
Abstract
Objective:
To assess food safety practices, food shopping preferences, and eating behaviors of people diagnosed with Salmonella or Campylobacter infection in the warm seasons, and to identify socioeconomic factors associated with behavior and practices.
Methods:
A cross-sectional survey was conducted among Salmonella and Campylobacter cases with onset of illness from January 1 to March 31, 2013. Multivariable logistic regression analyses examined relationships between socioeconomic position and food safety knowledge and practices, shopping and food preferences, and preferences, perceptions, and knowledge about food safety information on warm days.
Results:
Respondents in our study engaged in unsafe personal and food hygiene practices. They also carried out unsafe food preparation practices, and had poor knowledge of foods associated with an increased risk of foodborne illness. Socioeconomic position did not influence food safety practices. We found that people's reported eating behaviors and food preferences were influenced by warm weather.
Conclusions:
Our study has explored preferences and practices related to food safety in the warm season months. This is important given that warmer ambient temperatures are projected to rise, both globally and in Australia, and will have a substantial effect on the burden of infectious gastroenteritis including foodborne disease. Our results provide information about modifiable behaviors for the prevention of foodborne illness in the household in the warm weather and the need for information to be disseminated across the general population. An understanding of the knowledge and factors associated with human behavior during warmer weather is critical for public health interventions on foodborne prevention.
Introduction
I
Inadequate food preparation practices and lack of food safety knowledge of consumers may be responsible for foodborne disease from food consumed at home (Scott, 2003). Little is known about human behavior in response to warmer weather and whether changes in people's eating behaviors, food preferences, and food safety practices in the warm season increase the risk of foodborne disease. For example, human behavior such as outdoor eating in warm seasons may increase exposure to contaminated food (James and James, 2010). Likewise, changing food consumption patterns, including a preference for eating out, consuming preprepared food, and more fresh, potentially unwashed and uncooked fruit and vegetables may also contribute to an increase in foodborne illness in warm seasons (Rose et al., 2001).
South Australia (SA) has a Mediterranean climate with cool wet winters and hot dry summers, and in Adelaide the average maximum temperature during the warm seasons is 27°C (Milazzo et al., 2016). With warmer ambient temperature and heatwaves predicted to increase because of climate change, there might be an upsurge in incidence of foodborne disease adding to the burden currently associated with infectious gastroenteritis (Smith et al., 2014).
This study aimed to explore factors influencing behavior and food safety practices in the warm weather of people diagnosed with Salmonella or Campylobacter infection. We were specifically interested in understanding how demographic characteristics influenced food safety practices.
Materials and Methods
Study design
A cross-sectional survey was conducted to elicit information from Salmonella and Campylobacter cases about (1) knowledge and behaviors related to safe food handling practices;(2) behavior and preferences of shopping, eating out, and food consumption; and (3) preferences, perceptions, and knowledge about food safety information. Questions were based on findings from previous food safety studies and those on knowledge and consumption of high-risk foods were validated against reported foodborne outbreaks (Mitakakis et al., 2004; Brennan et al., 2007; Department of Human Services [DHS], 2007). In our study, we defined warm days occurring within our warmer season of January to March.
Participants and recruitment
Cases of Salmonella or Campylobacter infection in residents of SA and notified to the Communicable Disease Control Branch (CDCB), Department for Health and Ageing, with an onset of illness during the warm season of January 1 to March 31, 2013 were invited to participate in the survey. Cases (parent/guardian if a child case) were sent a letter of invitation from CDCB.
The survey tool was a structured questionnaire (Supplementary Data; Supplementary Data are available online at
Sample size
Assuming 600 cases notified across the warm season months, and a response rate of 25% we estimated 150 questionnaires would be returned. With this size sample, we could detect an odds ratio (OR) of 1.7 as statistically significant (assuming n = 150, α = 0.05, power = 0.80, exposure variable follows standard Normal distribution, and a two-sided test).
Data collection
The questionnaire consisted of 34 questions, with 13 of these demographic characteristics. The remaining 21 questions related to food safety within three broad domains; (1) 13 questions related to knowledge and behavior in safe food handling practices; (2) five questions related to behavior and preferences for shopping, eating out, and specific foods eaten on warm days, and (3) three questions concerned preferences and perceptions about receiving food safety information on warm days, and knowledge about heat as a risk factor for infectious gastroenteritis. For child cases, information specific to household-level food safety questions and food shopping practices was obtained from a proxy respondent, usually the parent/guardian.
