
Abstract
Objectives:
The objectives were to describe the incidence, demographics, laboratory findings, and suspected sources of childhood Salmonella infections in Alberta, Canada, with a focus on preventable cases.
Methods:
Data from Notifiable Disease Reports for children with nontyphoidal salmonellosis (NTS) or typhoid/paratyphoid fever from 2007 through 2015 were analyzed.
Results:
NTS was detected from 2285 children. Bacteremia was documented in 55 cases (2.4%), whereas a single infant had NTS meningitis. The suspected source was food (N = 577; 25.3%) followed by animal or animal manure contact (N = 426; 18.6%), of which a reptile was the suspected source in 264 cases (11.5%). There were 44 outbreaks with none sharing the same food source. Ninety-five children were diagnosed with typhoid/paratyphoid fever, of which 48 cases (51%) were typhoid cases in unimmunized children 2 years or older.
Conclusions:
There are still ∼275 pediatric cases of Salmonella infection in Alberta annually, the bulk of which are preventable.
Application:
Public education about reptile exposure, food safety, and pretravel immunizations could potentially prevent many cases of Salmonella infection.
Introduction
T
Salmonella cause two distinct diseases: nontyphoidal salmonellosis (NTS) and typhoid/paratyphoid fever. NTS is usually acquired from food products contaminated by animals that carry NTS or directly from infected pets, although person-to-person spread can occur. Disease typically presents as self-limiting gastroenteritis although invasive infection can occur. S. enterica serotypes Typhi and Paratyphi cause typhoid/paratyphoid fever, which manifests initially as bacteremia and fever. Transmission is through water or food contaminated by human feces, with the exception of some Paratyphi C, which have animal hosts (Harris and Ryan, 2015).
The epidemiology of NTS infections seems to have changed in recent decades (Linam and Gerber, 2007) with mass production and distribution of food, increased popularity of reptiles as household pets, and increased use of raw meat diets for household pets. The epidemiology of typhoid/paratyphoid fever has also evolved with increasing international travel. Recent data on risk factors for pediatric Salmonella infection primarily come from low- and middle-income countries (Uche et al., 2017). The purpose of this study was to analyze recently reported cases of Salmonella infection in children in Alberta (a Canadian province with primarily a semiarid cold climate) to determine the incidence and source of infection to inform policy change for prevention of disease.
Materials and Methods
After ethics approval from the Health Research Ethics Board of the University of Alberta, data were obtained on all Salmonella cases reported in Alberta in children <18 years of age from 2007 through 2015. The Alberta population was 3,645,257 in 2011 (Statistics Canada, 2011), of which ∼800,000 were <18 years of age (Government of Alberta, 2016). Laboratories are mandated by law in Alberta to report all Salmonella cases. Detection was through culture rather than molecular techniques during the years of the study. However, all laboratories that perform isolation of Salmonella forward the isolates to the Alberta Provincial Laboratory for Public Health for further identification, including serotyping and pulsed-field gel electrophoresis (PFGE).
Surveillance data are collected under the Public Health Act in Alberta, and public health follow-up is conducted by a provincial public health team that is coordinated by a single health authority. Data are entered into a centralized electronic communicable disease and outbreak management system. Data routinely collected on the Notifiable Diseases Report (NDR) form for every laboratory-diagnosed or epidemiologically linked infection include age, sex, date of symptom onset and of diagnosis, hospitalization status, type of specimen from which Salmonella was isolated, serotype cause of death when applicable, and history of recent travel or immigration. In addition, for NTS cases, the suspected source of infection and the location where the infection was acquired were reported. This information was based on the results of an interview with the patient or parent by a public health nurse or inspector.
For cases with no history of travel or association with an outbreak or other cases of Salmonella infection, attribution of source can be difficult. For Sporadic cases a comprehensive set of questions are asked to identify high-risk activities and foods. Based on the predicted level of risk for each exposure, the most likely source is determined. Ongoing training of public health staff is provided to promote consistency between investigators. Cases in which more than one animal type was suspected were not attributed to any specific type of animal in data analysis. For typhoid/paratyphoid fever cases, additional data included the typhoid immunization status.
For each case, a single specimen type is recorded on the NDR in a hierarchical manner in the descending order of cerebrospinal fluid (CSF), blood, urine, or sputum, then stool, such that if a specimen type higher on the hierarchy cultures Salmonella, only that specimen type is recorded regardless of the coexistence of a positive specimen lower on the hierarchy.
