
Abstract
Introduction:
Molecular subtyping of pathogens is critical for foodborne disease outbreak detection and investigation. Many clusters initially identified by pulsed-field gel electrophoresis (PFGE) are not confirmed as point-source outbreaks. We evaluated characteristics of clusters that can help prioritize investigations to maximize effective use of limited resources.
Materials and Methods:
A multiagency collaboration (FoodNet) collected data on Salmonella and Escherichia coli O157 clusters for 3 years. Cluster size, timing, extent, and nature of epidemiologic investigations were analyzed to determine associations with whether the cluster was identified as a confirmed outbreak.
Results:
During the 3-year study period, 948 PFGE clusters were identified; 849 (90%) were Salmonella and 99 (10%) were E. coli O157. Of those, 192 (20%) were ultimately identified as outbreaks (154 [18%] of Salmonella and 38 [38%] of E. coli O157 clusters). Successful investigation was significantly associated with larger cluster size, more rapid submission of isolates (e.g., for Salmonella, 6 days for outbreaks vs. 8 days for nonoutbreaks) and PFGE result reporting to investigators (16 days vs. 29 days, respectively), and performance of analytic studies (completed in 33% of Salmonella outbreaks vs. 1% of nonoutbreaks) and environmental investigations (40% and 1%, respectively). Intervals between first and second cases in a cluster did not differ significantly between outbreaks and nonoutbreaks.
Conclusions:
Molecular subtyping of pathogens is a rapidly advancing technology, and successfully identifying outbreaks will vary by pathogen and methods used. Understanding criteria for successfully investigating outbreaks is critical for efficiently using limited resources.
Introduction
A
Successful identification of the source of an outbreak and mitigation of ongoing risk depends on rapid detection and investigation of identified clusters of illness. Determining whether individual cases might be epidemiologically related can pose substantial challenges to investigators. Molecular subtyping of bacterial isolates, particularly the use of pulsed-field gel electrophoresis (PFGE), has had a dramatic impact on outbreak detection and investigation, allowing laboratory identification of clusters of cases with possible epidemiologic linkages, or related to environmental or food isolates. PulseNet, the national molecular subtyping network of the CDC and public health laboratories, routinely collects and compares PFGE data on selected enteric bacterial isolates from all participating jurisdictions to identify clusters of illness. Few studies have evaluated specific parameters or characteristics that might help epidemiologists prioritize investigation of clusters to maximize effective use of limited resources (Rounds et al., 2010, 2012). We performed a prospective study to assess factors that predict whether PFGE-identified clusters of Salmonella and E. coli O157 are ultimately confirmed to be outbreaks.
Materials and Methods
FoodNet is a collaboration among CDC's Emerging Infections Program, 10 participating state health departments, the U.S. Department of Agriculture's Food Safety and Inspection Service, and the U.S. Food and Drug Administration. FoodNet conducts active population-based surveillance for laboratory-confirmed infections, including Salmonella and E. coli O157. Data were collected in seven participating FoodNet sites (Connecticut, Maryland, Minnesota, New Mexico, Oregon, Tennessee, and selected counties in Colorado) from January 2009 to December 2011.
Submission of all Salmonella and E. coli O157 isolates to the state public health laboratory was required by all participating states, except Colorado, which requested submission and estimated compliance at >95%. Serotyping and PFGE subtyping were performed on all submitted isolates (Boxrud et al., 2010). For this study, a PFGE cluster was defined as ≥2 isolates of Salmonella or E. coli O157, with the same serotype and indistinguishable PFGE patterns by two enzymes, with isolation dates within 30 days of each other and in the same state. All cases of Salmonella and E. coli O157 were interviewed routinely by participating health departments as soon as they were reported. Clusters were investigated to determine epidemiological links among cases and possible sources of infection. The date of cluster identification was defined as the date of state public health laboratory receipt of the second isolate in a cluster.
A standard form was used to collect information on each cluster, including the number of matching isolates, dates isolates were received at the public health laboratory and reported to epidemiologists, and temporality among cases. Information on the epidemiologic methods used and outcome of investigations was also collected.
Final classification of a PFGE cluster as a confirmed “outbreak” was used as the outcome for analysis. An outbreak was defined as a cluster that met the following criteria: (1) ≥2 cases of a similar illness resulting from a common exposure (Centers for Disease Control and Prevention, 2009) and (2) the cluster was ultimately reported to CDC's National Outbreak Reporting System (NORS). For FBDOs, CDC criteria were used for confirmation of a food vehicle and setting.
Analyses were performed using SAS 9.3®. Means were compared using Student's t-test with 95% confidence intervals. Trends were analyzed using Chi-square and Fisher's exact tests for small numbers.
