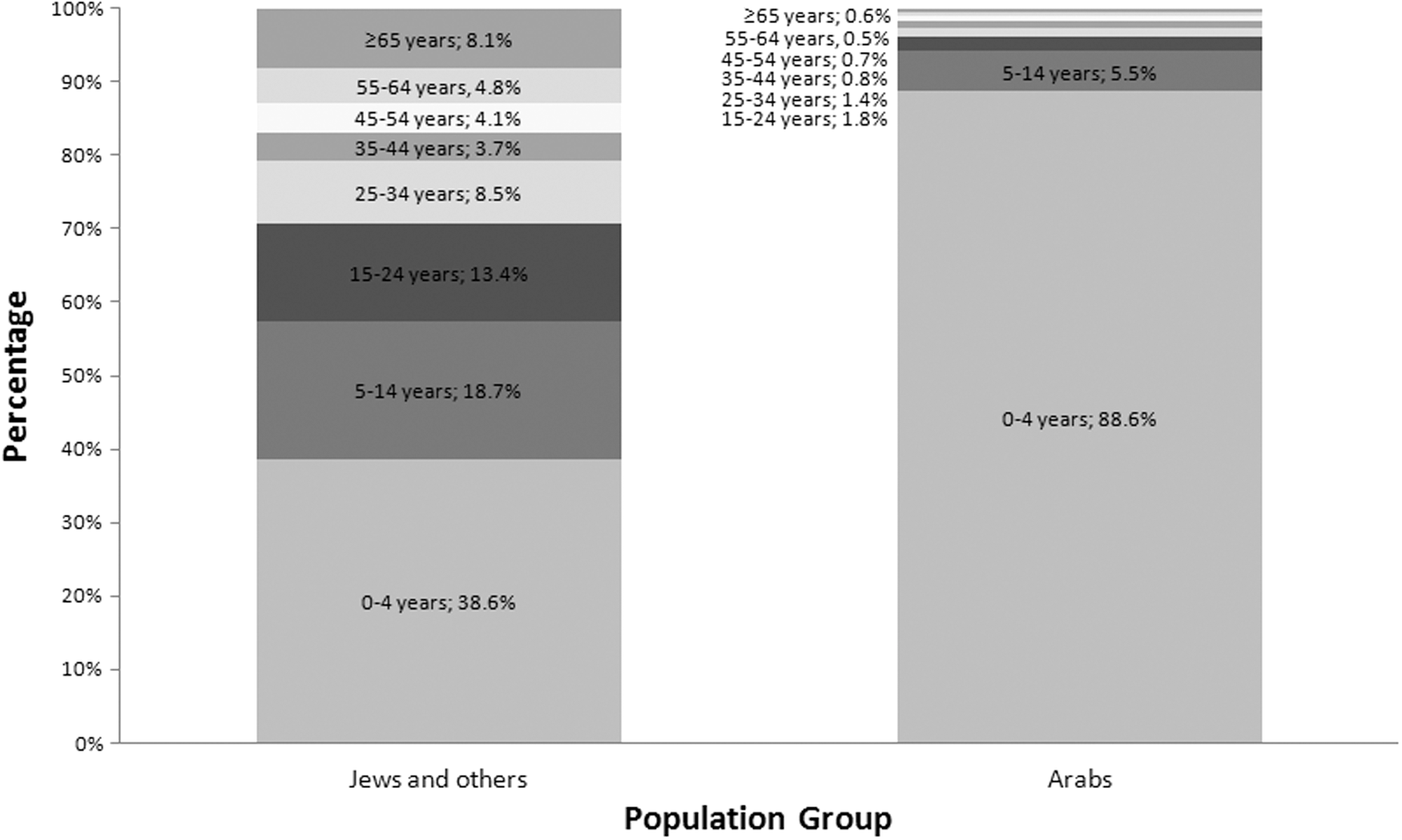
Distribution of Campylobacter isolates by population group and age group in sentinel laboratories, 1999–2012.
During the study period, the incidence rates of C. jejuni and C. coli remained stable (p-value for trend >0.05) among Arabs, while both species increased significantly among Jews and others (C. jejuni: 39.6 per 100,000 in 1999 to 79.1 per 100,000 in 2012 (p-value for trend <0.01); C. coli: 4.4 per 100,000 in 1999 to 12.1 per 100,000 in 2012 (p-value for trend <0.01) (Fig. 4).