Measures
Response categories to different items varied to reflect the range of questions used. We calculated an overall summary score for questions relating to food safety knowledge and practices, and consumption of high-risk foods. For each respondent, scores were summed to derive a total score for personal and food hygiene practices (minimum score 0, maximum score 30); safe food practices (0–25); knowledge on food safety practices (0–25); and consumption (0–16) and knowledge of high-risk foods (0–16). Higher scores were indicative of better knowledge or practice, and lower scores denoted poor knowledge and unsafe practices. We then dichotomized knowledge into poor (1) or good (0), based on the median of the distribution of the total knowledge score assigned. Similarly, we created a food safety practices dichotomous variable, with categories of safe or unsafe based on the median cutpoint. We created separate binary variables for each question that had more than one response option for shopping preferences and information receiving, and then coded these as yes/no or likely/unlikely dependent on the outcome variable.
Residential postcodes were used to derive the Index of Relative Socioeconomic Disadvantage (IRSD) (Australian Bureau of Statistics [ABS], 2006), which measures area-level of disadvantage based on economic and social conditions of people and households. We categorized each individual according to IRSD quintiles, with quintile 5 representing most disadvantaged through to quintile 1 indicating least disadvantaged.
Statistical analysis
Separate bivariate logistic regression analyses were performed to examine the association of individual items and summary dichotomy variables with household income, education level, and socioeconomic disadvantage. In the next stage of model fitting, we selected those variables with a significance level <0.25 and included them in the multivariable models to examine adjusted effects of demographic variables on outcome variables, and retained those with a significance level of 0.05. We used backward elimination in the second stage of multivariable model fitting to arrive at our final statistical model (Hosmer et al., 2013). IRSD was selected as the socioeconomic variable in the final models as the models with this variable had consistently better fit compared to models with levels of income or education. Age and gender were controlled for as possible confounding effects in all of the regression models. Responses of “don't know” and refusal to answer were excluded from the analysis of that question. Results are presented as adjusted OR with 95% confidence intervals (CI). Analyses were conducted using StataSE 13 (StataCorp LP, College Station, TX).
Ethics approval
All data analyzed were nonidentifiable with ethics approval given by the Human Research Ethics Committee of the SA Department for Health and Ageing (HREC/12/SAH/93).
Results
Characteristics of study participants
Of the 607 questionnaires sent to cases, 183 completed the survey and of these, 44 (24%) were telephoned post initial mail-out. Response proportions were higher for Campylobacter (60%) than Salmonella (40%) cases. Table 1 shows the demographic characteristics of participants. Just over half (52%) were aged between 20 and 59 years, and 58% were female. The highest education level was certificate or higher (45%), and 47% reported an annual income level of >$60,000. There was an even distribution of the study population in four of the five IRSD quintiles (21–23%). Demographic differences were observed between respondents. Salmonella cases were younger, with a greater percentage in the most disadvantaged group, and there was a lower percentage with higher education and income levels than Campylobacter cases. The majority of those who completed the questionnaire (including parents of children) were also the main person responsible for food preparation and shopping in their household.
