
Abstract
Campylobacter spp. is the most common gastrointestinal pathogen worldwide with a very low reported incidence in Italy. In November of 2013, local and national public health authorities investigated an outbreak caused by Campylobacter jejuni among children in a kindergarten in Northern Italy. A case was defined as a child who had diarrhea with a laboratory-confirmed diagnosis of C. jejuni between 11 and 30 November. Stool samples from the kindergarten kitchen staff and environmental samples from the kitchen were examined for enteric pathogens. As food leftovers were not available, the menu logbook of the refectory was reviewed to identify a possible source of the outbreak. C. jejuni strains were tested for antimicrobial susceptibility and subtyped by pulsed field gel electrophoresis (PFGE) and multilocus sequence typing (MLST). We identified 20 cases among 247 schoolchildren (attack rate = 8%), all who reported having lunch in the kindergarten. The stools from the kitchen staff as well as the environmental samples were negative for enteric pathogens. The identified outbreak strains (n = 5) were sensitive to all of the antimicrobials tested; the first four strains showed an identical PFGE profile, whereas the fifth strain showed a PFGE pattern similarity of 89%. Using MLST, all five strains were assigned to a single sequence type (ST), ST451 (clonal complex, CC21); this was the first identification of ST and the third reported outbreak of C. jejuni in Italy. Molecular typing confirmed that most of the cases belonged to a clonal cluster supporting the hypothesis of a common source; however, the source was not identified. Due to a delayed start of the investigation, it was not possible to perform any microbiological evaluation of the food consumed.
Introduction
C
Campylobacter is transmitted to humans through the consumption of raw milk, water, or contaminated meat, particularly in poultry (Silva et al., 2011). The majority of cases are sporadic and the route of infection is infrequently established (Altekruse et al., 1999). Outbreaks are well documented but rarely reported, although in Europe they represent 8.5% of all food-borne outbreaks (EFSA and ECDC, 2015).
Campylobacter infections are not subject to mandatory notification in several European countries (EFSA and ECDC, 2015), including Italy. Campylobacter isolates are reported in Italy on a voluntary basis by local and regional reference laboratories to the sentinel surveillance system for enteric pathogens (Enter-Net Italia, coordinated by the Istituto Superiore di Sanità, Rome, Italy; available at
Until 2009, the system registered up to 500 notifications per year but, from 2010, there was a noted increase, reaching 1257 notifications in 2014. Despite this increase in notifications, these data may underestimate the real burden of the disease due to the voluntary nature of the reporting system. As of the present time, only two outbreaks caused by Campylobacter have been reported in Italy (Amato et al., 2007; Armani et al., 2014).
The aim of this study was to describe both the microbiological and epidemiological features of the outbreak of C. jejuni that occurred in a kindergarten class in a small town in the province of Bergamo in Northern Italy.
Materials and Methods
Epidemiological investigation
On November 18, 2013, a pediatrician informed the local public health authorities of a child experiencing gastrointestinal symptoms. The child was tested for the presence of Salmonella spp., Shigella spp., and Campylobacter spp., and the laboratory-reported positive result for Salmonella spp. on the 31st October. The local public health authorities examined school attendance records to verify whether there had been an increase of absent children during the same period as the infected child. We interviewed parents of children absent during the same period and collected the following information: whether the children had gastrointestinal or other symptoms (diarrhea, abdominal pain, vomiting, nausea, or fever) between 11 and 30 November and whether the children had been tested for the presence of Salmonella spp., Shigella spp., and Campylobacter spp. If the children had been tested, the parents were asked for which laboratory the test was performed and for the laboratory diagnosis. If the children had not been tested, the parents were asked to have them tested for the presence of Salmonella spp., Shigella spp., and Campylobacter spp. Stool samples from the kindergarten staff (n = 15) were examined for the presence of Salmonella spp., Shigella spp., and Campylobacter spp. as described previously (Caprioli et al., 1996).
Descriptive epidemiology
We defined a probable case as a child with diarrhea between 11 and 30 November who attended the kindergarten and we defined a confirmed case as a child with diarrhea between 11 and 30 November who attended the kindergarten and had a laboratory-confirmed diagnosis of C. jejuni.
We collected demographic information (age and sex) and clinical characteristics (symptom and onset of disease) of confirmed cases by interviewing the parents. Since food leftovers were not available for microbiological investigation, we reviewed the kindergarten's menus to identify a likely food source of the outbreak. In addition, we interviewed the kindergarten staff to determine whether milk was served or whether any excursions were taken during the 3 days before the onset of the outbreak.