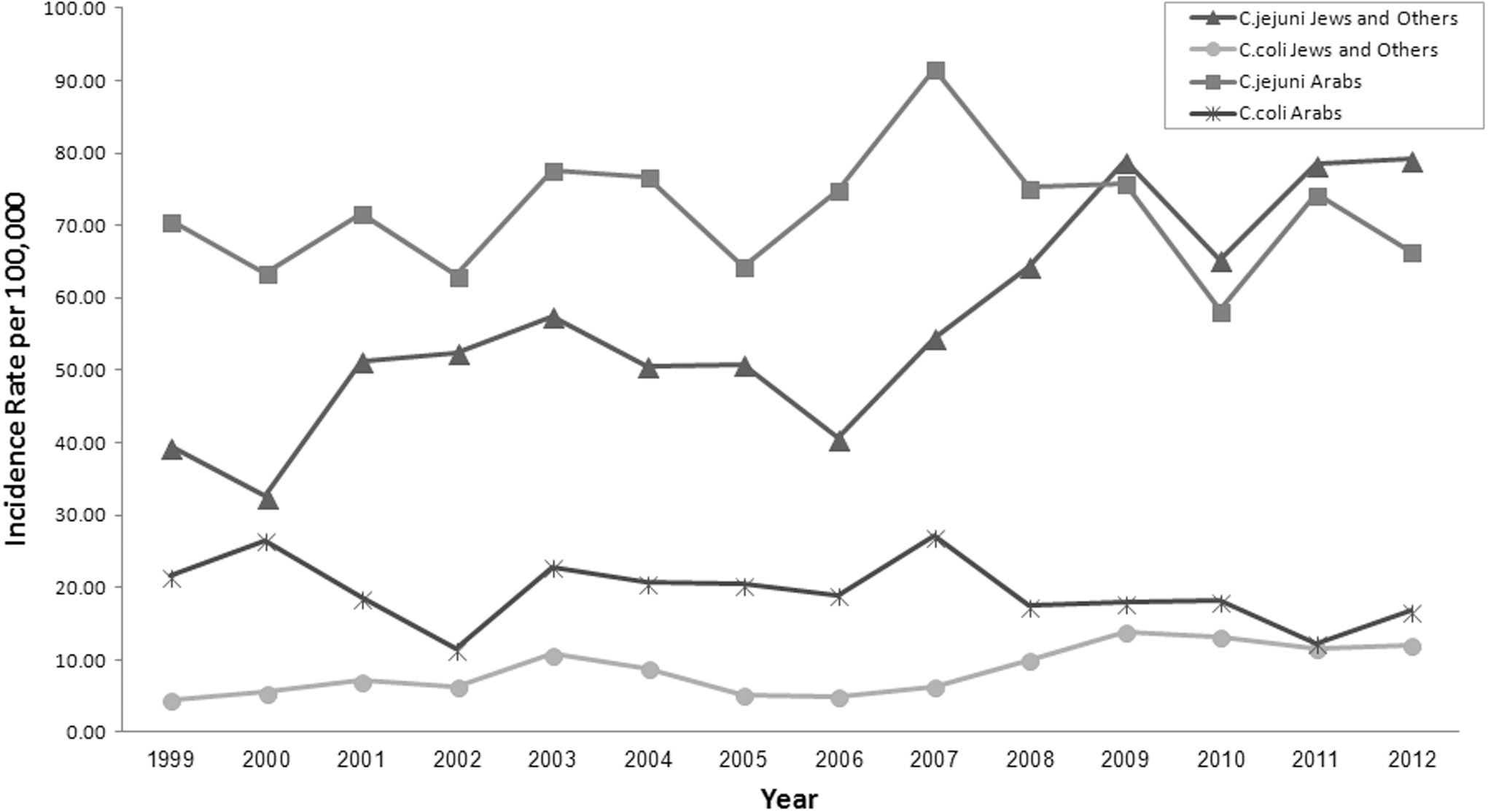
Incidence (per 100,000) of Campylobacter species by population group in sentinel laboratories, 1999–2012.
Of 23,049 Campylobacter spp. isolated from Jews and others, 3,031 (13.2%) were C. coli as compared with 1,766 (20.1%) C. coli finally defined among 6,619 Campylobacter spp. isolated from Arabs (p-value < 0.01). There were no differences in the host characteristics such as age and gender of Campylobacter isolates that were or were not typed at the Campylobacter Reference Laboratory.