Food safety practices
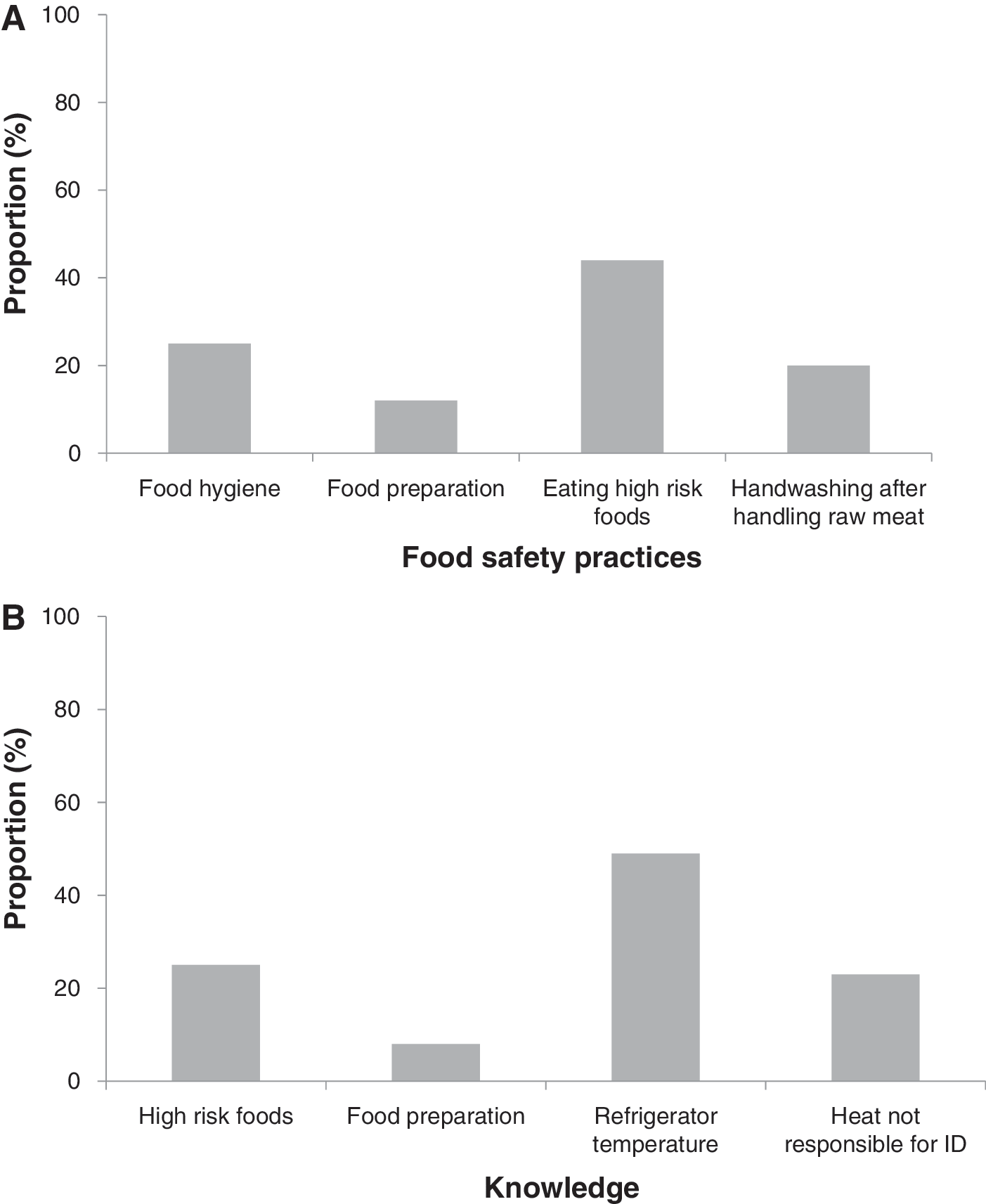
In the multivariable models IRSD was not significantly associated with unsafe food and personal hygiene practices. Figure 1A shows that 25% reported unsafe personal and food hygiene practices. Contrary to this, 80% reported that they always washed their hands after using the toilet, and 52% always washed their hands before handling food. Overall, 12% carried out unsafe food practices. Twenty percent did not wash their hands appropriately after handling raw meat, with 17% rinsing their hands and 3% wiping their hands. Separate cutting boards for raw meat only was used by 70%, and 80% always washed cutting boards before use for food, and after preparation of raw meat. Detergent (78%) was commonly used for washing cutting boards after preparing raw meat. Those who did not wash cutting boards properly used vinegar (3%) and plain water (3%).
IRSD was not a significant predictor of unsafe practices for food storage, and defrosting frozen meat at room temperature on warm days. Compared to the least disadvantaged group, those in the second to highest quintile were less likely to carry fresh food in a portable insulated container on a warm day (IRSD quintile 2, OR 0.11, 95% CI 0.02–0.52). On warm days, 88% of respondents were more likely to go directly home after food shopping, and 93% took less than 15 min to unpack raw meat and fresh food and place in storage. Preferences for defrosting frozen raw meat on warm days included refrigerator (57%), microwave (13%), and room temperature (28%) while 1% of respondents preferred water and cooking frozen meat, respectively. Of those defrosting frozen raw meat at room temperature on warm days, 43% took less than 2 h, and 28% took 4 or more hours. Most of the respondents (76%) were likely to carry food in insulated shopping bags.