Environmental investigation
The kitchen was inspected to evaluate the procedures used in food handling, preparation, and service. Environmental samples from the kindergarten kitchen (six samples from kitchen counter and four samples from kitchenware) were collected and examined for Salmonella spp., Shigella spp., and Campylobacter spp.
Campylobacter strains
Five strains isolated from children who attended the kindergarten were sent to Istituto Superiore di Sanità from a local laboratory of Bergamo who participated in the Enter-Net surveillance system. The laboratory also sent 11 other strains: 5 from children and 6 from adults, isolated during November 2013 from the general population in the Bergamo province. These 11 strains were included for microbiological and molecular comparison of the outbreak strains.
Antimicrobial susceptibility test
All strains were tested for antimicrobial susceptibility by the disk diffusion method following EUCAST guidelines (available at
Pulsed field gel electrophoresis
Pulsed field gel electrophoresis (PFGE) was performed using SmaI as a restriction enzyme (New Englands Biolabs, Ipswich, MA), according to CDC protocol (available at
Dendrogram and cluster analysis were performed using algorithms available in the BioNumerics software package (v. 6.6; Applied Maths, Sint-Martens-Latem, Belgium). The similarity between chromosomal fingerprints was scored using the Dice coefficient. The unweighted pair group method with arithmetic means (UPGMA) with a 1.00% tolerance limit and 1.00% optimization was used to obtain the dendrogram. DNA profiles differing by two–three DNA fragments were considered as closely related, according to Tenover et al. (1995).
Multilocus sequence typing
Strains were characterized by multilocus sequence typing (MLST) using the method described by Dingle et al. (2001). DNA was isolated from bacterial cultures using a Wizard DNA isolation kit according to the manufacturer's recommendations (Promega Corporation, Madison, WI). PCR amplification of the seven housekeeping genes was carried out as described previously (Dingle et al., 2001). Amplification products of the correct size were identified, purified, and prepared for sequencing using an ISOLATE II PCR and Gel Kit (Bioline, London, United Kingdom).
The nucleotide sequence was determined by using appropriate primers and BigDye reaction mix (Applied Biosystems, Foster City, CA) on an ABI prism 3730 automated DNA sequencer. Sequence data were collated and alleles were assigned using the Campylobacter PubMLST database (
Results
Epidemiological investigation and outbreak description
In the review of the attendance records, we found that 61 children were absent on the 18th of November. We were able to collect information from 41 parents by telephone, of which 33 reported that their children had experienced gastrointestinal symptoms (probable cases). Twenty children, among the 247 children who attended the kindergarten, had microbiological confirmation (confirmed cases; attack rate = 8%). Fourteen of the confirmed cases were male with a median age of 4 years (range: 2–5 years). Fever (75%) and abdominal pain (70%) were the most frequent symptoms. Eighteen cases occurred between 14 and 17 November and the last two cases occurred on the 22nd of November. Considering the case distribution and the incubation period of Campylobacter spp. (2–5 days), we examined the kindergarten menus between 11 and 13 November. Cheese, vegetables, potatoes, fruit, braised bovine meat, and turkey roast had been served during that period of time. No milk had been served and no excursions were taken from the kindergarten in the 3 days before the onset of the outbreak. Kitchen inspection did not reveal any apparent lack of hygiene measures in food preparation.
Microbiological results
Both environmental and stools samples from kitchen staff were negative for Salmonella spp., Shigella spp., and Campylobacter spp.
All of the outbreak strains were sensitive to the antimicrobials tested, whereas the strains isolated from the general population showed different patterns: three were sensitive to all antimicrobials tested, three were resistant to ciprofloxacin, and five were resistant to ciprofloxacin and tetracycline.
All isolates were typeable by PFGE. As shown in Figure 1, four out of five strains isolated from the children had an undistinguishable PFGE profile. The remaining strain (100/20/13) showed a PFGE similarity of 89% with the other outbreak strains. This strain had the PFGE profile identical to a strain (100/6/13) isolated from an adult, who apparently did not have any relationship with the kindergarten or any children who attended the kindergarten. This adult reported having consumed meat in a restaurant in the days before the onset of symptoms, which occurred on the 25th November, 3 days after the end of the outbreak. No further epidemiological investigation regarding the adult case was performed. All of the other strains that were not related to the outbreak showed a PFGE similarity ≤60% to the outbreak strains.