Discussion
This study summarizes 14 years of active sentinel laboratory-based surveillance of campylobacteriosis in Israel. The mean incidence rate of campylobacteriosis during the study period was high (mean of 86.7 per 100,000) in comparison to other developed countries (SFVO, 2012; CDC, 2014; FSAI, 2014). The FoodNet, which covers 15% of the U.S. population and is similar in structure to the Israeli SLBSN, reported an incidence rate of campylobacteriosis of 13.6 per 100,000 in 2010 (CDC, 2014). In Ireland, the Health Protection Surveillance Centre reported an incidence rate of 52.0 cases of campylobacteriosis per 100,000 in 2012 (FSAI, 2014). In Switzerland, campylobacteriosis cases account for 100 reports per 100,000 inhabitants (SFVO, 2012). It should be noted that inter-country comparisons of overall incidences of disease must be taken with caution since incidence rates are associated with each country's organization of the health system, diagnostic practices, surveillance systems, and other factors.
The data of the active SLBSN showed a clear increase in the incidence rate of campylobacteriosis from 65.7 per 100,000 in 1999 to 101.7 per 100,000 in 2012. It has to be emphasized that all stool samples are routinely tested in the sentinel labs for Campylobacter, Shigella, and Salmonella. There were no changes in the reporting system, reference lab practices, availability of materials or personnel at each sentinel laboratory. There was no change in the type or level of education and training of physicians in Israel during the study period that might have caused a change in their knowledge of Campylobacter and campylobacteriosis. We found a parallel trend with similar fluctuations over the years in the isolation rate of Campylobacter spp. further supporting the validity of the incidence data.
The incidence rate of campylobacteriosis reported by the Department of Epidemiology at the Israeli Ministry of Health, based on the national passive surveillance system followed the same pattern of increase that began in 1997, but the incidence rates were lower (from 38.1 per 100,000 in 1999 to 66.3 per 100,000 in 2012) than those identified in the same period by the SLBSN (ICDC 2012; ICDC 2014), most likely a result of under-reporting. There were no outbreaks of campylobacteriosis that were detected by the SLBSN throughout the period of the study though we cannot rule out occasional occurrence of clusters of disease supporting the observation on the paucity of epidemic occurrence of campylobacteriosis (Yu et al., 2010; WHO, 2011; Taylor et al., 2013; CDC, 2014). We are aware of only four published reports on outbreaks of campylobacteriosis in Israel in the last 30 years (Rogol et al., 1983; Cohen et al., 1984; Hershkowici et al., 1987; Srour et al., 2002). An increase in the incidence rate of campylobacteriosis in the last decade was also reported from other countries all over the world (Baker et al., 2007; SFVO, 2012; CDC, 2013; EFSA, 2013; Kaakoush et al., 2015). Recently, Kaakoush et al. reviewed data from different studies showing a dramatic increase in campylobacteriosis in North America, Europe, and Australia. Data from parts of Africa, Asia, and the Middle East over the last ten years, indicate that campylobacteriosis is highly endemic in these areas, especially in children (Kaakoush et al., 2015). In the United States, the estimated incidence of campylobacteriosis monitored by FoodNet was higher in 2012 compared with 2006–2008 (14% increase) (CDC, 2013). Data from 27 member states of the European Union (EU) showed that the number of confirmed cases of campylobacteriosis followed a significant increase trend between 2008 and 2011 (EFSA, 2013). In Switzerland, the incidence rate of campylobacteriosis increased since 2005 and has become the most common food-associated notifiable illness (SFVO, 2012). In New Zealand, the incidence of notified campylobacteriosis has also risen steadily for more than two decades (Baker et al., 2007).
The reason for the significant increase in the incidence of campylobacteriosis in Israel, and in other countries, is still unclear. Single and combined factors, such as an increase in poultry consumption, a higher level of contamination of poultry with Campylobacter spp., and eating outside home might be responsible for this trend (Baker et al., 2007; FAO, 2014; Wei et al., 2015). Although studies have shown that a high percentage of chicken (70%) are contaminated with Campylobacter species (Harrison et al., 2001; Zhao et al., 2001; Wei et al., 2015) and are the main reservoir for human infections, environmental sources may also result in direct human exposure and contamination in the food processing industry (Whiley et al., 2013).
We found a clear and consistent pattern of highest rates of campylobacteriosis in May. This pattern is different from that of salmonellosis in Israel, with highest and consistent incidence rates in July and August (Bassal et al., 2012) and also different from that of shigellosis with winter and midsummer peaks of morbidity (Cohen et al., 2014). A very similar seasonal pattern with morbidity peaks in May and June was reported from England and Wales, suggesting that one or more seasonal factors related to environmental and climatic conditions could be responsible for the excess of human exposure and transmission of Campylobacter (Nichols, 2005). The sharp increase in the density of the fly population during this period of the year under favorable environmental temperature and humidity was proposed as a significant means of enhanced transmission of Campylobacter to humans (Ekdahl et al., 2005; Nichols, 2005).