Food and shopping preferences
Respondents aged over 60 years were less likely to eat out at festival events (OR 0.25, 95% CI 0.07–0.84) or have a barbeque on warm days (OR 0.14, 95% CI 0.05–0.42) compared to those aged 40 to 59 years. Overall, parties (45%), cafes (35%), and takeaway (30%) were preferred food outlets and events for eating out on warm days. Just over half (54%) of the households were likely to have a barbeque on a warm day.
Compared to the least disadvantaged group, those most disadvantaged were more likely to eat chicken (OR 4.12, 95% CI 1.49–11.33) and vegetables (OR 3.59, 95% CI 1.24–10.34). Those aged 60+ years were more likely to eat eggs (OR 6.44, 95% CI 1.87–22.19) compared to those aged 0–9 years. Overall, 44% of participants consumed high-risk foods on a warm day, including fruit (72%), ice-cream (64%), vegetables (59%), chicken (52%), fish (49%), and eggs (40%).
There was no clear preference for shopping closer to home on a warm day, and 59% were likely to shop at a supermarket rather than in specific locations such as the butcher or fruit and vegetable shop. The exception was those in the most disadvantaged group who were less likely to shop in a supermarket (OR 0.07, 95% CI 0.00–0.61) compared to those in the least disadvantaged quintile.
Knowledge
IRSD was not a significant predictor for knowledge about risky foods or that warm weather could be responsible for infectious diseases. Figure 1B shows that overall 25% of respondents had poor knowledge about high-risk foods for foodborne infection. Foods considered high-risk by respondents were undercooked chicken (92%), raw chicken (90%), raw meat (75%), undercooked meat (70%), fish (55%), raw eggs (41%), dairy (34%), and prepacked salads (27%). The correct refrigerator temperature setting was not known by 49% of respondents, although women were twice as likely as men to know the correct setting (OR 2.26, 95% CI 1.09–4.71). As shown in Figure 1B, knowledge of food hygiene practices deemed unsafe was good (92%), and 67% perceived that heat was responsible for infectious diseases causing diarrhea.
Information about food safety
Those aged 60+ years were less likely to feel that they received adequate information (OR 0.28, 95% CI 0.11–0.74) compared to those aged 40–59 years. Overall, 60% felt that they had received adequate information.
Table 2 highlights preferred methods for receiving food safety information on warm days. Women were significantly more likely than men to prefer television for receiving information (OR 2.36, 95% CI 1.15–4.87). Compared to the least disadvantaged group, those most disadvantaged were less likely to prefer the internet (OR 0.27, 95% CI 0.07–0.92) and printed material (OR 0.32, 95% CI 0.10–0.98). Women were less likely than men to prefer information received from the health department (OR 0.34, 95% CI 0.13–0.84) and schools (OR 0.10, 95% CI 0.02–0.41). There were no significant differences for receiving information via the radio or pamphlets according to gender, age group, or IRSD.
Age: In the analysis, age was restricted to include the 20–39, 40–59, and 60+ year age groups.
CI, confidence interval; OR, odds ratio.
Discussion
This study highlighted gaps in food safety knowledge and practices in domestic households. Our findings are in line with other Australian (Mitakakis et al., 2004; DHS, 2007; Worsley et al., 2013) and international studies of the general population (Gilbert et al., 2007; Nesbitt et al., 2009; Langiano et al., 2012). Despite the fact that our respondents were Salmonella or Campylobacter cases, our findings are in keeping with those reported from community surveys. Poor practices in food preparation and hygiene suggest that, in general, consumers do not take necessary measures to safeguard against the transfer of pathogens during food preparation potentially increasing the likelihood of cross-contamination in the domestic kitchen leading to foodborne illness (Scott and Herbold, 2010).
Generally, food safety practices in warm weather were not linked to risky behavior. On a warm day respondents were likely to go home after food shopping and take little time to unpack cold food and place in storage. These are consistent with a New Zealand study, although that study did not relate practices according to ambient temperature. In relation to safe practices, our respondents were likely to carry their food in an insulated bag, compared to New Zealand where only a small proportion did (Gilbert et al., 2007). In our study risky behavior in the warmer weather was linked to defrosting frozen meat at room temperature for more than 4 h. This practice has been more commonly reported in other countries (Brennan et al., 2007; Nesbitt et al., 2009; Langiano et al., 2012) and is believed to contribute to foodborne illness since multiplication of microorganisms in food is directly influenced by ambient temperature. For example, Salmonella growth occurs within an ideal temperature range of 35–43°C and Campylobacter within 30–45°C (Craig and Batholomaeus, 2011). Therefore, it is necessary to recommend actions for awareness at a community level to improve people's knowledge on safe practice in households, especially in the warmer weather.