Results
During the 3-year study period, 948 PFGE clusters were identified; 849 (90%) were Salmonella and 99 (10%) were E. coli O157. Of those, 192 (20%) were ultimately defined as outbreaks (154 [18%] of Salmonella and 38 [38%] of E. coli O157 clusters).
Among all identified PFGE clusters, the mean time from date of collection of the first isolate to receipt by the state laboratory was 8 days (median = 6) for Salmonella and 4 days (median = 4) for E. coli O157. Mean time from receipt of isolates at the public health laboratory to reporting of PFGE results to health department epidemiologists was 20 and 15 days (medians = 14 and 7, respectively), and the mean time between collection of the first and second specimens in a cluster was 15 and 9 days (medians = 10 and 4), respectively. Mean time from reporting of PFGE results of the second isolate to initiation of an epidemiologic investigation was 7 days for Salmonella and 5 for E. coli O157 (median 1 day for both pathogens).
Times between receipt of isolates and subsequent steps for outbreaks compared to nonoutbreaks are shown in Table 1, along with the extent and proportion of clusters investigated epidemiologically. For Salmonella clusters, compared to those not determined to be outbreaks, those that were outbreaks were significantly more likely to have the first and second isolates submitted faster (p < 0.0001) and have PFGE results reported faster to epidemiologists (p < 0.0001). For E. coli O157 clusters, those determined to be outbreaks had initial PFGE results reported sooner than nonoutbreaks (p = 0.036). Intervals between collection of first and second isolates did not differ significantly between outbreaks and nonoutbreaks, for either pathogen.
Time calculated from date epidemiologist was notified of PFGE results of second isolate.
“Outbreak,” PFGE clusters ultimately reported to CDC as confirmed outbreaks; N/A, not applicable or not available; Statistically significant difference between outbreaks and nonoutbreaks, * p < 0.0001; ** p = 0.032; †p = 0.036.
IQR, interquartile range; PFGE, pulsed-field gel electrophoresis; SPHL, State Public Health Laboratory.
The most commonly reported reasons for pursuing additional epidemiologic investigation of clusters are shown in Table 2. The most commonly cited reasons for not more aggressively investigating included too few cases and difficulty contacting patients.
CDC, Centers for Disease Control and Prevention.
Salmonella and E. coli O157 clusters were significantly more likely to be identified as outbreaks as the number of cases in the PFGE cluster increased (Fig. 1) (p < 0.001 for both). E. coli O157 clusters of ≥6 cases were 2.8 times more likely to indicate an outbreak compared with smaller clusters (and 3.8 times more likely in the case of Salmonella). Among Salmonella outbreaks, 118 (77%) were reported as foodborne, 6 (4%) were reptile associated, and 14 (9%) were associated with other animal contact (for E. coli O157, 25 [66%], 0, and 2 [5%], respectively). Among Salmonella foodborne outbreaks, 32 [27%] had a confirmed location of exposure, and 51 [43%] had a confirmed vehicle of transmission (5 [20%] and 17 [68%], respectively, for E. coli O157).
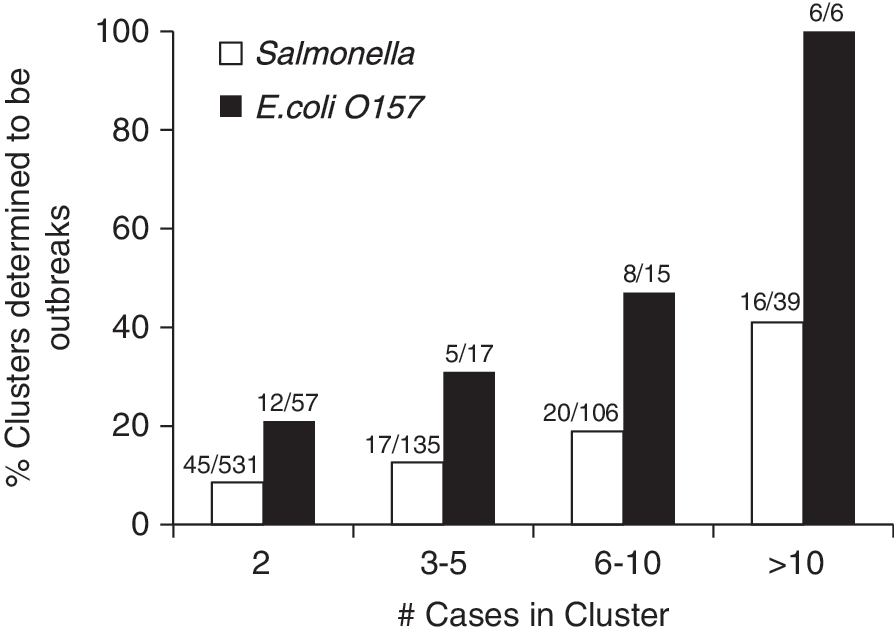
Proportion of PFGE clusters of Salmonella and Escherichia coli O157 ultimately determined to meet the CDC case definition of an outbreak. Bar labels show numbers of outbreaks/total clusters. Trends are significant for both pathogens, p < 0.001.