The age distribution of campylobacteriosis was consistent with that reported by others (Baker et al., 2007; Heymann, 2008; WHO, 2011; CDC, 2014; Schielke et al., 2014) with high incidence in the age group 0–4 and peak incidence in the first year of life. A possible higher tendency for physicians to have young children perform stool test than other age groups may contribute at least in part to the excess of Campylobacter spp. isolates in this age group. Early exposure to the pathogen and naturally acquired immunity leading to a lower proportion of susceptibles are the most probable reasons for the lower infection rates later in life (Randremanana et al., 2014) and possibly for the predominance of sporadic versus epidemic morbidity (Taylor et al., 2013). Weinberger et al. (2013) also reported an increase in the incidence rate of campylobacteriosis in Israel in all age groups (mostly evident in very young children), which was explained in part by a noticeable transition from the consumption of frozen to fresh poultry meat (Weinberger et al., 2013). Poultry produced in Israel is extensively consumed by both Jews and Arabs.
An interesting finding of this study is the much higher proportion of Campylobacter spp. isolates in the 0–4 year age group among Arabs (88.6%) compared with Jews and others (38.6%). This is probably the result of earlier exposure to Campylobacter spp. in Arabs living mostly in rural settlements and perhaps being at a higher risk of exposure to domestic animals carrying the bacteria (e.g., chicken). Such differences in the age distribution of isolates of Campylobacter spp. between ethnic groups within one country were also reported from Birmingham, England in Asian versus non-Asian inhabitants (Manaseki et al., 2004).
In Israel, healthcare is delivered in a universal fashion thanks to the National Health Insurance Law and participation in a medical insurance plan is compulsory. Thus, there is no difference between the Arabs and Jews living in Israel in the accessibility to healthcare services and the health services are supplied for free for both. Nevertheless, we cannot rule out the possibility that there might be a differential utilization of medical services and health-seeking behavior in respect to diarrheal diseases among the Jewish and Arab subpopulations possibly leading to a differential underestimation of the burden of campylobacteriosis among Israeli Arabs in general and in older age groups, in particular.
Our finding on the excess of Campylobacter infections in males corroborates other reports (Gillespie et al., 2008; Schielke et al., 2014) and is consistent with a similar pattern observed with other infectious diseases mostly in children (Green, 1992).
C. jejuni was the predominant species of Campylobacter, with C. coli as the second most important. The predominance of C. jejuni relatively to C. coli and the other species of Campylobacter is common but varies quantitatively as reported in England and Wales, China, and the Republic of Ireland with a prevalence of 92%, 89% and 67%, respectively (Gillespie et al., 2008; Chen et al., 2011; Madden et al., 2011).
It has been shown that the risk of C. coli infection in comparison with C. jejuni is higher in people older than 19 years, in people who live in rural areas and during the summer months (Roux et al., 2013). The fact that Israeli Arabs primarily reside in rural areas may, in part, explain our finding that a higher percent of C. coli among Campylobacter spp. is isolated among Arabs as compared Jews and Others.
The data generated by the active laboratory-based surveillance of campylobacteriosis have showed that the disease is highly endemic in Israel, with incidence rates higher than those reported from other developed countries and increasing in the last decade and a half. Data on the level of infestation with Campylobacter spp. of the livestock in Israel, especially poultry, are needed. Further analytical studies are necessary to identify factors associated with an increased risk of disease in humans to better direct prevention and control of the disease in Israel. In New Zealand, where a dramatic increase in the incidence rate of campylobacteriosis was observed between 1980 and 2006, a range of voluntary and regulatory interventions were made to reduce Campylobacter spp. contamination of poultry including the levels of primary production, processing, retail and consumer (Sears et al., 2011). The results of these actions lead to 54% decline in the incidence rate of campylobacteriosis in 2008, compared with the average annual rate of 2002–2006 (Sears et al., 2011).
Conclusions
We report on an increase in the incidence of campylobacteriosis in Israel in the last 15 years. The peak morbidity occurred consistently in late spring, with a risk excess in younger age groups, in males compared with females, as well as earlier in the life span among Arabs compared with Jews and others. C. jejuni was the predominant species of Campylobacter, with C. coli as the second most important. A concerted effort of veterinary and public health authorities is necessary to stop the rise in the incidence of the disease and ultimately reduce the burden of campylobacteriosis in humans in Israel.
Footnotes
Acknowledgments
We thank Nadia Pekurovski for her assistance in the data collection of the Sentinel Laboratory-Based Surveillance Network. The study was supported in part by a grant from Nuclear Threat Initiative, Washington DC in frame of the Middle East Consortium for Infectious Diseases Surveillance conferred to Tel-Aviv University.
Disclosure Statement
No competing financial interests exist.