It has been postulated that with increasingly warmer weather, consumers may change their shopping behavior and purchase all their food needs at the one supermarket, or increase their preference for takeaway and home delivery of fast foods (Banwell et al., 2012). In our study there was no preference for shopping closer to home on warm days, although the most disadvantaged group were less likely to shop in a supermarket, which may reflect other options (Banwell et al., 2012), such as from fast food takeaway outlets.
Almost half of respondents preferred eating foods in the warmer weather that could be potential sources of foodborne pathogens into the home (Scott, 2003). Food is an important route of transmission for Salmonella infection and implicated foods most commonly associated with outbreaks have been poultry, eggs, raw meat, milk, dairy products, fresh produce, and fruit juice (Berger et al., 2010; Craig and Batholomaeus, 2011). In Australia, chicken consumption is identified as the main risk factor for Campylobacter infection (Stafford et al., 2008).
Knowledge on correct refrigerator temperature in our study was poor. Previous reports suggested the proportion with poor knowledge ranged from 29% (Macías-Rodríguez et al., 2013) to 60% (Nesbitt et al., 2009) having good knowledge of correct temperature setting (Brennan et al., 2007; Vegara et al., 2014). Incorrect (high) refrigeration temperature increases the opportunity for pathogenic microorganisms to grow in contaminated food (Vegara et al., 2014). There is scope and a need to improve consumers' knowledge about temperature setting of refrigerators, which may become even more relevant with predicted rises in ambient temperature in the future.
More attention needs to be paid to community health education for older people, as those in our study felt that they did not receive sufficient information about food safety on warm days. Warmer temperature was not thought to be a risk factor for infectious gastrointestinal illness among our respondents, suggesting the need for tailored public health messages. To understand how this may translate into recommendations for promoting awareness, it is ideal to identify preferences of community members so that relevant actions can be taken accordingly. In this study we found that preferences for information receiving varied. Although not related to receiving information about food safety on warm days, preferred mediums for information receiving identified in other food safety surveys were not dissimilar to our findings. These included a preference for mass media and print brochures (Langiano et al., 2012), and electronic media to inform consumers of high-risk food items (Nesbitt et al., 2009).
Demographic factors may predict food safety behavior as highlighted in our study. We found the most disadvantaged respondents consumed more high-risk foods, while the 60+ group were more likely to eat eggs than younger respondents. Preferences for information receipt varied in our study between IRSD quintiles, gender, and age. In contrast to our findings, other studies reported that socioeconomic status shapes behaviors of respondents related to household food preparation (Brennan et al., 2007; Nesbitt et al., 2009; Langiano et al., 2012). All these factors should be accounted for when designing relevant community intervention strategies.
Our study has several limitations. The response rate was 30%, which is similar to other food safety surveys (Gilbert et al., 2007; Nesbitt et al., 2009). Responses to survey questions were based on self-reported behavior, which is subject to possible reporting bias. Self-reported behaviors may not correlate with observed behavior (Redmond and Griffith, 2003; Wills et al., 2015). There were discrepancies between participants reported food preparation behavior and knowledge of food safety. Despite the fact that our study population was Salmonella or Campylobacter cases, other studies found no differences in behavior and knowledge between Salmonella cases and controls, adding more evidence to the applicability of our results to the wider population (Kohl et al., 2002; Parry et al., 2002). Recall bias is another possible limitation of our study. Some respondents would have answered on days of extreme heat, whereas other respondents would have completed the survey on less extreme heat days.
Conclusion
Many people do not practice safe food handling and preparation in the household. When poor food practice collides with higher ambient temperatures, the potential for a synergistic increase in risk of foodborne illness during warm seasons is alarming. The need for targeted initiatives in warmer weather is even more important, since the role of temperature and foodborne disease incidence is well established. These findings will assist policy makers and public health practitioners to develop practice guidelines for community level education and awareness.
Footnotes
Acknowledgment
The authors thank staff from the Disease Surveillance and Investigation Section, Communicable Disease Control Branch, Department for Health and Ageing (SA Health) for their support in conducting this study.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.