NTS was attributed to recent immigration or travel if the onset occurred within 18 days of entry or return to Alberta (Seals et al., 1983). Typhoid/paratyphoid fever was attributed to recent immigration or travel when the onset occurred within 60 days (American Academy of Pediatrics, 2015) of entry or return to Alberta from a resource-poor country.
The single Public Health Laboratory in Alberta has a dedicated enteric team that typically identifies potential outbreaks first. An outbreak was defined as more cases of a particular PFGE pattern or serotype observed than expected in a particular time and location. In general, the instigation for an outbreak investigation was recognition of two or more cases in a short period of time living in the same geographic area but not the same household. Standard outbreak investigation processes were followed to identify and confirm the source. Data collected for this study included the number of pediatric and adult cases and the source. The source was considered to be confirmed if verified by molecular typing of Salmonella from the case and from the source and suspected if the presumed source was based on epidemiological data.
Data analysis
Incidence was calculated based on the average number of children per year in Alberta in the respective age group, using population data from Statistics Canada (2016). Comparative statistics were calculated using chi-square test or Fisher exact test as appropriate. Data analysis was performed using SAS 9.3 (SAS Institute, Inc., Cary, NC, 2011).
Results
Nontyphoidal salmonellosis
Demographics
Over the study period, there were 2285 NTS cases (249 inpatients and 2036 outpatients; 1228 males and 1057 females) (Table 1; Fig. 1) ranging from 10 days to 17 years of age (mean 5.96 ± 5.27 years; median 4 years). Inpatients comprised 10.9% and had a mean age of 5.30 ± 5.42 years (range 10 days to 17 years; median 3 years). Younger age was associated with a higher incidence of infection and hospitalization (19.8% of children <5 years of age were hospitalized vs. 8.6% of older children; p < 0.0000001) (Table 1). Infants <1 year old with NTS were 2.68 times more likely to be hospitalized than were the next most likely age group (1 year old).
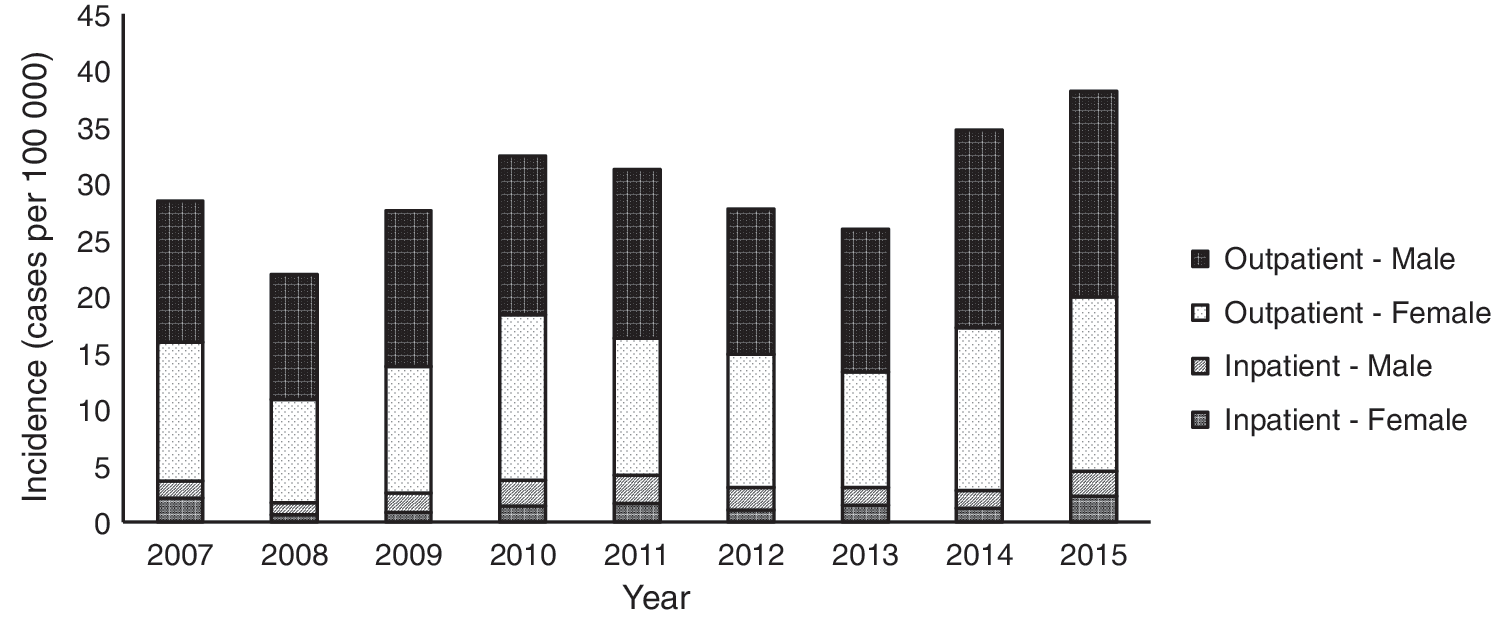
The incidence of childhood NTS in Alberta, by gender and hospitalization status. NTS, nontyphoidal salmonellosis.