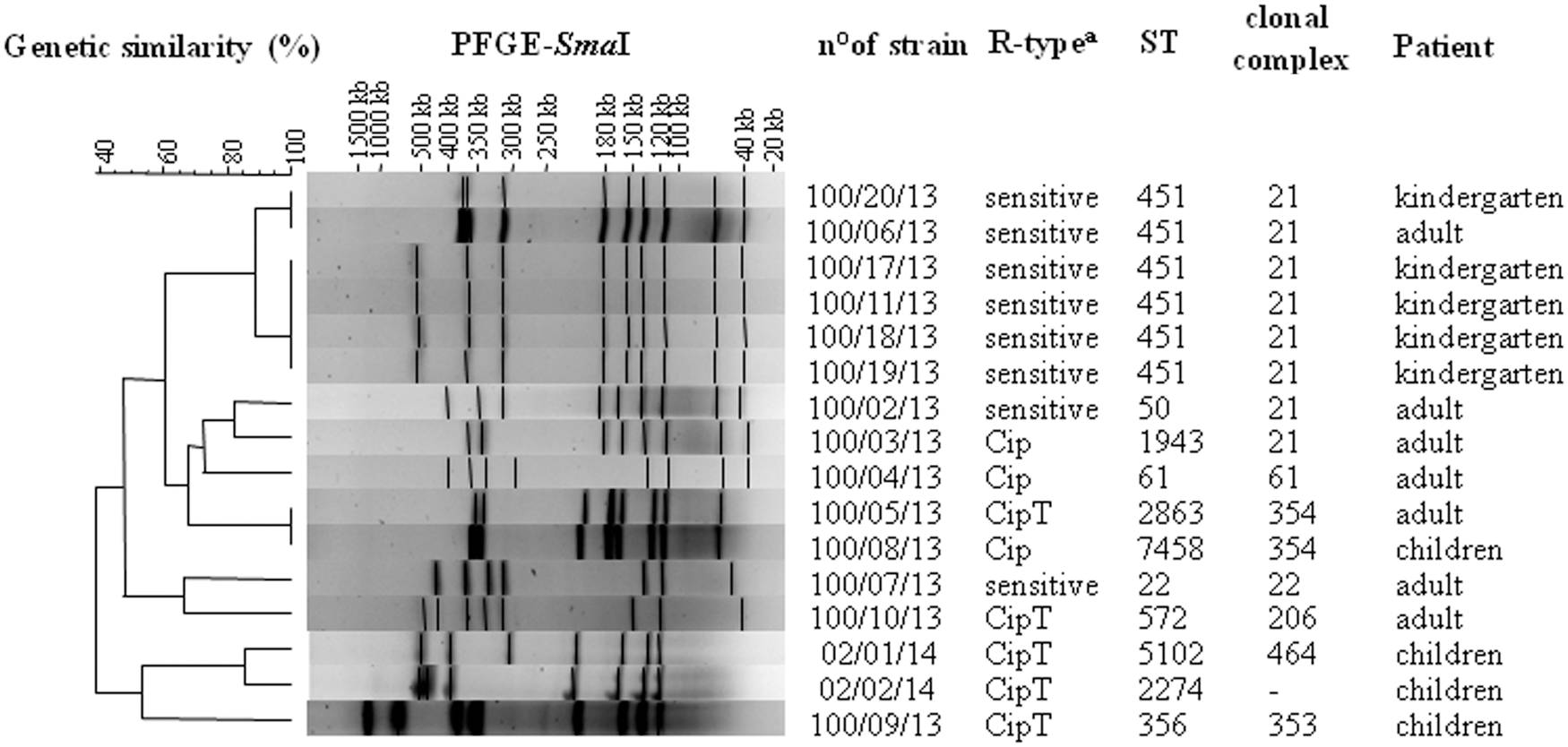
Dendrogram generated by Bionumerics software showing the cluster analysis of pulsed field gel electrophoresis (PFGE) profiles of the 15 Campylobacter jejuni strains analyzed in this study. Antimicrobial susceptibility, sequence type (ST), clonal complex (CC), and patient also shown. aCip, ciprofloxacin; T, tetracycline.
Using the MLST technique, the four strains with the same PFGE profile were assigned to a single ST, ST451 (clonal complex, CC21), together with the isolates nos. 100/6/13 (adult) and 100/20/13 (children) (Fig. 1). Among the nonoutbreak strains, only two (nos. 100/2/13 and 100/3/13) belonged to CC21, but had a different ST, whereas the other strains belonged to STs and clonal complexes (CCs) that were different from the outbreak strains. We also found a new allele in the tkt locus of strain no. 100/08/13, which subsequently led to a definition of a new ST, ST7458.
Discussion
Here, we described a campylobacteriosis outbreak that occurred in a kindergarten in Northern Italy that was detected by a pediatrician by chance who identified a single case of salmonellosis. To our knowledge, this is the third C. jejuni outbreak described in Italy to date (Amato et al., 2007; Armani et al., 2014). In both previous cases, the source of the outbreaks was traced to consumption of raw milk. Although the source of outbreak here described was not identified, consumption of raw milk was excluded as the source.