Discussion
Molecular subtyping of pathogens using PFGE is a critical tool for the recognition and investigation of FBDOs, and substantial public health resources are devoted to such activities. Of clusters initially identified by PFGE, 80% ultimately ended up not being confirmed as outbreaks (i.e., attributed to a common source). There remain substantial challenges and opportunities to improve the efficiency and effectiveness of outbreak response.
In this study, many days passed between initial collection of patient specimens, testing in the laboratory, and receipt of results by epidemiologists, which are consistent with the findings of others (Hedberg et al., 2008). More rapid delivery of specimens to the laboratory and faster testing and reporting of PFGE results to investigators were associated with more successful outbreak investigations. While many delays may be due to unavoidable technological limitations, there are likely additional factors that would be amenable to improvement with a detailed analysis of the barriers involved at each step. In general, compared to Salmonella, E. coli O157 isolates were submitted and subtyped faster, and epidemiologic investigations were initiated sooner. This is not surprising given their relatively lower incidence, and the fact that the rates of morbidity and mortality are higher for E. coli O157, particularly among children.
There are no well-defined, quantifiable thresholds which investigators can use to reliably determine whether a disease cluster is “worthwhile” investigating in more depth. The linear increase in the likelihood of a cluster being identified as an outbreak depending on cluster size is important. Because additional cases are often identified during the process of an investigation, it is not possible to determine precisely at what point aggressive measures should begin. Similarly, indicators such as being reported by a healthcare provider or the public, or being alerted to the cluster by CDC can increase suspicion of an outbreak independent of recognition of a PFGE cluster.
Defining a cluster of illnesses as an “outbreak” can be complex. Some level of epidemiologic investigation is always required to meet the CDC definition of an outbreak, for example, to rule out the potential for multiple shared risk factors among cases (e.g., in family members) and to identify a likely common source (e.g., a specific food, restaurant, food handler, or exposure site). Because outbreaks reported to CDC are screened for these criteria, inclusion in CDC databases was used as a proxy for being a confirmed outbreak.
While we attempted to carefully define specific activities associated with an outbreak response, determining when an investigation “starts” or “ends” can be difficult. Because all cases of Salmonella and E. coli O157 are interviewed routinely by health departments as soon as they are reported, this initial basic interview is frequently performed before PFGE results are available or before the case is recognized to be part of a PFGE cluster. If a cluster is determined to warrant further investigation by epidemiologists, subsequent activities may include administering additional hypothesis-generating questionnaires, queries to the CDC PulseNet database (to determine if there are isolates from other states that match a cluster identified locally), communication with other states or CDC, initiation of an analytic study (e.g., case–control or cohort study), performance of an environmental investigation at a suspected site of contamination, and widespread notification of other agencies of a possible outbreak. These investigative steps may occur in any order or concurrently, and most clusters are not investigated using all of these steps.
Currently, PFGE is the primary method of molecular subtyping available to public health laboratories nationwide. The field of molecular microbiology is changing rapidly, however, with the increasing availability of other molecular tests and nonculture diagnostic methods (Jones et al., 2012). This study demonstrates the importance of molecular subtyping data to outbreak investigations and highlights the need both for continued public health laboratory access to pathogen isolates and the need for public health to develop the capacity for capturing data that is at least as useful as the present system, in light of new commercially available tests. Whole genome sequencing (WGS) shows great potential for further refining PFGE clusters, by identifying isolates that appear related by PFGE, but are not by WGS. With the increasing availability of this technology, much more precise distinction between isolates will be possible, with the hope that correlation of laboratory and epidemiologic data will improve outbreak detection and response. This study provides data which may be used to evaluate the relative costs and benefits of implementing WGS in public health laboratories.
In addition, our results serve as a reminder that while molecular subtyping and laboratory data are vitally important, basic epidemiologic capacity remains critical for the investigation of outbreaks. This capacity is necessary at the local, state, and federal levels. While national initiatives such as PulseNet have markedly improved outbreak response, the overwhelming majority of FBDOs are still detected and investigated at the state and local level (Murphree et al., 2012). In the face of continued declines in public health funding, balancing these important needs will become increasingly challenging.
Footnotes
Acknowledgments
The authors thank Alvina Chu, Maryland Department of Health and Mental Hygiene, and members of the FoodNet Outbreak Working Group for their assistance with this study. This work was supported by the Centers for Disease Control and Prevention, Emerging Infections Program Cooperative Agreement in participating states.
Disclosure Statement
No competing financial interests exist.