NTS, nontyphoidal salmonellosis.
Laboratory findings
Of the 2285 NTS cases, 2192 (96%) were laboratory confirmed, of which 114 cases were linked to an outbreak. The other 93 cases were not laboratory confirmed with 61 linked to household cases and 32 linked to an outbreak (Table 2). Common serotypes were Enteritidis (37.5%), Typhimurium (14.8%), and Heidelberg (8.8%) (Table 2). Hospital admission was less common for Enteritidis cases (9.1%) versus all other serotypes (14.4%; p = 0.0068; Fisher exact) (Table 2). Salmonella Heidelberg was isolated from the CSF of an infant <1 year old who died from the infection.
Includes serotypes that caused <1% of cases.
For laboratory-confirmed cases, NTS was detected in CSF (N = 1; 0.05%), blood (N = 55; 2.5%), urine (N = 54; 2.5%) sputum (N = 2; 0.09%), and stool (N = 2070; 94.4%).
Sources
The most common suspected source was food (N = 577; 25.3%) followed by animal or animal manure contact (N = 426; 18.6%), recent travel to a resource-poor country (N = 431; 18.9%), person-to-person transmission (N = 190; 8.3%), domestic travel (N = 40. 1.8%), recreational water (N = 10; 0.4%), raw pet treats (N = 3; 0.1%), unknown (N = 597; 26.1%), and other (N = 8; 0.4%).
A reptile was the suspected source in 264 cases (11.5%, including 10.6% of outpatient cases and 19.3% of inpatient cases) with the encounter occurring in the child's home (N = 248), in another home (N = 9), in a pet store (N = 3), at a petting zoo/livestock event (N = 2), while camping (N = 1), and at school (N = 1). For infants <1 year old with NTS (N = 334), 84 cases (25.1%) were linked to reptiles with the next highest age group being 11 to 17 year olds (N = 530), in which 64 cases (12.1%) were linked to reptiles. Reptile-associated cases were more likely to result in hospitalization than were other exposures (relative risk = 1.86; 95% confidence interval 1.39–2.49; p = 0.0002). Eight cases were linked to cats or kittens (six pet cats, one kitten contaminated with sewage, and one cat rescue shelter) and seven to hedgehogs.
The most common locations where NTS was suspected to have been acquired was a private dwelling (N = 941; 41.4%), followed by recent international travel/immigration (N = 431; 18.9%), an animal facility (N = 91; 4%), a permitted food establishment (N = 68; 3%), domestic travel (N = 40; 1.8%), a school or childcare facility (N = 25 (1.1%), unknown (N = 657; 27.8%), and other (N = 50; 2.2%).
Outbreaks
One hundred forty-six childhood NTS cases were linked to 44 outbreaks. Each outbreak included a mean of 3.30 ± 3.53, median of 2, and range of 1 to 21 pediatric cases. For the outbreaks with full data (N = 27), there were a mean of 14.00 ± 14.42, median of 8, and range of 2 to 51 linked adult cases. Outbreaks were confirmed or suspected to be related to food (N = 16; 1 outbreak each from cantaloupe, chia seed powder, sprouts, frying batter, and improperly handled/packaged poultry products with the exact food not known in 11 outbreaks), food handlers (N = 1), recent international travel (N = 8; travel to Cuba and Mexico in 4 outbreaks each), animals (N = 6; 2 pet bearded dragons, 1 feeder mice, 1 live baby poultry; 2 unknown), recent domestic travel to Saskatchewan (N = 1), pet treats (N = 1), or an unknown source (N = 11). The main serotypes causing outbreaks were Enteritidis (N = 15), Typhimurium (N = 9), Heidelberg (N = 4), Agona (N = 2), Infantis (N = 2), Javiana (N = 2), and Reading (N = 2). Serotypes Cotham, Cubana, Hartford, Litchfield, Newport, Schwarzengrund, ssp enterica (1) 4,5,12:D:-, and ssp enterica (I) 4,5,12:I:- caused one outbreak each.