Molecular typing showed that the outbreak strain belonged to a unique ST (ST451) clonal complex 21 (CC21). According to the literature, ST451 is relatively infrequent. It has been described in 24.7% of strains from poultry and in 1.6% of human strains isolated in New Zealand (Mullner et al., 2009). In Finland, ST451 has been described in five strains isolated from bovines but not in humans (de Haan et al., 2010). In the Campylobacter PubMLST database, there are only four strains belonging to ST451, all of which were isolated from humans: two strains isolated in Japan, one strain isolated in Australia, and one strain isolated in The Netherlands (
The ST451 belongs to CC21, one of the largest CCs found to date, comprising 26% of all the isolates submitted to PubMLST, with a total of 152 different STs (
Only two studies have evaluated MLST on strains isolated from poultry, humans (Piccirillo et al., 2014), and turkey (Manfreda et al., 2016). Piccirillo et al. (2014) reported that 47.8% of strains isolated from chickens belonged to CC21 and that this CC was found in a strain out of 11 strains of human origin. The CC21 was also identified in 23.4% of turkey isolates in a study conducted in Northern Italy (Manfreda et al., 2016). Other studies performed in Italy have shown that the CC21 is relatively common in strains isolated from cattle and bulk tank milk (Bianchini et al., 2014a; Bianchini et al., 2014b).
In our study, both PFGE and MLST were useful to assess the strains in a clonal cluster isolated from the outbreak cases (Taboada et al., 2013). Although PFGE results have been reported as not highly reproducible (Ahmed et al., 2012), in our study, this technique was able to discriminate strains within the same MLST. The discrepancy between MLST and PFGE may be explained by the technique itself. MLST investigates the variation in slowly evolving housekeeping genes (Ahmed et al., 2012); therefore, this technique is not able to identify differences occurring in other parts of the genome. PFGE, however, is able to detect substantial genetic changes, such as rearrangements, deletions, and insertions, appearing as band differences in PFGE profiles (Barrett et al., 2006).
The difference in the PFGE profiles of our strains, shown in Figure 1, consists of a fragment of ∼500 kb present in the four strains isolated but missing in strains 100/20/13 and 100/6/13; instead, these two strains have a fragment of 350–400 kb. The most likely explanation is that these strains (100/20/13 and 100/6/13) underwent intragenomic rearrangements that led to a deletion of ∼100 kb. These types of modifications, responsible for the nonclonal population structure of C. jejuni, may occur very quickly even in the absence of selective pressure (de Boer et al., 2002; Kuusi et al., 2004; Steinbrueckner et al., 2001) or during an outbreak (Kuusi et al., 2004). Kuusi et al. (2004) analyzed nine strains, of which eight showed an identical PFGE profile and one showed a different PFGE profile.
Despite the differences in PFGE profiles between the adult strain and the kindergarten outbreak strains, they all had the same MLST, supporting a possible epidemiological link; therefore, a common source cannot be excluded. However, the molecular typing showing strain similarity was carried out one month after the outbreak, which was too late to perform a proper investigation regarding the restaurant where the meat was consumed.
Conclusions
Here, we describe one of the few C. jejuni outbreaks in Italy. Molecular analysis allowed for the detection of ST451 for the first time, and these results indicated that circulation of this ST is likely underestimated. Such an ST could represent a marker to identify the source of infection if the outbreak investigation had been carried out in a timely manner. Our study demonstrates the importance of rapid reporting of gastroenteritis cases to local public health authorities to perform a timely epidemiological and microbiological investigation. Mandatory notification for Campylobacter would be useful for better estimation of the disease, as well as identification of the source of infection and proper control measures to protect public health.
Footnotes
Acknowledgments
We are grateful to Dr. Aftab Jasir for discussion and helpful suggestions. We would also like to thank Dr. Laura Busi for her technical assistance.
This work was partially supported by a grant from the Italian Ministry of Health, Centro Nazionale per la Prevenzione ed il Controllo delle Malattie (CCM) [project “Sorveglianza delle malattie trasmesse da alimenti e acqua (EnterNet): adeguamento del sistema italiano al quadro normativo europeo” 5 M10-1616-2014].
Authors' Contribution
C.L. designed the study, wrote the article, performed PFGE, and contributed to epidemiological data analysis; A.M.D. performed antimicrobial susceptibility tests, MLST, and cluster analysis using the BioNumerics software; L.T. coordinated the local investigation and collected epidemiological information; C. F. provided the strains; M.P. performed strain isolation and identification; T. K. performed epidemiological analysis; F.D'A. contributed to epidemiological analysis; I.L. designed and supervised the study; A.M.D., T.K., F.D'A., and I.L. read and revised the article. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.