Typhoid/paratyphoid fever
There were 95 cases (73 Salmonella Typhi and 22 Salmonella Paratyphi; 50 males and 45 females) aged 5 months to 17 years (mean 7.62 ± 5.06 years; median 7 years) (Table 1). Detection was from blood in 73 cases (78%) and from stool alone in 21 cases (22%). Hospitalization was required for 61 cases (64%).
Most patients with typhoid/paratyphoid fever recently immigrated or traveled to a resource-poor country without a predeparture typhoid vaccine (N = 78; 82.1%) (Table 3). Sixty-eight of these 78 children were 2 years or older; 48 had typhoid and 20 had paratyphoid fever. Therefore, 48 of the 95 typhoid/paratyphoid cases (51%) were potentially vaccine preventable, recognizing that typhoid vaccines do not have 100% efficacy. All had visited/emigrated from Asia with the exception of one case from Nigeria. Five other children (5.3%) acquired typhoid fever in Asia despite adequate immunization (maximum 385 days before travel) (Table 3). Twelve patients (12.6%) had no history of recent travel to a resource-poor country but eight of them reported a symptomatic close contact with such travel. There were no typhoid/paratyphoid outbreaks recognized.
One child was vaccinated 4 years before traveling internationally and was, therefore, included in the recent immigration or international travel, unvaccinated group.
Discussion
There are a mean of ∼250 NTS cases and 10 typhoid/paratyphoid fever cases diagnosed annually in children in Alberta. More than half of cases occurred in children <5 years of age with an average incidence of 52.8 per 100,000 (51.4 per 100,000 for NTS alone). Similarly, a 1996–2012 study from 10 sites in the United States reported 63.5 Salmonella infections per 100,000 children <5 years of age versus 16.4 per 100,000 in the entire population (CDC, 2013a). A 1990–2004 study from Waterloo, Canada, reported that the number of NTS cases per 100,000 children <5 years of age was more than double that for any other age group (p < 0.001) (Keegan et al., 2009). There may be a bias toward increased stool testing in young children (Franklin et al., 2015). Nonetheless, in the current study, the incidence of NTS hospitalization was highest among infants <1 year old, suggesting a true increased risk of disease. A 1997–2007 study from London, Ontario, Canada, verified this higher admission rate in infants and showed that almost all children <12 weeks of age with Salmonella infection (83%) required hospitalization (Cellucci et al., 2010) (vs. only 26 of 58 [45%] in this study). Neonates maintain mild gastric acidity and an increased gastric emptying rate, both of which increase their susceptibility to intestinal infections (Bula-Rudas et al., 2015).
Serotypes Enteritidis (36.0%), Typhimurium (14.2%), and Heidelberg (8.4%) comprised 59% of all Salmonella cases. These were also the top serotypes in two previous Canadian studies (Cellucci et al., 2010; Public Health Agency of Canada, 2013). Variable geographic distributions may reflect interprovincial environmental or animal husbandry differences (The Center for Food Security and Public Health, 2016; Hoelzer et al., 2011).
A statistically significantly smaller percentage of cases of serotype Enteritidis required hospitalization than did other serotypes. Similarly a large FoodNet study found that there was a trend toward a lower hospitalization rate for serotype Enteritidis than for serotypes Typhimurium or Heidelberg (CDC, 2008). This may stem from variable pathogenicity across serotypes (Jones et al., 2008; Bula-Rudas et al., 2015) but needs to be interpreted with caution, as it could be because of a different patient age distribution of Enteritidis versus other serotypes.
The reason for the high incidence of reptile-associated NTS infections in children is unclear (Asmar & Abdel-Haqi 2015). It is possible that compared with adults, children have more direct contact with reptiles, but their risk may also stem from consumption of food prepared and contaminated by adults with reptile contact. There is a high incidence of invasive disease in reptile-associated cases (15% in one study with those with invasive disease being significantly younger) (Meyer Sauteur et al., 2013). Reptile exposure was associated with about 20% of hospitalized NTS cases in this study, whereas 33% of reptile-associated cases in infants <1 year old resulted in hospitalization (vs. 15% of nonreptile-associated cases; p > 0.05). Previous research confirms that having reptiles in the home is a risk factor for NTS in infants <1 year old; these infections are likely transmitted indirectly because infants infrequently touch reptiles (CDC, 1995; Mermin et al., 1997). Breastfeeding may be protective against NTS in general (Rowe et al., 2004) and reptile-associated NTS in particular (Mermin et al., 1997).
A case–control study demonstrated that NTS infections in children were significantly associated with recent contact with cats (Younus et al., 2010). In the current study, eight patients with NTS had cats as the suspected source. Seven serotype Typhimurium cases were linked to pet hedgehogs. In recent years, hedgehogs have been associated with Typhimurium outbreaks and a growing number of cases in the United States (CDC, 2013b).
A recent study from Australia confirmed our finding that a risk factor for NTS infection is young age. They also described a link with the use of powdered formula, pet ownership, and recent antibiotic use (Williams et al., 2016). Environmental sampling from collection of visible animal feces, vacuum dust, pond water, or sandpit sand in or near the home detected NTS in 41 of 56 (73%) cases and 18 of 29 (62%) controls (odds ratio: 1.67; 95% confidence interval: 0.57–4.79; p = 0.29) with the environmental sample not matching the clinical sample in 23 of 41 cases (56%). Clearly it is very common for young children to be exposed to NTS and further work is required to determine risk factors for symptomatic infection.
Food (N = 16; 36%) or animals (N = 6; 14%) were commonly linked to NTS outbreaks, which is consistent with data from U.S. outbreaks in 1998 through 2008 (Bula-Rudas et al., 2015). Chia seed powder was first identified as a source of Salmonella during a 2014 international outbreak (Tamber et al., 2016).
International travel accounted for 19% of NTS cases (and 24% of Salmonella Enteritidis cases) with most children visiting Mexico and the Caribbean. Previous studies estimated that of Salmonella Enteritidis cases, travel was related to 52% (Ontario data) (Tighe et al., 2012) or 36% (Canada-wide data) (Nesbitt et al., 2012), and that Caribbean (Nesbitt et al., 2012; Tighe et al., 2012) and Mexico (Tighe et al., 2012) were the most visited areas.
In an international collaborative project that collects data on ill travelers, <40% from resource-rich countries had predeparture contact with a travel clinic (Boggild et al., 2010). There is no vaccine for paratyphoid fever, or a typhoid vaccine licensed for children <2 years old. Ten (14%) of the typhoid cases occurred in children too young to be vaccinated. However, about half of the typhoid cases occurred in children who were 2 years or older but recently immigrated from or traveled to a high-risk country without typhoid vaccine. India, Pakistan, and Bangladesh were the most frequent source countries. Five patients who recently entered Alberta from India or Pakistan acquired typhoid fever within 385 days posttyphoid vaccination. These infections are possibly attributable to the 1- and 2-year efficacies of 69% and 59% for the Typhim Vi vaccine, and 35% and 58% for the Ty21a vaccine (Anwar et al., 2014).
From 1999 to 2006, 21% of typhoid fever cases in the United States were domestically acquired; 22% of these were linked to outbreaks, whereas ∼17% were linked to disease carriers (Bula-Rudas et al., 2015). Comparatively, in this study, 13% of typhoid/paratyphoid cases (13%) were domestically acquired, of which 67% reported close contact with a recent traveler, leaving only 4% with no presumed source.
A limitation of Salmonella epidemiological studies is that the source of infection is often suspected rather than proven. The NDR allows for either a suspected source or a recent travel history for each patient, but not both, so we did not know the suspected source type in children who reportedly acquired Salmonella outside Alberta.
In conclusion, a large number of potentially preventable cases of Salmonella infection continue to occur in children in Alberta. The risk from exposure to reptiles needs to be further publicized (Alberta Health 2015; Alberta Veterinary Medical Association 2017), perhaps through social media with an emphasis on the higher risk of severe disease in infants. Outbreaks of NTS were each attributed to a different food source, but perhaps part of the solution lies in including information on food safety in the school curriculum. The vast majority of cases of typhoid/paratyphoid fever occurred in unimmunized travelers to Asia. It needs to be established whether the common barriers to pretravel immunization can be overcome.
Application
This study demonstrates that even in an affluent country, public education about reptile exposure, food safety, and pretravel immunizations could potentially significantly decrease the incidence of Salmonella infections.
Footnotes
Acknowledgments
The authors thank Alberta Health Services and the Alberta Provincial Laboratory for Public Health for data collection.
Disclosure Statement
No competing financial interests exist.